Pharmacologic pitfalls in heart failure: A guide to drugs that may cause or exacerbate heart failure. A European Journal of Heart Failure expert consensus document
Amr Abdin, Johann Bauersachs, Magdy Abdelhamid, Suleman Aktaa, Hussam Al Ghorani, Antonio Bayes‐Genis, Jan Biegus, Michael Böhm, Javed Butler, Nicolas Girerd, Marco Metra, Wilfried Mullens, Hadi Skouri, Muthiah Vaduganathan, Seif El Hadidi, Giuseppe M.C. Rosano

TL;DR
This paper identifies medications that can worsen heart failure and provides guidance for clinicians to avoid harmful drug use in patients with heart failure.
Contribution
The paper offers a comprehensive, expert consensus on drugs that may cause or exacerbate heart failure, emphasizing clinical scenarios and management strategies.
Findings
Several drug classes, including antidiabetic agents and antiarrhythmics, may worsen heart failure.
Clinicians should review medication regimens to avoid iatrogenic harm in heart failure patients.
Individualized therapy and close monitoring are emphasized to prevent drug-induced deterioration.
Abstract
Heart failure (HF) exerts a global health burden, often complicated by polypharmacy due to the frequent coexistence of cardiovascular and non‐cardiovascular comorbidities. While guideline‐directed medical therapy and devices have significantly improved outcomes, a range of commonly prescribed medications may inadvertently worsen HF or precipitate decompensation. This expert consensus statement provides a comprehensive overview of drugs known to cause or exacerbate HF, offering practical guidance for clinicians to identify and avoid harmful pharmacologic exposures in this vulnerable population. The review examines the pathophysiological mechanisms, clinical evidence, and guideline‐based recommendations for several drug classes, including antidiabetic agents (e.g. thiazolidinediones, dipeptidyl peptidase‐4 inhibitors), antiarrhythmics (particularly Class I and III), calcium channel…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7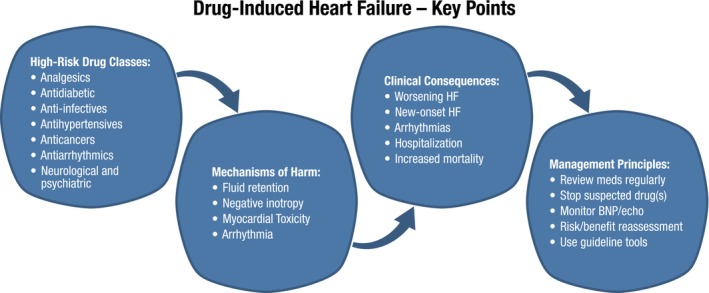 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10 Figure 11
Figure 11 Figure 12
Figure 12 Figure 13
Figure 13 Figure 14
Figure 14 Figure 15
Figure 15 Figure 16
Figure 16 Figure 17
Figure 17 Figure 18
Figure 18 Figure 19
Figure 19 Figure 20
Figure 20 Figure 21
Figure 21 Figure 22
Figure 22 Figure 23
Figure 23 Figure 24
Figure 24 Figure 25
Figure 25 Figure 26
Figure 26 Figure 27
Figure 27 Figure 28
Figure 28 Figure 29
Figure 29 Figure 30
Figure 30 Figure 31
Figure 31 Figure 32
Figure 32 Figure 33
Figure 33 Figure 34
Figure 34 Figure 35
Figure 35 Figure 36
Figure 36 Figure 37
Figure 37 Figure 38
Figure 38 Figure 39
Figure 39 Figure 40
Figure 40 Figure 41
Figure 41 Figure 42
Figure 42 Figure 43
Figure 43 Figure 44
Figure 44 Figure 45
Figure 45 Figure 46
Figure 46 Figure 47
Figure 47 Figure 48
Figure 48 Figure 49
Figure 49 Figure 50
Figure 50Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Cardiac Fibrosis and Remodeling · Diabetes Treatment and Management