Chronic Bicompartmental Bucket-Handle Meniscal Tears Associated With Anterior Cruciate Ligament (ACL) Rupture in an Epileptic Patient: A Case Report
Basil Alsuwaine, Rahaf Alrasheed, Suha Alanazi, Mohammed Alorayyidh, Ibrahim Assiri

TL;DR
A rare case of chronic meniscal tears and ACL rupture in an epileptic patient is presented, highlighting delayed diagnosis due to neurological issues.
Contribution
This case report presents a rare combination of chronic bicompartmental bucket-handle meniscal tears and ACL rupture in a patient with epilepsy.
Findings
MRI and arthroscopy confirmed bicompartmental bucket-handle meniscal tears and ACL rupture.
Neurological comorbidities likely delayed diagnosis and treatment.
ACL reconstruction was not performed due to reattachment and no instability.
Abstract
Bilateral bucket-handle meniscal tears (BHMTs) are uncommon, as these injuries are typically unilateral in a single knee and often associated with anterior cruciate ligament (ACL) tears. We present a rare case of a 36-year-old male with a history of intracerebral hemorrhage and epilepsy who developed chronic right knee pain, instability, and mechanical locking. MRI revealed ACL rupture and a displaced meniscal fragment. Arthroscopy confirmed bicompartmental BHMTs and ACL deficiency. Partial meniscectomy and debridement were performed. ACL reconstruction was not undertaken, as arthroscopy showed reattachment of the ligament, adequate graft tightness, and no clinical evidence of instability. ACL reconstruction was not performed due to adequate reattachment of the ACL. This case describes a rare presentation of chronic bicompartmental BHMTs with ACL rupture in a patient with underlying…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
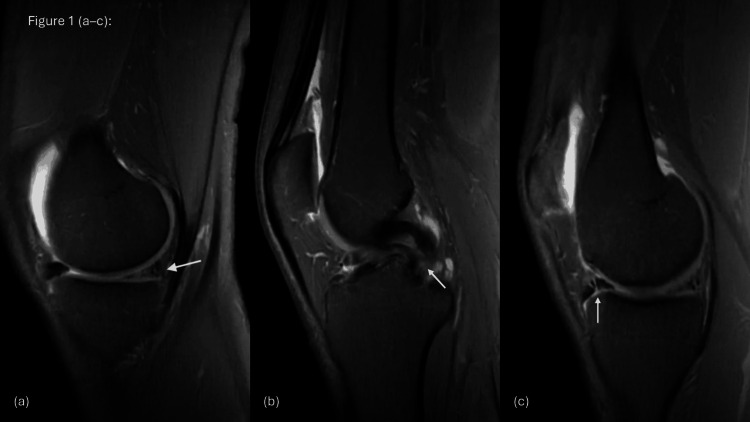 Figure 1
Figure 1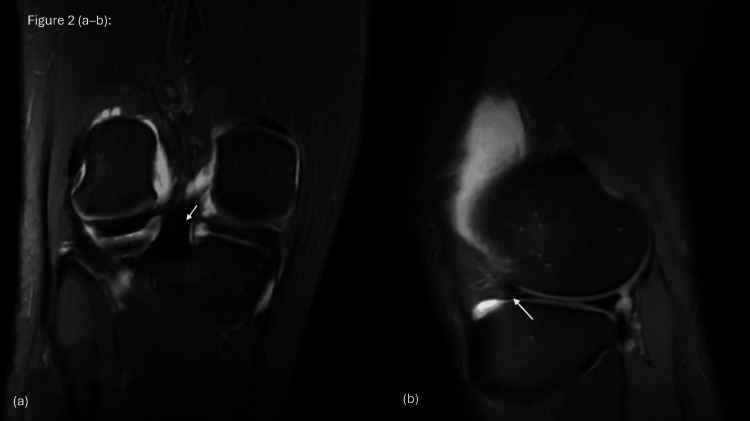 Figure 2
Figure 2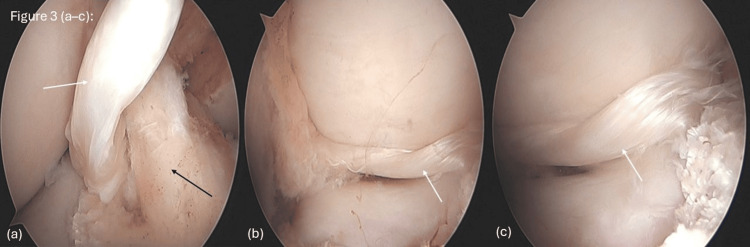 Figure 3
Figure 3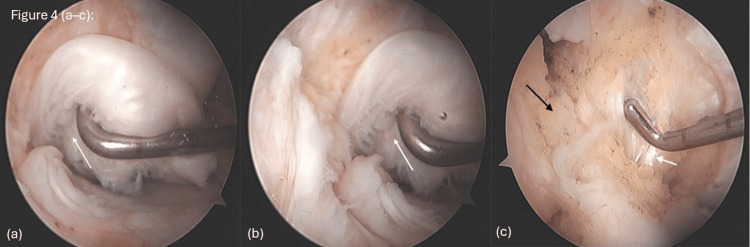 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Foot and Ankle Surgery · Orthopedic Surgery and Rehabilitation
Introduction
A bucket-handle meniscal tear (BHMT) is a vertical or oblique longitudinal tear in which a central meniscal fragment remains attached to the anterior and posterior horns but displaces toward the intercondylar notch, away from the peripheral rim [1]. It is highly prevalent in the setting of anterior cruciate ligament (ACL) tears; in 69.8% of cases, reflecting the substantial meniscal burden in this typically young, active population [2]. Meniscal tears are frequent, and the medial meniscus is affected approximately threefold more often than the lateral meniscus. Nevertheless, bicompartmental bucket-handle tears are documented in only about 30% of cases, representing a distinctly rare subtype of meniscal injury [3,4]. The knee menisci play a key biomechanical role in load distribution, shock absorption, joint stability, and lubrication; loss of meniscal tissue, particularly after subtotal or total meniscectomy, has been shown to accelerate degenerative changes and predispose to early osteoarthritis [5]. Clinically, meniscal tears usually present with localized joint-line pain, swelling or effusion, and mechanical symptoms such as catching, clicking, or true locking of the knee, especially during weight-bearing flexion and rotation [6]. The overarching aim of meniscal repair is to relieve symptoms while preserving native meniscal tissue in order to restore near-normal knee biomechanics and protect the articular cartilage [7]. We report a case of bicompartmental BHMT in a 36-year-old man, a presentation that has been rarely reported in the literature.
Case presentation
A 36-year-old right-leg-dominant man with a history of intracerebral hemorrhage, epilepsy, left-sided lower limb weakness, and bronchial asthma presented to our orthopedic clinic with progressive right knee pain and mechanical symptoms. Two months earlier, he had sustained a twisting injury to the right knee while walking. Since then, he reported new-onset medial knee pain associated with episodes of locking, during which the knee became stuck in flexion and required passive manipulation to extend. He denied acute swelling, redness, fever, constitutional symptoms, or recent seizures, with a previous right knee injury eight years earlier while playing football. At that time, he experienced pain, recurrent locking, and occasional giving-way episodes of the right knee but did not undergo imaging or surgical treatment. Symptoms partially improved after a course of physiotherapy, and he returned to his usual daily activities. For the last two years, he had resumed recreational football without instability until the recent twisting episode. At presentation, he was no longer participating in sports but was able to walk independently without assistive devices, although he remained limited by intermittent locking and pain.
On physical examination, he weighed 62 kg and ambulated with a non-antalgic gait. There was no obvious deformity or effusion of the right knee. Residual neurological deficits from his prior intracerebral hemorrhage were evident, with baseline weakness of the left lower limb. Manual muscle testing showed quadriceps strength of grade 4/5 on the right and 3/5 on the left. The right knee had full extension, with flexion reproducing medial joint-line discomfort, although no mechanical block was noted during the examination. There was localized tenderness along the medial joint line, but no warmth or joint erythema. Ligamentous assessment of the right knee revealed a stable joint with grade 1 anterior drawer and grade 1 Lachman tests, both with a firm endpoint, and no varus or valgus laxity. Distal neurovascular examination was intact.
The pre-operative magnetic resonance imaging (MRI) of the right knee (Figures 1A-1B) demonstrated a large longitudinal tear of the medial meniscus with a flipped fragment extending into the intercondylar notch, consistent with a bucket-handle tear (Figures 1A-1C). The ghost sign and double posterior cruciate ligament (PCL) sign were both observed (Figures 1B-1C). The lateral meniscus appeared intact (Figures 2A-2B). The cruciate ligaments showed a full-thickness ACL tear from the femoral attachment, while the PCL remained intact, with no anterior tibial translation. Minimal periligamentous edema was noted around the medial collateral ligament (MCL), indicating a grade I sprain, whereas the lateral collateral ligament (LCL) was unremarkable. The extensor mechanism, including the quadriceps tendon, patellar tendon, and Hoffa’s fat pad, was normal. Cartilage assessment demonstrated a mildly heterogeneous signal in the medial compartment, with preservation of the lateral and patellofemoral compartments.
Sagittal T2-weighted MRI showing (a) the ghost sign (white arrow), (b) the double posterior cruciate ligament (PCL) sign (white arrow), and (c) a displaced anterior horn fragment (white arrow).
MRI findings showing (a) coronal T2-weighted FSE FS images demonstrating a medial meniscus tear (white arrow), and (b) sagittal T2-weighted FSE FS images showing a lateral meniscus anterior horn tear (white arrow).FSE FS: fast spin-echo fat-suppressed
The patient underwent subtotal medial and lateral meniscectomy without concomitant ACL reconstruction because the ACL had become fibrotic and reattached to an abnormal location, and the patient had already adapted to this chronic condition.
The bucket-handle tears in both the medial and lateral menisci were confirmed on arthroscopy, with displaced fragments extending into the intercondylar notch (Figures 3A-3C). The degenerative nature of the meniscal tissue precluded repair, necessitating subtotal meniscectomy and joint debridement. Arthroscopic shavers and punches were utilized to remove unstable fragments and contour the remaining meniscal rims. In the lateral compartment, arthroscopy demonstrated a visible meniscus tear (Figure 3A), a bucket-handle configuration (Figure 3B), and a displaced fragment located within the intercondylar notch adjacent to the ACL (Figure 3C). In the medial compartment, a degenerative meniscal tear was observed (Figure 4A), along with a bucket-handle tear (Figure 4B). The ACL was reattached in a more inferior position at the femoral insertion, but intraoperative probing revealed good graft tightness, and thus ACL reconstruction was not performed (Figure 4C).
Images showing (a) a lateral meniscus tear (white arrow) with ACL (black arrow), (b) a bucket-handle tear in the lateral compartment (white arrow), and (c) a displaced lateral meniscus fragment in the notch (white arrow).ACL: anterior cruciate ligament
Images showing (a) a medial meniscus tear (white arrow), (b) a bucket-handle tear in the medial compartment (white arrow), and (c) ACL reattachment, with the ACL indicated by the black arrow and the PCL indicated by the white arrow.ACL: anterior cruciate ligament; PCL: posterior cruciate ligament
After surgery, early postoperative assessment showed a right knee range of motion from 0° to 130°. The patient reported overall improvement in his symptoms, although he continued to experience residual pain of about 5/10 on the visual analog scale. He began a supervised rehabilitation program at a private physiotherapy center, which included knee range-of-motion work, quadriceps and hamstring strengthening, neuromuscular training, and adjunctive shockwave therapy. On examination, the anterior drawer and Lachman tests remained grade 1 with a firm endpoint, similar to his preoperative findings, and the knee was clinically stable without any episodes of giving way. At his six-month follow-up, he noted mild but clear improvement in pain, complete resolution of locking, and no further instability during daily activities. He continued to walk independently without the need for assistive devices.
Discussion
Bilateral BHMTs with an ACL rupture are extremely rare, and this makes the diagnosis difficult, especially when the symptoms do not follow the usual pattern [1]. Our patient was a 36-year-old man who had delayed mechanical symptoms and left-sided neurological deficits. This is different from what has been reported in most cases, where patients typically present soon after injury with obvious locking and instability, as described by Yahyazadeh et al. [8] and Idrissi et al. [9]. In our case, the symptoms appeared almost a year after a secondary twisting event and six years after the original trauma, which contributed to the diagnostic delay.
MRI revealed classic signs of BHMTs, including the ghost sign and the double-PCL sign (Figures 1A-1C). These findings are consistent with what has been reported by Valderrama et al. [2] and Yahyazadeh et al. [8]. Sohail et al. [10] also highlighted the value of these signs, especially in acute injuries. However, similar to other reports, MRI did not fully demonstrate the chronic or complex aspects of the injury. The lateral meniscal tear, for example, was only clearly identified during arthroscopy (Figures 3A-3C), showing that imaging alone can sometimes miss important details.
During surgery, we performed a subtotal medial and lateral meniscectomy with joint debridement because the meniscal tissue was too degenerated to repair. This approach is similar to what was used in other chronic cases where repair was not possible [10,11]. In contrast, younger patients with acute injuries, as described by Bong and Lee [11] and Sohail et al. [10], were suitable for all-inside meniscal repair techniques.
We chose not to reconstruct the ACL because the patient had already adapted to the injury over several years, had neurological deficits, and did not participate in high-demand physical activities. This decision is supported by Wright et al. [12], who reported that partial meniscectomy alone can be enough in non-athletic patients who remain functionally stable despite ACL insufficiency.
The patient recovered well after surgery, began physiotherapy early, and did not experience any complications. His postoperative course is similar to what has been reported in other cases treated either surgically or conservatively [10,11].
Overall, this case shows that MRI has important limitations in chronic meniscal injuries and that arthroscopy remains essential for confirming the diagnosis and guiding management. It also demonstrates how neurological deficits can mask typical knee symptoms and delay diagnosis, and highlights the importance of tailoring treatment, especially decisions regarding ACL reconstruction, to the patient’s functional level, chronic adaptations, and overall condition.
Conclusions
Chronic bicompartmental BHMTs with ACL insufficiency are extremely uncommon, especially in patients with neurological conditions that may mask typical knee symptoms. In long-standing injuries where the meniscus cannot be repaired, partial meniscectomy can still provide meaningful improvement and acceptable short-term results. In this case, ACL reconstruction was not performed because intraoperative assessment showed that the knee remained relatively stable and the patient had functionally adapted over time. Overall, this case highlights the need for individualized treatment decisions and reinforces the important role of diagnostic arthroscopy in managing complex meniscal injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sagittal MR images of the knee: a low-signal band parallel to the posterior cruciate ligament caused by a displaced bucket-handle tear AJR Am J Roentgenol Weiss KL Morehouse HT Levy IM 1171191561991 https://ajronline.org/doi/abs/10.2214/ajr.156.1.1898543189854310.2214/ajr.156.1.1898543 · doi ↗ · pubmed ↗
- 2Prevalence of meniscal and articular surface injuries in patients undergoing primary and revision anterior cruciate ligament reconstruction: a retrospective analysis Cureus Valderrama J León A Hernández R 017202510.7759/cureus.85106 PMC 1220667240589699 · doi ↗ · pubmed ↗
- 3Prevalence and consequences of delayed diagnosis of anterior cruciate ligament ruptures Knee Surg Sports Traumatol Arthrosc Arastu MH Grange S Twyman R 120112052320152467138510.1007/s 00167-014-2947-z · doi ↗ · pubmed ↗
- 4Both medial and lateral bucket-handle meniscus tears associated with chronic ACL injury: a rare presentation of triple-PCL sign Int J Surg Case Rep Santoso A Poetera CY Marindratama H Anugrah JY Anwar IB Sibarani TS 1064138720213453752510.1016/j.ijscr.2021.106413 PMC 8449230 · doi ↗ · pubmed ↗
- 5The basic science of human knee menisci: structure, composition, and function Sports Health Fox AJ Bedi A Rodeo SA 340351420122301610610.1177/1941738111429419 PMC 3435920 · doi ↗ · pubmed ↗
- 6Meniscal tear: presentation, diagnosis and management Aust Fam Physician Shiraev T Anderson SE Hope N 182187412012 https://search.informit.org/doi/abs/10.3316/INFORMIT.15768044499189822472678 · pubmed ↗
- 7Bicompartmental locked bucket-handle tears of menisci concealing the concomitant anterior cruciate ligament injury for 2 years - a case report J Med Sci Zabrzynski J Szwedowski D Zabrzyńska A ŁapajŁ 225228302018 https://jms.ump.edu.pl/index.php/JMS/article/view/303
- 8Simultaneous medial and lateral bucket-handle meniscus tears in chronic ACL deficiency: a rare case of the triple-PCL sign J Res Orthop Sci Yahyazadeh H Haghbin M Elahifar O 161166102023 https://jros.iums.ac.ir/article-1-2253-en.pdf