Leadership Lessons From a Quality Improvement Project to Decrease the Avoidable Days in the Hospital Related to Decision-Making Capacity
Hira Fatima, Syed Atif, Bella Ayala, Zorez R Mian, Sobia Zareen, Erum Azhar, Abdul Waheed

TL;DR
This study shows how implementing a structured decision-making capacity assessment tool and leadership changes can reduce avoidable hospital days.
Contribution
The study introduces a multifaceted intervention combining the U-CARE tool and leadership strategies to reduce avoidable hospital days.
Findings
The U-CARE tool and bundled intervention were associated with a reduction in avoidable days.
Leadership changes significantly impacted the outcomes of the quality improvement project.
Many physicians lacked awareness and use of standardized capacity assessment tools prior to the intervention.
Abstract
Introduction: Extended hospital stays drive up costs for patients, payors, and health systems. For this reason, it is crucial to minimize “avoidable days” (ADs), or delays to discharge after a patient is medically stable. Delays in determining decision-making capacity are a significant contributor to ADs. The present study implemented the U-CARE tool - a structured, evidence-informed capacity assessment instrument that provides a standardized framework for evaluating understanding, choice, appreciation, and reasoning. The tool requires brief clinician training and has been used in prior hospital-based quality improvement initiatives to improve consistency in capacity evaluations. We introduced U-CARE as part of a multifaceted bundled intervention to decrease ADs at a community hospital in Lebanon, Pennsylvania. Methods: A quasi-experimental pre-post intervention study was conducted,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
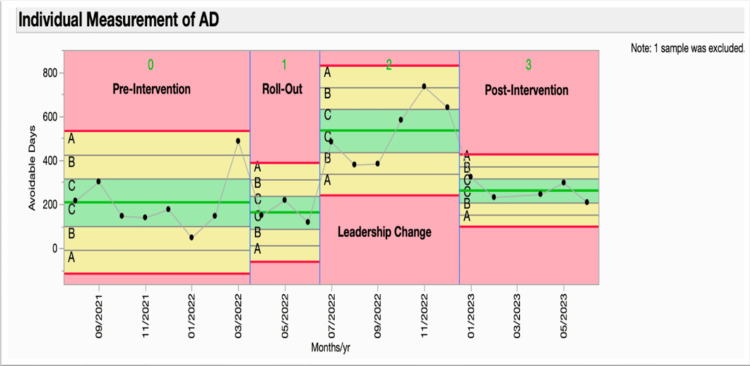 Figure 1
Figure 1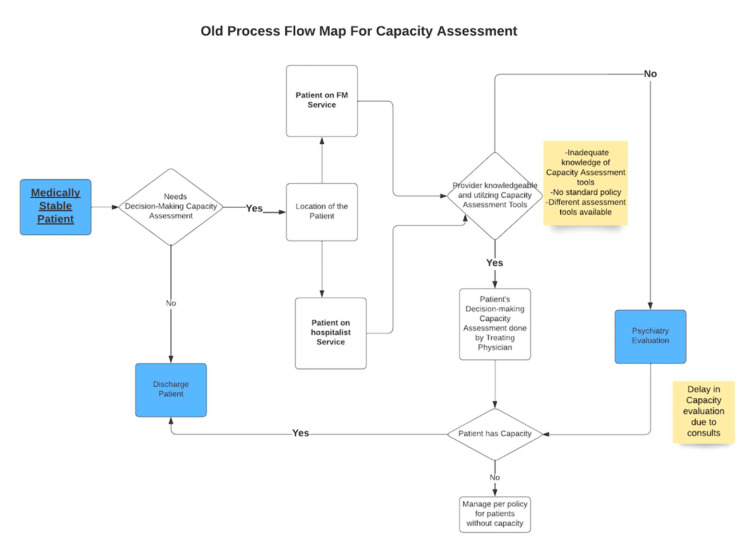 Figure 2
Figure 2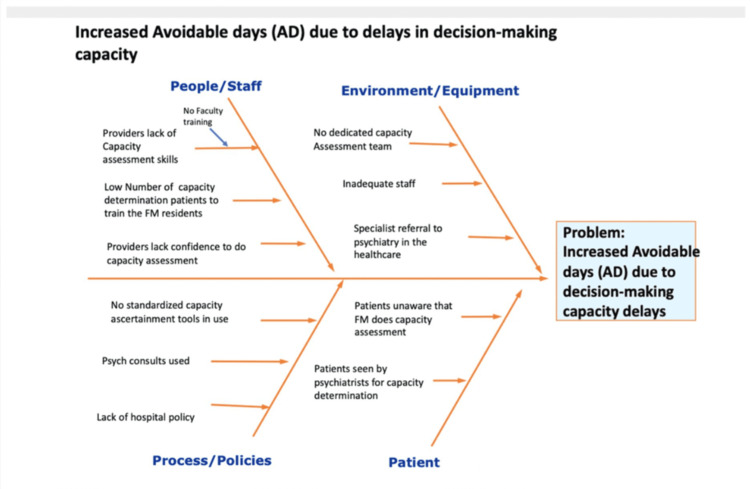 Figure 3
Figure 3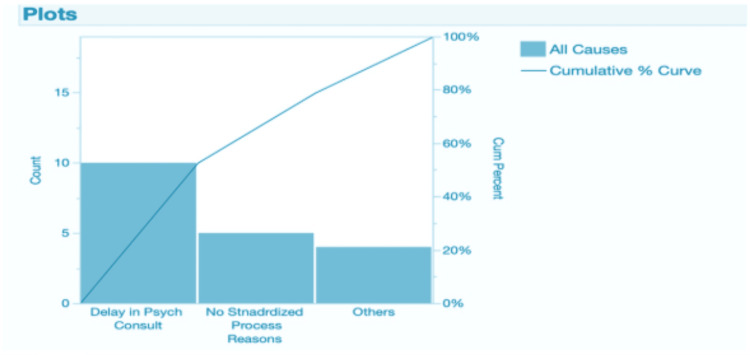 Figure 4
Figure 4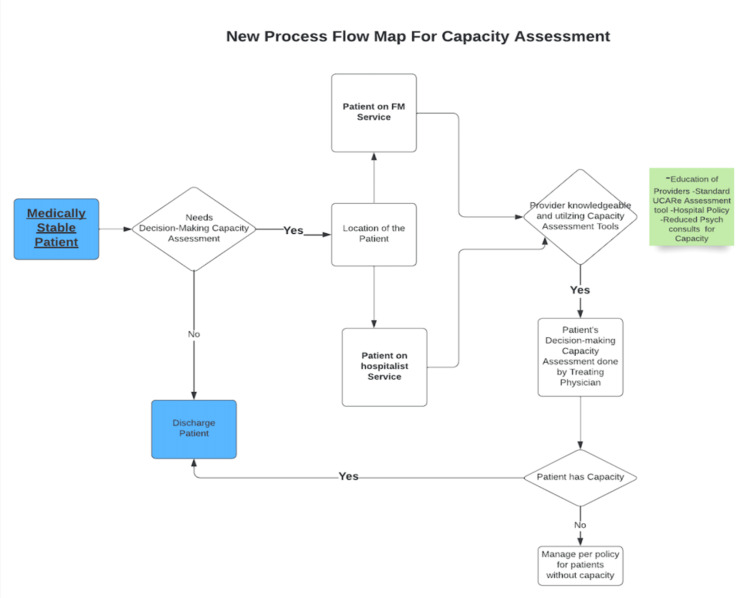 Figure 5
Figure 5| Analysis of Variance | |||||
| Source | DF | Sum of Squares | Mean Square | F Ratio | Prob > F |
| Intervention | 3 | 460,478.29 | 153,493 | 11.4010 | 0.0002* |
| Error | 18 | 242,336.30 | 13,463 | ||
| C. Total | 21 | 702,814.59 | |||
| Means for Oneway ANOVA | |||||
| Level | Number | Mean | Std Error | Lower 95% | Upper 95% |
| 0 | 8 | 208.250 | 41.023 | 122.06 | 294.44 |
| 1 | 3 | 162.667 | 66.990 | 21.93 | 303.41 |
| 2 | 6 | 534.333 | 47.369 | 434.81 | 633.85 |
| 3 | 5 | 261.800 | 51.891 | 152.78 | 370.82 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Policy Implementation Science · Hospital Admissions and Outcomes · Nursing education and management
Introduction
Hospital length of stay (LOS) is a crucial indicator of system performance, directly linked to costs, bed availability, and patient outcomes. Prolonged LOS is associated with higher risks of hospital-acquired complications, functional decline, and readmissions, while also congesting flow from the emergency department (ED) and limiting access for incoming patients. Common drivers include patient factors (age, comorbidity, functional and cognitive status), care-process issues (diagnostic/treatment delays, complications), and system barriers (discharge-planning gaps, post-acute placement delays, and care-coordination failures). Large reviews consistently identify discharge bottlenecks, especially arranging post-acute services and social supports, as major contributors to extended stays [1-3].
Within this broader context, Majeed et al. [1] define avoidable days (ADs) as inpatient days that occur after a patient is medically stable but remains hospitalized due to non-medical delays. ADs commonly stem from placement or insurance authorization delays, transportation issues, and workflow/communication gaps. Importantly, decision-making capacity (DMC) uncertainty can also stall discharge: when a patient’s ability to understand, appreciate, reason about, and express a choice is unclear, teams may defer to psychiatry or legal processes, pathways that are not scalable for every case and can add days to LOS [4].
The ethical stakes are high; clinicians must balance respect for autonomy with the duty to protect vulnerable patients. Appelbaum outlines DMC across four abilities: communicating a choice, understanding relevant information, appreciating the consequences, and reasoning about options [5]. It cautions against relying on global cognitive screens like the Mini-Mental State Examination (MMSE), as no single cutoff provides adequate sensitivity and specificity for capacity determinations. Consistent with this, Grisso and Appelbaum [6] advocate a structured bedside approach grounded in these abilities rather than cognition scores alone; empirical work also shows that MMSE is an imprecise discriminator for DMC [7].
Published outcome studies isolating Understanding, Consistency, Appreciation, Reasoning, Expression (U-CARE) specifically are limited; peer-reviewed work more commonly evaluates closely related Understanding, Appreciation, Reasoning, Expression (U-ARE) protocols derived from the same four-abilities framework. In memory-care and research settings, U-ARE has been associated with more efficient, standardized capacity assessments and with “capacity optimization” strategies (e.g., communication aids) that preserve autonomy [8]. In long-term care and community practice, descriptive quality improvement (QI) reports using U-CARE-style checklists echo these benefits, clearer bedside documentation and faster team consensus even though controlled trials remain scarce [4,5].
Finally, because implementation succeeds or fails at the team level, we incorporated multidisciplinary rounds (MDR) prompts and shared accountability. Evidence from a Cochrane review by Silva and colleagues indicates that collective leadership approaches can improve professional practice and healthcare outcomes, supporting the leadership and teamwork elements embedded in our intervention [9].
The present study implemented a pragmatic capacity-assessment approach using the U-CARE/U-ARE framework (a structured bedside method aligned with the four abilities) and bundled system supports (education, auditing/reminders, and MDR prompts). The objective of this project was to evaluate whether a structured U-CARE-based workflow could reduce ADs related to these delays at a community hospital in Lebanon, Pennsylvania.
Materials and methods
Study design and setting
A quasi-experimental pre-post quality‐improvement study was conducted at a community hospital in Lebanon, Pennsylvania. Monthly ADs were tracked across three phases: pre-intervention (August 2021-June 2022), roll-out (June-September 2022), and post-intervention (September 2022-June 2023). The project was reviewed by the institution and determined to be a quality improvement, exempt from IRB oversight.
Study population
The cohort included all adult inpatients on hospitalist services for whom ADs are routinely recorded by case management using the hospital’s operational definition (days spent in hospital after medical stability until discharge). In addition to overall ADs, a subset of ADs attributed to capacity-related delays was identified from case-management annotations and MDR notes.
Pre-intervention
A pre-intervention baseline of monthly ADs (see Figure 1) and a pre-intervention process map of the existing DMC workflow (see Figure 2) were developed to identify failure points and handoffs.
Trends in avoidable days (ADs)Statistical process control (SPC) phase analysis control chart tracking the scholarly activities completed by individual residents, divided into Pre-intervention (0) and Post-intervention (1) phases separated by the (blue) intervention line. μ0 represents the mean as the center green line. UCL (upper red line): three sigma upper control limit. LCL (lower red line): three-sigma lower control limit. Values in UCL and LCL represent three standard deviations above and below the mean, respectively. Special cause variation is highlighted in red with the Nelson rule number 1 and a change in the mean from the pre-intervention to the post-intervention phase.UCL: upper control limit, LCL: lower control limit
Baseline Process MapFM = Family Medicine
A root cause analysis (RCA) was conducted using an Ishikawa (fishbone) diagram with representation from hospital medicine, family medicine residency, case management, nursing leadership, and social work (see Figure 3). Contributing factors were organized under People, Policies, Procedures, Environment, and Communication/Information flow. Outputs from the RCA informed intervention selection and the Knowledge, Attitudes, and Practices (KAP) survey content.
Root Cause AnalysisFM = Family Medicine
A cross-sectional KAP survey was administered to attending physicians and residents on inpatient services, achieving a 100% response rate (n=32). Survey domains included 1) Knowledge: awareness of capacity frameworks/tools (e.g., U-CARE), familiarity with Appelbaum’s four abilities; 2) Attitudes: perceived difficulty of DMC evaluations; beliefs about the role of psychiatry/courts; perceived ethical risks (autonomy vs protection); and 3) Practices/Barriers: current use of any standardized tool; turnaround times for psychiatry consults; presence/clarity of local policies; documentation practices.
Results were summarized descriptively (proportions) and visualized with a Pareto chart to identify the “vital few” drivers (see Figure 4). Key pre-intervention findings informing the intervention included: high self-reported challenge with DMC evaluation (87.5%), low use of any capacity tool (61.5% not using one), limited awareness of U-CARE (42.3% unaware), and dominant barriers of psych consult delays (≈48%) and lack of a standardized process (≈45%).
Pareto Chart from the Baseline Knowledge, Attitudes, and Practices (KAP) Survey
Intervention
The present study introduced a multifaceted intervention centred on a structured bedside framework labelled U-CARE (Understanding, Consistency, Appreciation, Reasoning, Expressing a choice).
Education
The Director of Hospital Medicine provided education sessions for all attendings and residents on the U-CARE approach and expectations for bedside assessment and documentation.
Audit and Feedback
Case managers conducted weekly chart audits of open cases with ADs and sent targeted reminders to the hospitalist of record regarding capacity-related delays.
Workflow Prompt
MDR adopted a scripted inquiry about ADs and DMC status to prompt timely application of U-CARE and escalation only when needed.
Process fidelity was monitored by logging delivery of education sessions, completion of weekly audits, and MDR prompt uptake.
Data collection and analysis
Data were collected on outcome measures (ADs during various phases) and process measures (a three-part intervention). Statistical Process Control (SPC) was used to display and monitor ADs over time. Monthly ADs were plotted using an Individuals (XmR) chart, a type of SPC chart used to track individual data points over time, in JMP® Pro 19 (JMP Statistical Discovery LLC, Cary, NC, USA). Institute for Healthcare Improvement (IHI) special-cause rules were applied to detect non-random variation (e.g., shifts, trends) and to recalculate centerlines/control limits when indicated. For phase-level comparisons, we conducted a one-way ANOVA of monthly AD means across the three phases (α = 0.05). Analyses focused on both overall ADs and capacity-attributable ADs where available.
Results
The post-intervention process map (Figure 5) illustrates the redesigned bedside pathway for DMC. It includes an early U-CARE prompt at the point of clinical stability, clear documentation expectations, and a scripted MDR check to identify capacity-related barriers before ADs accrue. Compared with the baseline map (Figure 2), redundant handoffs were removed and escalation criteria clarified.
Post-implementation Process MapFM = Family Medicine; MDR = Multidisciplinary Rounds; U-CARE = Understanding, Consistency, Appreciation, Reasoning, Expressing a Choice.
The pre-intervention baseline period demonstrated that mean ADs were 208 per month (Figure 1). This value functioned as the reference centerline on the statistical process control (SPC) chart and provided a benchmark against which subsequent phase changes were evaluated.
The initial implementation period showed an immediate beneficial effect of the bundled intervention. During Phase 1, mean ADs decreased to 163 per month, representing a reduction of 45 days and a 21.6% improvement compared with baseline. In the Individuals (XmR) SPC chart, Phase-1 values consistently fell below the baseline centerline and met Institute for Healthcare Improvement special-cause criteria, prompting recalculation of the centerline. This reduction corresponded with the period in which education sessions, weekly case-management audits, and MDR prompts were most consistently executed, aligning with the optimized workflow illustrated in Figure 5.
The subsequent leadership transition period was associated with a marked deterioration in performance. During Phase 2, mean ADs increased to 534 per month the highest level observed across all phases. This increase represented a rise of 371 ADs compared with Phase 1 (+227.6%) and 326 ADs compared with baseline (+156.7%). The SPC chart displayed a clear upward level shift with rule-based evidence of special cause variation, indicating that the change in hospital medicine leadership corresponded with a substantial disruption in the implementation of standardized processes.
The period following leadership re-engagement demonstrated partial stabilization and improvement. During Phase 3, mean ADs decreased to 262 per month, which was 272 lower than the Phase-2 peak (-50.9%). Although performance improved, ADs remained 54 above baseline (+26.0%) and 99 above the Phase-1 mean (+60.7%). The XmR chart reflected a downward shift consistent with restoration of partial process control, though not a full return to the initial gains achieved during early implementation.
The survey-observed mechanisms provided insight into the drivers underlying these trends. Before implementation, the KAP survey (Figure 4) showed that most clinicians found capacity assessment challenging (87.5%), did not use a formal assessment tool (61.5%), and were unaware of U-CARE (42.3%). The Pareto chart identified delays in psychiatry consultation (48%) and the absence of a standardized workflow (45%) as the most influential contributors to capacity-related ADs. Additionally, the fishbone diagram (Figure 3) highlighted gaps in policy clarity, documentation variability, and communication flow all issues directly addressed by the intervention components.
The comparison of mean ADs across phases demonstrated a statistically significant difference. A one-way ANOVA yielded an F value of 11.4 (p < 0.05) (Table 1), confirming that the observed variation across phases was unlikely due to chance. The direction and magnitude of changes initial reduction, subsequent deterioration with leadership turnover, and partial recovery with leadership engagement support the interpretation that the intervention was effective when supported by stable leadership, but vulnerable to disruption when leadership continuity was interrupted.
Discussion
Our intervention demonstrated that a bundled strategy incorporating the U-CARE decision-making capacity workflow, audit and feedback, and MDR team-based inpatient care meetings was associated with an initial reduction in ADs. Following a transition in hospital medicine leadership, ADs increased beyond baseline, then declined again after the new leader re-engaged with the work. This pattern highlights the central role of consistent leadership involvement in sustaining quality improvement efforts and maintaining reductions in ADs. Suggestive of two complementary insights: (1) structured capacity tools can reduce avoidable delays, and (2) leadership continuity and institutional embedding are critical to sustain those gains.
Majeed et al. [1] showed that delays, often unrelated to ongoing medical care, inflate bed occupancy and prolong stays. Broader work by Allen et al. [10]. highlighted delays to placement barriers, fragmented coordination, and process inefficiencies. In a systematic review Cadel et al. [2] reported that discharge facilitation and patient-tracking systems can help in reducing delays, but their effectiveness was contingent on organizational commitment and leadership support. Broader analyses by Abdelhalim et al. [11] concluded that delayed discharge persists because of structural barriers, leadership gaps, and weak cross-setting integration. Studies indicate that nearly 6% of internal medicine inpatients experienced delayed discharge, with contributions from dependence in ADLs and hospital-acquired complications [12]. Delayed discharge has been closely linked to overall hospital length of stay and call for hospital process improvements paired with post-acute capacity [13].
Decision-making capacity represents a specific discharge clinical barrier. Appelbaum’s “four abilities” model, understanding, appreciation, reasoning, and expressing a choice remains the dominant clinical framework [5]. Expansions on this model have linked these domains to their legal and ethical roots, highlighting the importance of structured assessment in clinical practice [14]. Global cognitive screens are insufficient for capacity: Kim and Caine showed the MMSE lacks sensitivity for assessing appreciation and reasoning, leading to misclassification [7]. To operationalize the abilities at the bedside, U-ARE offers a pragmatic, stepped approach; Hamilton et al. reported more efficient, standardized assessments and “capacity optimization” tactics that preserve autonomy [8]. Our Phase-1 AD reduction is consistent with these data: embedding a structured, ability-based method (here, U-CARE-aligned) reduced uncertainty, standardized documentation, and surfaced barriers earlier in MDR.
The Phase-2 spike coincided with leadership turnover, then improved with leader re-engagement, mirroring evidence that leadership behavior shapes patient safety and quality, and that performance erodes when sponsorship lapses [14,15]. Collective leadership approaches further show gains in professional practice, outcomes, and staff well-being [16]. In Kotter’s terms, Phase-1 reflected urgency, a guiding coalition (director, case management, MDR), and short-cycle wins; turnover disrupted that coalition, and Phase-3 recovery followed re-forming it. Healthcare applications of Kotter’s 8-step model similarly associate explicit attention to coalition-building, barrier removal, and anchoring in culture with improved adoption and sustainment [17-19].
Finally, beyond DMC workflows, hospital medicine leadership influences LOS. Program evaluations and reviews link hospitalist models, paired with reliable discharge planning and daily multidisciplinary goal setting, to shorter LOS and better satisfaction [20-23]. Our bundle operationalized those principles (MDR scripts, closed-loop audits, standard work), and loss then restoration of visible leadership tracked closely with AD performance.
For organizations adopting U-CARE/U-ARE-style capacity pathways, pair the technical change with a leadership-proof sustainment plan: (i) anchor a Kotter-style guiding coalition beyond a single leader; (ii) hard-wire MDR prompts and documentation standards; (iii) maintain a shared LOS/AD dashboard owned by hospital medicine and case management; and (iv) monitor capacity-attributable ADs to verify mechanism and target coaching. Standardization reduces variation; stable, engaged leadership keeps the gains.
This quality improvement project has several limitations. First, the observed association between leadership presence and reductions in ADs may be influenced by unmeasured confounders, such as concurrent workflow changes, staffing patterns, or seasonal variation in patient volume. Second, the project was conducted at a single community hospital, which may limit generalizability to other settings with different resources, structures, or decision-making processes. Finally, the pre-post design does not allow for causal inference. Despite these limitations, the findings suggest that formal leadership involvement plays an important role in sustaining improvements in discharge processes and reducing ADs.
Conclusions
Formal leadership presence is significantly associated with outcomes in this quality improvement project. The U-CARE tool has the potential to reduce ADs by allowing hospitalists to determine decision-making capacity without a psychiatry consult. The benefits of eliminating ADs would be experienced by healthcare systems, payors, and patients alike.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delay in discharge and its impact on unnecessary hospital bed occupancy BMC Health Serv Res Majeed MU Williams DT Pollock R Amir F Liam M Foong KS Whitaker CJ 4101220122316765610.1186/1472-6963-12-410PMC 3511236 · doi ↗ · pubmed ↗
- 2Initiatives for improving delayed discharge from a hospital setting: a scoping review BMJ Open Cadel L Guilcher SJ Kokorelias KM Sutherland J Glasby J Kiran T Kuluski K 011202110.1136/bmjopen-2020-044291 PMC 788011933574153 · doi ↗ · pubmed ↗
- 3Defining delayed discharges of inpatients and their impact in acute hospital care: a scoping review Int J Health Policy Manag Micallef A Buttigieg SC Tomaselli G Garg L 1031111120223261082210.34172/ijhpm.2020.94PMC 9278600 · doi ↗ · pubmed ↗
- 4You let them do what??!!: Decision-making capacity and the exercise of patient autonomy in LTCJ Long Term Care Ferrini R Gibson RM 2010 https://www.hmpgloballearningnetwork.com/site/altc/content/you-let-them-do-what-decision-making-capacity-and-exercise-patient-autonomy-ltc
- 5Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med Appelbaum PS 1834184035720071797829210.1056/NEJ Mcp 074045 · doi ↗ · pubmed ↗
- 6Assessing Competence to Consent to Treatment: A Guide for Physicians and Other Health Professionals Grisso T Appelbaum PS New York Oxford Academic 1998 https://books.google.ca/books?hl=en&lr=&id=krcky Cid Sug C&oi=fnd&pg=PA 1&dq=Assessing+Competence+to+Consent+to+Treatment:+A+Guide+for+Physicians+and+Other+Health+Professionals&ots=147tx Xi A Qp&sig=Rh GQ 5Wp 8iy Z 1U Um 3HFM 4nfn NZ Uo&redir_esc=y#v=onepage&q=Assessing%20Competence%20to%20Consent%20to%20Treatment%3A%20A%20Guide%20for%20Physicians%20and%20Other%20Heal
- 7Utility and limits of the Mini Mental State Examination in evaluating consent capacity in Alzheimer's disease Psychiatr Serv Kim SY Caine ED 132213245320021236468610.1176/appi.ps.53.10.1322 · doi ↗ · pubmed ↗
- 8The U-ARE protocol: a pragmatic approach to decisional capacity assessment for clinical research J Alzheimers Dis Hamilton RK Phelan CH Chin NA 4314427320203186866310.3233/JAD-190457 PMC 7388558 · doi ↗ · pubmed ↗