A Case of Cryptococcal Meningitis in an Immunocompetent Individual
Elodie Baumgartner, Lexi Weltin, John J Farrell

TL;DR
A 49-year-old immunocompetent man was diagnosed with cryptococcal meningitis after initial misinterpretation of his symptoms and imaging.
Contribution
This case highlights the diagnostic challenges of cryptococcal meningitis in immunocompetent individuals and the need for heightened suspicion.
Findings
Cryptococcal meningitis was confirmed via cerebrospinal fluid evaluation despite initial imaging suggesting a cerebrovascular accident.
The patient's symptoms improved with antifungal therapy and intracranial pressure management.
The case emphasizes the importance of considering fungal meningitis in non-immunocompromised patients.
Abstract
Cryptococcal meningitis is classically associated with immunocompromised hosts but can also occur in individuals without identifiable immune dysfunction. Its nonspecific and often indolent presentation may delay diagnosis, particularly when early neuroimaging suggests alternative etiologies. We report a case of a 49-year-old immunocompetent man who presented with progressive headaches, sensory changes such as transient hearing loss, visual changes, and balance issues. Initial imaging showed a hyperdense area on CT, which was interpreted as a possible cerebrovascular accident, delaying recognition of an infectious process. Cerebrospinal fluid (CSF) evaluation ultimately confirmed cryptococcal meningitis, and the patient improved with targeted antifungal therapy and intracranial pressure (ICP)-directed management. This case highlights diagnostic challenges in immunocompetent hosts and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
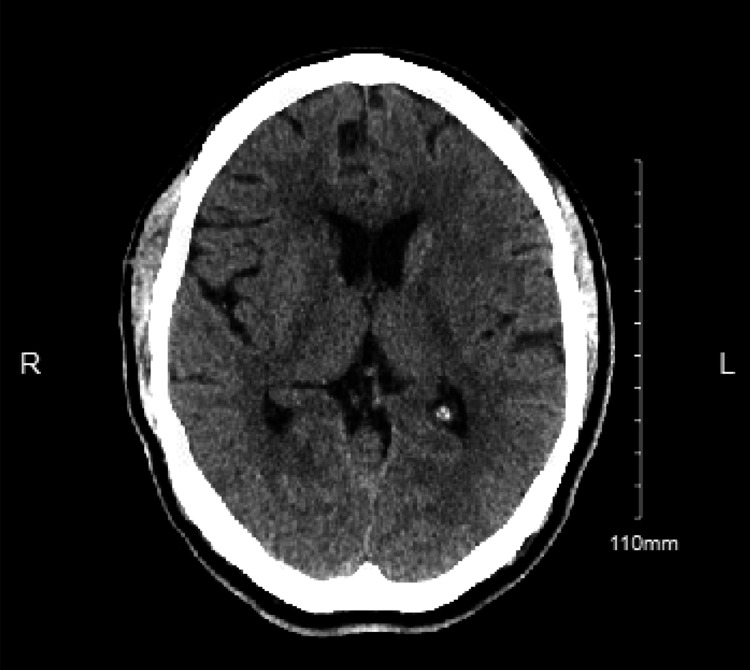 Figure 1
Figure 1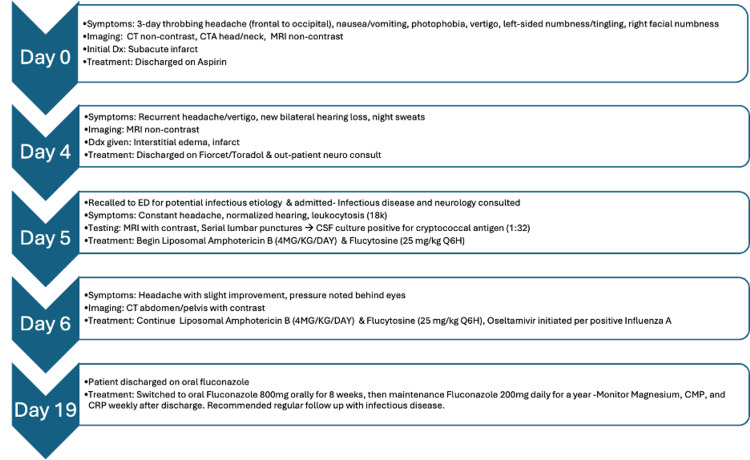 Figure 2
Figure 2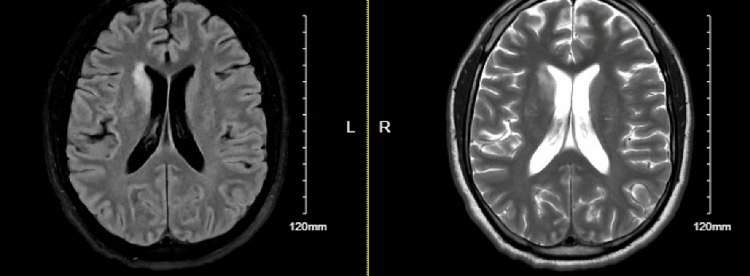 Figure 3
Figure 3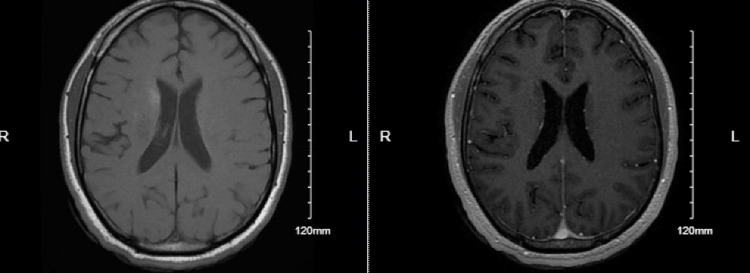 Figure 4
Figure 4| Test | Result | Reference Range |
| WBC | 14.47 (High) | 4.00-12.00 x 103/mcL |
| RBC | 5.46 | 4.40-5.80 x 106/mcL |
| HGB | 16.1 | 13.0-16.5 g/dL |
| HCT | 46.7 | 38.0-50.0% |
| MCV | 85.5 | 82.0-96.0 fL |
| MCH | 29.5 | 26.0-32.0 pg |
| MCHC | 34.5 | 31.0-36.0 g/dL |
| Platelet count | 349 | 140-440 x 103/mcL |
| RDW | 13.4 | 11.8-15.5 % |
| MPV | 9.5 | 8.0-12.6 fL |
| Neutrophils | 82.3 High | 40.0-68.0% |
| Lymphocytes | 12.0 Low | 19.0-49.0% |
| Monocytes | 4.6 | 3.0-13.0% |
| Eosinophils | 0.5 | 0.0-8.0% |
| Basophils | 0.6 | 0.0-1.0% |
| Absolute neutrophils | 11.91 (High) | 1.40-5.30 x 103/mcL |
| Absolute lymphocytes | 1.74 | 0.90-3.30 x 103/mcL |
| Absolute monocytes | 0.67 | 0.10-0.90 x 103/mcL |
| Absolute eosinophils | 0.07 | 0.00-0.50 x 103/mcL |
| Absolute basophils | 0.08 | 0.00-0.10 x 103/mcL |
| NRBC per 100 WBC | 0 | NA |
| Test | Result | Reference Range |
| WBC | 18.01 (High) | 4.00-12.00 x 103/mcL |
| RBC | 5.17 | 4.40-5.80 x 106/mcL |
| HGB | 15.4 | 13.0-16.5 g/dL |
| HCT | 44.9 | 38.0-50.0% |
| MCV | 86.8 | 82.0-96.0 fL |
| MCH | 29.8 | 26.0-32.0 pg |
| MCHC | 34.3 | 31.0-36.0 g/dL |
| Platelet count | 329 | 140-440 x 103/mcL |
| RDW | 13.8 | 11.8-15.5% |
| MPV | 10.0 | 8.0-12.6 fL |
| Neutrophils | 75.6 (High) | 40.0-68.0% |
| Lymphocytes | 18.0 (Low) | 19.0-49.0% |
| Monocytes | 5.7 | 3.0-13.0% |
| Eosinophils | 0.3 | 0.0-8.0% |
| Basophils | 0.4 | 0.0-1.0% |
| Absolute neutrophils | 13.61 (High) | 1.40-5.30 x 103/mcL |
| Absolute lymphocytes | 3.25 | 0.90-3.30 x 103/mcL |
| Absolute monocytes | 1.02 (High) | 0.10-0.90 x 103/mcL |
| Absolute eosinophils | 0.06 | 0.00-0.50 x 103/mcL |
| Absolute basophils | 0.07 | 0.00-0.10 x 103/mcL |
| NRBC per 100 WBC | 0 | NA |
| CSF Analysis | ||
| CSF culture | Cryptococcus neoformans | No growth (Sterile) |
| CSF glucose | 38 mg/dL | 40-70 mg/dL (~2/3 of serum glucose) |
| CSF protein | 70 mg/dL | 15-45 mg/dL (lumbar) |
| RBC count | 116/mm³ | 0 cells/µL (unless traumatic tap) |
| TNC count | 280/mm³ | 0-5 cells/µL (adults) |
| Differential: Neutrophils | 5% | 0-6% (adults) |
| Differential: Lymphocytes | 89% | 40-80% (adults) |
| Differential: Monocytes | 6% | 5-45% (adults) |
| CSF lactic acid | 3.9 mmol/L | 10-22 mg/dL (1.1-2.4 mmol/L) |
| CSF VDRL | Negative | Non-reactive (Negative) |
| CSF cryptococcus antigen qual. | Positive | Negative |
| CSF cryptococcus antigen quant. | 1:32 → 1:64 | <1:8 titer |
| Antimicrobial susceptibility (Yeast) | Cryptococcus neoformans | Sensitive/Intermediate/Resistant |
| Histoplasma/Blastomyces antigen | Not detected | Negative |
| CSF IgG Profile | ||
| CSF IgG index | 1.34 | 0.29-0.59 |
| CSF IgG | 13.6 mg/dL | 0.8-7.7 mg/dL |
| CSF albumin | 35.2 mg/dL | 8-32 mg/dL |
| CSF IgG/albumin | 0.39 | ≤0.27 |
| CSF IgG synthesis rate | 43.56 mg/24h | ≤3.3 mg/day |
| Serum IgG | 1,380 | 700-1,600 mg/dL |
| IgG/albumin (Serum) | 0.29 | 0.2-0.4 |
| Albumin quotient (CSF/Serum) | 7.33 | ≤0.007 |
| Serum Albumin | 4,800 | 3.5-5.0 g/dL |
| Infectious Disease Testing | ||
| Test | Result | Reference Range |
| West Nile Virus IgG & IgM | Negative | Negative (Non-reactive) |
| Herpes Simplex 1 & 2 PCR (CSF) | Negative | Negative (Non-reactive) |
| Lyme CNS infection IgG | Negative | Negative (Non-reactive) |
| Enterovirus PCR (CSF) | Negative | Enterovirus PCR (CSF): Negative (Not detected) |
| Lyme antibody | 0.13 | Lyme antibody: Negative (Non-reactive) |
| CMV IgG & IgM | Normal | Negative or positive (past infection) |
| Toxoplasma IgM | <3.0 (Normal) | Negative (Non-reactive) |
| Hep B surface antibody/core Ab | Negative | ≥10 mIU/mL (Protective) |
| Hep C antibody | Negative | Negative (Non-reactive) |
| Syphilis IgG/IgM | Negative | Negative (Non-reactive) |
| Quantiferon TB Gold | Normal | Negative (Non-reactive) |
| Hematologic/Inflammatory Markers | ||
| ESR | 12 mm/h | 0-20 mm/hr (varies by age/sex) |
| CRP | <0.10 mg/dL | <1.0 mg/dL (Low risk) |
| CBC: WBC | 18.01 x 10³/mcL | 4,000-11,000 cells/µL |
| CBC: ANC | 13.61 x 10³/mcL | 1,500-8,000 cells/µL |
| ANA screen | Negative titer | Negative (<1:40 titer) |
| ANCA IFA screen | Normal <1:20 | Negative |
| DHR flow cytometry (ANC) | 19,680 cells/mcL *Not consistent with CGD | ≥90% of control |
| CMP Component | Value | Reference Range |
| Sodium | 137 mmol/L | 136-145 mmol/L |
| Potassium | 4.4 mmol/L | 3.5-5.1 mmol/L |
| Chloride | 102 mmol/L | 98-107 mmol/L |
| CO₂ (Venous) | 24 mmol/L | 22-30 mmol/L |
| Anion gap | 11 mmol/L | <18 mmol/L |
| Glucose | 130 mg/dL (High) | 70-99 mg/dL |
| BUN | 16 mg/dL | 9-21 mg/dL |
| Creatinine | 0.99 mg/dL | 0.70-1.30 mg/dL |
| BUN/Creatinine ratio | 16 | 12-20 |
| Total protein | 6.4 g/dL | 6.0-8.0 g/dL |
| Albumin | 3.6 g/dL | 3.5-5.0 g/dL |
| A/G Ratio | 1.3 | 1.0-2.2 |
| Calcium | 9.0 mg/dL | 8.7-10.5 mg/dL |
| Total bilirubin | 0.3 mg/dL | 0.2-1.2 mg/dL |
| AST (SGOT) | 33 U/L | 6-42 U/L |
| ALT (SGPT) | 85 U/L (High) | 6-55 U/L |
| Alkaline phosphatase | 70 U/L | 40-150 U/L |
| Estimated GFR | >60 | ≥60 |
| Test Name | Result |
| AMPA-R AB CBA | Negative |
| Amphiphysin AB S | Negative |
| AGNA 1 S | Negative |
| ANNA 1 S | Negative |
| ANNA 2 S | Negative |
| ANNA 3 S | Negative |
| CASPR-IgG CBA S | Negative |
| CRMP 5 IGG | Negative |
| DPPX AB CBA S | Negative |
| GABA-B-R AB CBA S | Negative |
| GAD65 AB assay S | 0.02 (WNL) |
| GFAP IFA S | Negative |
| MGLUR1 AB IFA S | Negative |
| IgLON5 CBA S | Negative |
| LGI1-IGG CBA S | Negative |
| Neurochrongrin IFA S | Negative |
| NF IFA S | Negative |
| NMDA-R AB CBA S | Negative |
| PCA 1 | Negative |
| PCA 2 | Negative |
| PCA TR | Negative |
| PDEIS PDE10A AB IFA S | Negative |
| Septin-7 IFA S | Negative |
| T46IS TRIM46 AB IFA S | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Insects and Parasite Interactions
Introduction
Cryptococcus neoformans and C. gattii are true yeast that possess a prominent polysaccharide capsule that stains pink/red with mucicarmine but is impermeable to India ink and behave as opportunistic pathogens [1]. C. neoformans is associated with meningitis in immunocompromised individuals, particularly those with an HIV infection who have progressed to AIDS with a CD4 count below 100 cell/mL [2,3]. However, emerging evidence suggests that C. neoformans pneumonia and meningitis are occurring in immunocompetent patients more frequently [4,5]. Factors contributing to the rise in incidence of C. neoformans infections in immunocompetent individuals may include increasing human lifespans as well as expanding use of immune modulators in medical practice; but 20% of cases appear to be immune competent, some of whom were ultimately diagnosed with leukocyte adhesion deficiency (LAD) [5]. Cryptococcal meningitis is extremely difficult to treat due to the severe neurological sequelae, raised intracranial pressure (ICP), and immune reconstitution inflammatory syndrome (IRIS) [6].
The typical clinical presentation includes fever, headache, and photophobia, but classic signs associated with bacterial meningitis such as nausea and vomiting, and nuchal rigidity may not be present. Atypical manifestations such as acute cerebellar signs have been reported [3]. Neuroimaging usually does not inform the diagnostic workup. Although subtle MRI findings including leptomeningeal enhancement or dilated perivascular spaces may be present, CT imaging of the head is typically normal and findings of miliary nodules or frank ventriculitis are extremely rare [3]. Definitive diagnosis relies on cerebrospinal fluid (CSF) analysis, with CSF culture being the gold standard due to their high sensitivity and specificity [4]. Also, multiplex PCR panels (mPCR) of CSF are known to produce false negatives. The sensitivity of mPCR panels is significantly lower in patients with a low CSF yeast burden (e.g., <100 CFU/mL) [4].
This case report highlights cryptococcal meningitis in an immunocompetent patient, emphasizing its diagnostic challenges and the importance of maintaining a high index of suspicion even in the absence of classic risk factors.
Case presentation
A 49-year-old man with no past medical history and a family history of diabetes mellitus initially presented to the emergency department with three days of a throbbing frontal/occipital headache with associated nausea, vomiting, flashing lights, vertigo, and numbness and tingling of the left hand, left leg, and right face. At baseline, he works with heavy machinery and as a farmhand. At the initial presentation, CT of head/brain without contrast was ordered and revealed faint areas of hypodensity in the right head of the caudate nucleus, which were concerning lacunar infarcts (Figure 1). CT angiography of head was then ordered and revealed no large vessel occlusion. Subsequent MRI of brain demonstrated abnormal diffusion restriction of the bilateral corona radiata/centrum semiovale white matter and right caudate. Diffuse mild effusion and T2/fluid-attenuated inversion recovery (FLAIR) signal abnormality were also noted throughout the cerebellum. The patient was subsequently diagnosed with a cerebrovascular accident and was discharged with 300 mg aspirin daily and 50-325-40 mg Fioricet every four hours as needed.
Day 0 CT of head w/o contrast. Abnormal FLAIR signal in the right caudate and left basal ganglia, with corresponding diffusion restriction in the right caudate and bilateral corona radiata/centrum semiovale white matter. Some T2 shine through is noted involving the right caudate.FLAIR: Fluid-attenuated inversion recovery
Four days later, the patient returned to the emergency department with the same symptomatic headache and stated he had new onset bilateral hearing loss and no relief after taking the previously prescribed medications as needed (Figure 2). At this time, he was unsure of fevers but endorsed night sweats and demonstrated leukocytosis with an elevated white blood cell count on complete blood count (CBC) which was attributed to the inflammatory process of his stroke at the time (Table 1). Infectious etiology was low on the differential due to the patient not manifesting tachycardia or altered mental status. MRI did not indicate a stroke, but Neurology consult felt that continuing with secondary treatment for stroke was appropriate and that the hearing loss could be contributed to a potential past stroke.
Abbreviated timeline of eventsThis illustrates the main series of events leading to the diagnosis of cryptococcal meningitis. It highlights the most pertinent symptoms, labs/imaging, and treatments associated with this case.
A second MRI of the brain was ordered and was significant for an increased hyperintensity along the bilateral corona radiata right anterior caudate nucleus, dorsal left putamen, and bilateral cerebellar hemispheres (Figure 3). The increased signal on diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) maps indicate there is acute or subacute interstitial edema not caused by acute infarct. The patient experiencing headaches as well as the sensory deficits indicate elevated ICP, which can result in cerebral interstitial edema. Patient felt better on Toradol and was discharged at this time with Fioricet and Toradol for 2-4 days. Upon later review of the MRI by a new neurologist on shift, infectious etiology became a concern and the patient was recommended to get a lumbar puncture.
Day 4 MRI non-contrast Radiologic interpretation of increased hyperintensities in both ADC and DWI along the bilateral corona radiata right anterior caudate nucleus, dorsal left putamen and bilateral cerebellar hemispheres with an exception of a small area in the caudate. These imaging findings are consistent with acute or subacute interstitial disease. Differential includes inflammatory/post inflammatory, infectious/postinfectious, autoimmune, and PRES or demyelinating processes. DWI: Diffusion-weighted imaging; ADC: Apparent diffusion coefficient; PRES: Posterior reversible encephalopathy syndrome
The patient arrived at the tertiary care emergency department two days later and reported that the headache was still constant with relief only provided by ketorolac and that his hearing loss and numbness was only present when the headache was present. He also reports potential weight loss but is unsure of the amount of weight loss. He weighed 170 lbs at admission and 170 lbs a year prior. He denied recent travel outside of the United States and denied any sick contacts, shortness of breath, hemoptysis, dysuria, diarrhea, seizure history, or traumatic brain injury. At this time, the patient was ultimately admitted to the hospital for lumbar puncture and further work-up. On admission, the patient was hemodynamically stable with an elevated blood pressure of 141/98. CBC with differential demonstrated continued leukocytosis (Table 2). On physical examination, he demonstrated mild neck tenderness to palpation with an otherwise unremarkable exam including no focal neurological deficits.
A full workup was ordered, and Infectious Disease was consulted for the patient to determine any potential infectious causes of the patient’s persistent headaches. Lumbar puncture CSF studies revealed a low glucose of 38 mg/dL, high protein of 70 mg/dL, high total nucleated cell counts of 280 cm^3^, red blood cell (RBC) count of 116 cm^3^, 89% lymphocytes, 6% monocytes, 5% neutrophils, and an opening pressure of 29 cm H_2_O (Table 3). Other pertinent negative tests performed during the infectious workup include Negative West Nile virus antibody IgG and IgM, Lyme IgG with antibody reflex, CSF herpes simplex 1 and 2, CSF venereal disease, and enterovirus polymerase chain reaction (PCR) (Table 4).
Ultimately, with both the CSF culture and cryptococcal antigen screen the sensitivity is 98%. The patient’s CSF culture demonstrated *Cryptococcus neoformans. The *patient also demonstrated a positive Cryptococcus antigen screen and antigen titer of 1:32, which further confirmed the source of headaches and associated symptoms. At this time, induction therapy was started with liposomal amphotericin B at 4 mg/kg once daily and flucytosine 25 mg/kg every six hours. In the setting of no documented and verbalized past medical history, the patient underwent further testing to identify potential immune deficiency given his active Cryptococcus infection (Table 6). However, the studies done to assess immunocompromise were found to be inconclusive. He was hepatitis B surface antibody and core total antibody negative, hepatitis C antibody negative, syphilis IgG/IgM negative, quantiferon tuberculosis (TB) gold testing within normal limits (WNL), cytomegalovirus (CMV) IgG and IgM WNL, toxoplasma IgM antibody WNL, human immunodeficiency PCR test negative, and had a CD4 cell count of 641 cells/mm^3^. The patient did demonstrate an elevated absolute neutrophil count (ANC) of 19,680 cells/microliter on dihydrorhodamine (DHR) flow cytometric blood tests, but other values were WNL, and the results were not consistent with chronic granulomatous disease (CGD) or myeloperoxidase deficiency.
Thus, the patient did not have an identifiable source of immunocompromise despite having Cryptococcus neoformans induced meningitis.
As the patient started induction therapy, he continued to demonstrate significantly debilitating headaches while admitted despite additional symptomatic treatment. It was subsequently determined at that time that the patient would potentially benefit from serial lumbar punctures to reduce ICP with a goal opening pressure of around 25 cm H_2_O with symptomatic improvement. The repeat lumbar puncture demonstrated an increased opening pressure at 36 cm H_2_O from the initial 29 cm H_2_O. A repeat MRI of the brain demonstrated similar patchy areas of cerebral and cerebellar T2 FLAIR hyperintensity with corresponding intraparenchymal and leptomeningeal enhancement. It did not demonstrate lesions that were classic for cryptococcoses. A few days later, another Cryptococcus antigen titer came back at a value of 1:64, demonstrating potential improvement from the induction therapy but still the presence of an active infection. The patient concurrently demonstrated an improvement in symptomatic headaches. A third lumbar puncture was obtained given the previous elevated opening pressures. This lumbar puncture demonstrated an opening pressure of 27 cm H_2_O, thus achieving its goal with symptomatic improvement from his headaches with full resolution. The patient ultimately completed induction therapy and was transitioned to fluconazole 800 mg by mouth daily for eight weeks and then scheduled for 200 mg of fluconazole by mouth daily for one year total duration. One month after admission, the patient received a repeat MRI of the brain that demonstrated an overall improvement in areas of T2 prolongation with minimal residual enhancement (Figure 3). This imaging was consistent with the patient’s resolution of symptomatic headaches and neck tenderness.
One-month post treatment MRI non-contrast Radiology impression includes interval improvement in areas of T2 prolongation, which have enhancement in the parenchyma and leptomeninges within the bilateral cerebellar hemispheres and right basal nuclei in comparison with initial MRI of the brain. Minimal residual enhancement remains. No midline shift or uncal herniation are present. No new areas of abnormal enhancement within the cerebral or cerebellar parenchyma are present.
Discussion
C. neoformans is an encapsulated yeast that can be found in old pigeon droppings and can cause a spectrum of infections, ranging from asymptomatic airway colonization to severe disseminated disease or meningitis [7,8]. While immunocompromised individuals (e.g., HIV/AIDS patients with CD4 counts <100 cells/μL) are at highest risk, immunocompetent hosts may also develop progressive infections, particularly in the central nervous system [2,5]. Globally, cryptococcal meningitis causes an estimated 220,000 cases annually, with sub-Saharan Africa and Asia bearing the highest burden [4]. However, as seen in this case, sporadic infections occur even in seemingly healthy individuals.
Cryptococcal meningitis typically presents as subacute meningoencephalitis, with symptoms such as headache, altered mental status, fever, neck stiffness, nausea, and vomiting [2]. In HIV-positive patients, symptoms may be milder or nonspecific, whereas immunocompetent individuals often experience prolonged symptom duration (6-12 weeks) [5]. Visual disturbances (e.g., diplopia, photophobia) or hearing loss may occur due to elevated intracranial pressure (ICP) or cranial nerve involvement [3]. The 49-year-old immunocompetent man in this case presented with a three-day history of throbbing headache, nausea, vomiting, vertigo, and transient sensory deficits, initially misdiagnosed as a stroke. His symptoms persisted despite treatment, and he later developed bilateral hearing loss, a finding consistent with cryptococcal meningitis-related cranial nerve involvement [3]. His lymphocytic pleocytosis, elevated CSF protein (70 mg/dL), low glucose (38 mg/dL) and opening pressure of 29 cm H_2_O aligned with classic cryptococcal meningitis findings [2]. Notably, his ICP rose to 36 cm H_2_O during treatment, mirroring data where >50% of cryptococcal meningitis patients had ICP >25 cm H_2_O [3].
C. neoformans reproduces by budding, forming round yeast cells with a polysaccharide capsule that evades immune detection [6]. Diagnosis relies on CSF analysis, antigen testing, and culture. In this case, CSF culture confirmed C. neoformans, with a positive antigen titer (1:32) consistent with active infection despite the patient’s normal CD4 count (641 cells/mm³). This aligns with rare reports of cryptococcal meningitis in immunocompetent hosts [4,5]. First-line therapy for cryptococcal meningitis combines liposomal amphotericin B (4 mg/kg/day) and flucytosine (25 mg/kg Q6H) for induction, followed by fluconazole consolidation [4,9]. This regimen was initiated here, with symptomatic improvement after ICP reduction via serial lumbar punctures, a critical intervention given his rising pressure [3]. The patient responded well to therapy, with resolution of headaches and improved imaging after one month. His antigen titer declined to 1:64, suggesting treatment efficacy. However, his lack of identifiable immunodeficiency underscores the importance of considering cryptococcal meningitis even in immunocompetent patients with subacute neurological symptoms [4,5].
Mortality in cryptococcal meningitis can be attributed to the increase in ICP. The mechanism of raised ICP is thought to be due to the fungi obstructing CSF reabsorption leading to communicating hydrocephalus and eventually leading to herniation and death if not treated [10]. This also explains the interstitial edema seen early in the case as the raised ICP and communicating hydrocephalus can result in fluid being pushed into the periventricular space, seen as a hyperintensity on MRI. Multiple lumbar punctures to reduce ICP have been shown to decrease mortality [10]. In immunocompromised patients, in particular, raised ICP can be caused by immune reconstitution inflammatory syndrome. During HIV immune reconstitution with concomitant infection, the immune system has an exaggerated response resulting in an average mortality of 20% in this population [11]. This only occurs in 25% of patients with HIV but marks an important consideration when giving treatment [11].
While cryptococcal meningitis is classically HIV associated, this case reflects the rising recognition of cryptococcosis in immunocompetent populations. The optimal treatment duration for non-HIV patients remains unclear due to limited data, highlighting the need for inclusive clinical trials [4]. This case of cryptococcal meningitis in an immunocompetent patient challenges conventional clinical paradigms and offers critical insights that expand upon current literature. The patient was initially misdiagnosed with a stroke due to nonspecific MRI findings, illustrating how cryptococcal meningitis’s neuroimaging can overlap with ischemic stroke or demyelinating processes, potentially delaying diagnosis [2]. Early CSF analysis remains essential to ensure timely recognition and treatment of cryptococcal meningitis across all immune phenotypes.
Conclusions
This case demonstrates that CM should remain part of the differential diagnosis for subacute neurological symptoms even in immunocompetent individuals and when early imaging suggests alternative etiologies. Prompt CSF evaluation and timely initiation of antifungal therapy are critical for favorable outcomes. Clinicians should maintain a broad diagnostic perspective and consider fungal meningitis in patients with persistent or progressive neurological symptoms regardless of immune status.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis Clin Microbiol Rev Brouwer MC Tunkel AR van de Beek D 4674922320102061081910.1128/CMR.00070-09PMC 2901656 · doi ↗ · pubmed ↗
- 2HIV-associated cryptococcal meningitis AIDS Jarvis JN Harrison TS 211921292120071809003810.1097/QAD.0b 013e 3282 a 4a 64d · doi ↗ · pubmed ↗
- 3Cryptococcal meningitis: a review for emergency clinicians Intern Emerg Med Fisher KM Montrief T Ramzy M Koyfman A Long B 103110421620213342090410.1007/s 11739-020-02619-2 · doi ↗ · pubmed ↗
- 4Treatment of cryptococcal meningitis: how have we got here and where are we going?Drugs Ngan NT Flower B Day JN 123712498220223611234210.1007/s 40265-022-01757-5PMC 9483520 · doi ↗ · pubmed ↗
- 5Cryptococcal meningitis in apparently immunocompetent patients Crit Rev Microbiol Qu J Lv X 76865020243656273110.1080/1040841 X.2022.2159786 · doi ↗ · pubmed ↗
- 6Cryptococcus gattii meningitis complicated by immune reconstitution inflammatory syndrome in an apparent immunocompetent host in Malaysia Med Mycol Case Rep Chang CY Mohd Shah SH Lio JY Bahari N Radhakrishnan AP 143520223498416610.1016/j.mmcr.2021.12.004PMC 8693149 · doi ↗ · pubmed ↗
- 7Cryptococcosis today: it is not all about HIV infection Curr Clin Microbiol Rep O'Halloran JA Powderly WG Spec A 8895420172913002710.1007/s 40588-017-0064-8PMC 5677188 · doi ↗ · pubmed ↗
- 8Disseminated Cryptococcus in an immunocompetent patient due to prison yard pigeon exposure ID Cases Barvo M James N Ayyaz M 026202110.1016/j.idcr.2021.e 01285 PMC 846136834589412 · doi ↗ · pubmed ↗