Atopic dermatitis and fecundity: a Danish National Birth Cohort study
Camilla L Kjersgaard, Anne Gaml-Sørensen, Pernille J Clemmensen, Linn H Arendt, Siri E Håberg, Onyebuchi A Arah, Mette Deleuran, Cecilia H Ramlau-Hansen

TL;DR
Women with atopic dermatitis may have better fertility outcomes, as they conceive faster and use infertility treatments less than those without the condition.
Contribution
This study provides the first empirical evidence linking atopic dermatitis to improved fecundity in pregnant women.
Findings
Women with atopic dermatitis had a lower risk of infertility treatment and longer time-to-pregnancy (>12 months) compared to those without.
The odds of subfecundity and infertility were reduced in women with atopic dermatitis.
The results suggest an immunological advantage for conception in women with atopic dermatitis.
Abstract
Do women with atopic dermatitis have higher fecundity than those without? Pregnant women with a history of atopic dermatitis had a slightly shorter time-to-pregnancy (TTP) and a lower risk of conceiving using infertility treatment than those without. Atopic dermatitis has a characteristic T-helper-2-cell-skewed immune response that mirrors the immune shift in pregnancy, which is necessary for the pregnant woman’s immune response to tolerate the fetus. Therefore, it has been hypothesized that atopic dermatitis may be advantageous for conception and pregnancy maintenance. However, this has not yet been investigated. This cohort study included 88 713 pregnant women from the population-based Danish National Birth Cohort (DNBC), who were enrolled between 1996 and 2002. The women were defined as having atopic dermatitis if, in a computer-assisted interview conducted around gestational…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
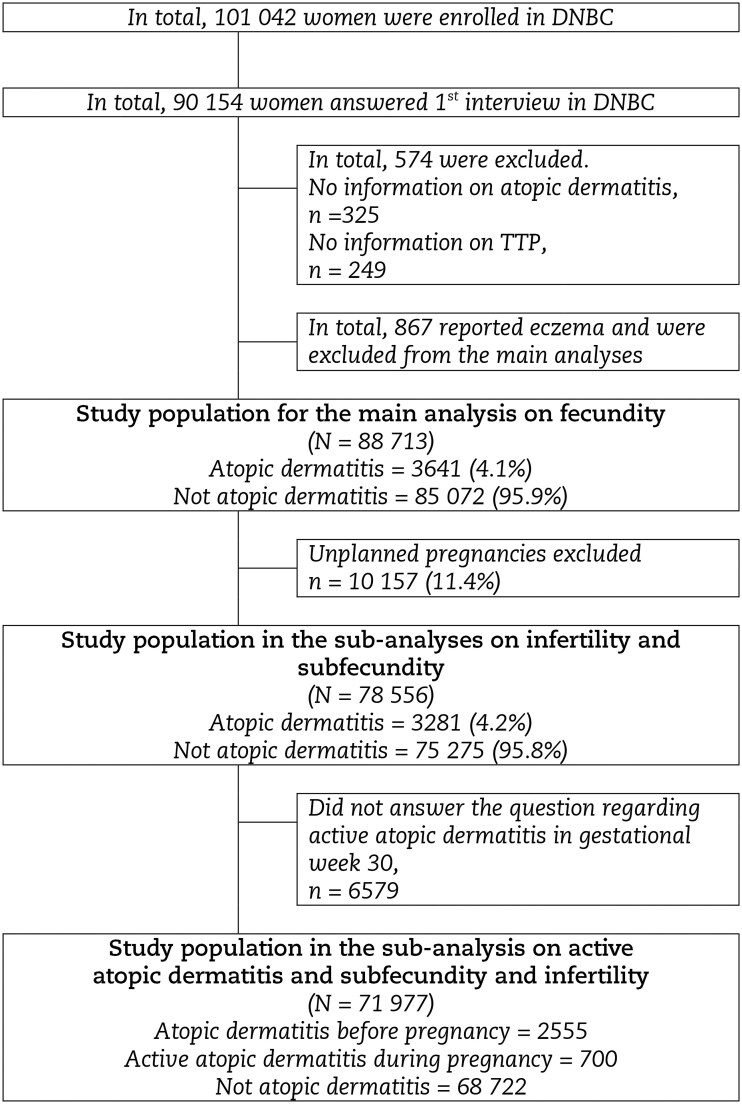 Figure 1
Figure 1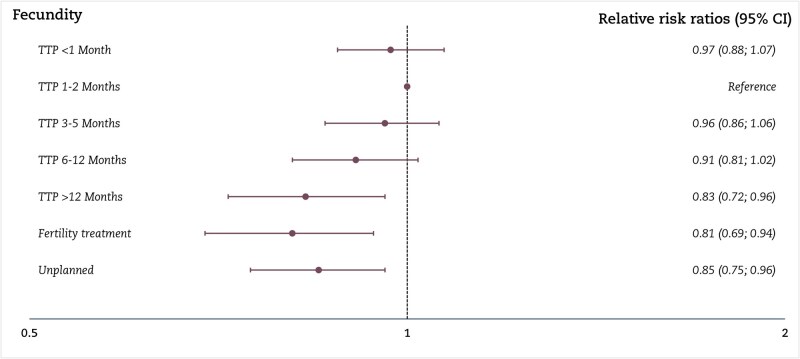 Figure 2
Figure 2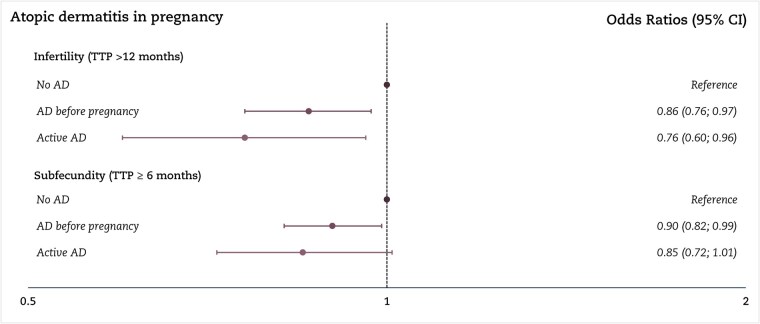 Figure 3
Figure 3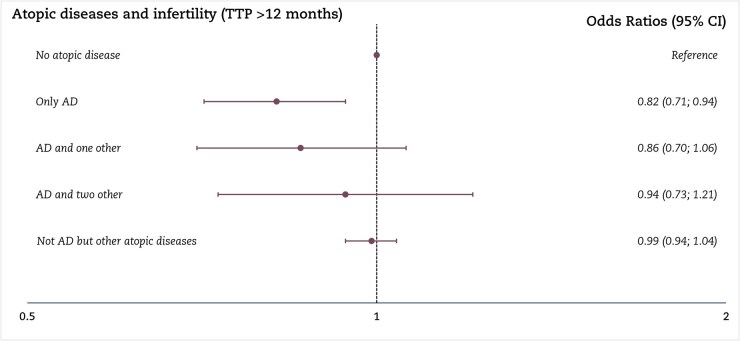 Figure 4
Figure 4| No atopic dermatitis | Atopic dermatitis | |
|---|---|---|
| n (%) | 85 072 (95.9%) | 3641 (4.1%) |
|
| ||
|
| ||
| High-grade professional | 20 053 (23.6) | 941 (25.8) |
| Low-grade professional | 26 300 (30.9) | 1210 (33.2) |
| Skilled worker | 23 863 (28.1) | 913 (25.1) |
| Unskilled worker | 12 009 (14.1) | 455 (12.5) |
| Student | 1971 (2.3) | 100 (2.8) |
| Economically inactive | 876 (1.0) | 22 (0.6) |
| Missing | 0 | 0 |
|
| ||
| No | 47 230 (55.5) | 1990 (54.7) |
| Yes | 37 755 (44.4) | 1646 (45.2) |
| missing | 87 (0.1) | 5 (0.1) |
|
| ||
| Non-smoker | 62 997 (74.1) | 2818 (77.4) |
| 0–10 cigarettes/day | 18 043 (21.2) | 706 (19.4) |
| >10 cigarettes/day | 3822 (4.5) | 106 (2.9) |
| Missing | 210 (0.3) | 11 (0.3) |
|
| ||
| Mean age | 30.5 (4.3) | 30.0 (4.0) |
| Missing | 15 | 0 |
|
| ||
| <1 month | 16 771 (19.7) | 767 (21.1) |
| 1–2 months | 20 598 (24.2) | 958 (26.3) |
| 3–5 months | 14 769 (17.4) | 658 (18.1) |
| 6–12 months | 10 960 (12.9) | 461 (12.7) |
| >12 months | 6605 (7.8) | 241 (6.6) |
| Infertility treatment | 5572 (6.6) | 196 (5.4) |
| Unplanned pregnancy | 9797 (11.5) | 360 (9.9) |
| Missing | 0 | 0 |
|
| ||
| Yes | 2148 (2.5) | 284 (7.8) |
| No | 82 670 (97.2) | 3349 (92.0) |
| Missing | 254 (0.3) | 8 (0.2) |
|
| ||
| Yes | 6964 (8.2) | 726 (19.9) |
| No | 78 004 (91.7) | 2904 (79.8) |
| Missing | 104 (0.1) | 11 (0.3) |
|
| ||
| Yes | 12 039 (14.2) | 1097 (30.1) |
| No | 72 650 (85.4) | 2532 (69.5) |
| Missing | 383 (0.5) | 12 (0.3) |
|
| ||
| Underweight (<18.5) | 3780 (4.4) | 145 (4.0) |
| Normal weight (18.5–25) | 56 686 (66.6) | 2430 (66.7) |
| Overweight (>25–30) | 16 296 (19.2) | 687 (18.9) |
| Obese (>30) | 6925 (8.1) | 320 (8.8) |
| Missing | 1385 (1.6) | 59 (1.6) |
|
| ||
| First child | 39 908 (46.9) | 1775 (48.8) |
| Second child or more | 43 802 (51.5) | 1816 (49.9) |
| Missing | 1362 (1.6) | 50 (1.4) |
|
| ||
| 1997–1998 | 10 912 (96.6) | 383 (3.4) |
| 1999 | 18 265 (96.4) | 681 (3.6) |
| 2000 | 19 167 (96.1) | 775 (3.9) |
| 2001 | 17 513 (95.6) | 804 (4.4) |
| 2002 | 15 814 (95.1) | 819 (4.9) |
| 2003 | 3386 (95.0) | 179 (5.0) |
| Missing | 15 | 0 |
- —Danish Council for Independent Research10.13039/501100004836
- —Aarhus University10.13039/100007605
- —Fonden af Fam. Kjærsgaard, Sunds
- —Research Council of Norway10.13039/501100005416
- —Centres of Excellence funding scheme
- —European Union10.13039/501100000780
- —European Union or the European Research Council
- —European Union, Intereg V ÖKS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatology and Skin Diseases · Food Allergy and Anaphylaxis Research · Pregnancy and Medication Impact
Introduction
Atopic dermatitis is a common chronic inflammatory skin disease that often develops in early childhood, affecting up to 20% of children (Vestergaard et al., 2019). In adults, 2–5% have active disease (Wollenberg et al., 2016), which may significantly reduce the quality of life (Senra and Wollenberg, 2014). The immediate effects of atopic dermatitis, including dry, itchy eczema lesions, a compromised skin barrier function, and sleep disturbances, are well-documented (Silverberg, 2019). However, its long-term implications for reproductive health remain poorly understood.
Although the visible eczema lesions of atopic dermatitis often improve with age, the underlying predisposition may persist, manifesting as dry atopic skin and increased risk of relapses even after long asymptomatic intervals (Weidinger and Novak, 2016; Weidinger et al., 2018; Maintz et al., 2022). Atopic dermatitis is driven by a T-helper (Th) 2-dominant inflammatory response. It is strongly associated with other atopic diseases, such as asthma, allergic rhinitis, and food allergies, partly due to shared genetic factors regulating immune cells and the skin barrier (Ferreira et al., 2017; Silverberg, 2019; Graham and Eigenmann, 2020; Langan et al., 2020; Ravnborg et al., 2021).
In a normal pregnancy, the immune system shifts from a Th1- to a Th2-skewed profile to support implantation and early fetal tolerance (Orefice, 2021). It has been hypothesized that the Th2 dominance seen in individuals with atopic dermatitis may facilitate implantation and early pregnancy establishment, potentially contributing to higher fecundity (the biological capacity to become pregnant; Olsen, 1999), as atopic dermatitis has been associated with reduced risk of spontaneous abortions and increased probability of giving birth at term (Hanzlikova et al., 2009; Isogami et al., 2024). Atopic dermatitis may also positively impact reproductive health through other mechanisms. Up to 50% of individuals with atopic dermatitis have a loss-of-function mutation in the filaggrin gene (FLG), a key component of the skin barrier, which is associated with an earlier onset and more severe atopic dermatitis (Bieber et al., 2022). However, FLG loss-of-function has also been associated with enhanced cutaneous absorption of vitamin D (Khatib et al., 2024), which may positively impact reproductive health by improving fecundity (Arab et al., 2019; Jukic et al., 2019). On the other hand, compromised skin barrier and the consequent increased absorption of endocrine-disrupting chemicals and allergens may adversely affect hormonal balance and the reproductive system (Kezic and Nielsen, 2009; Yilmaz et al., 2020; Munera-Campos and Carrascosa, 2024).
Existing research often groups atopic dermatitis with other atopic conditions, such as asthma and allergic rhinitis, into a single exposure category. This approach may obscure condition-specific effects, as different atopic diseases could have distinct influences on fecundity and fertility (Nilsson et al., 1997; Karmaus and Eneli, 2003). However, a Danish study observed that women with allergic rhinitis experienced shorter time-to-pregnancy (TTP) (Westergaard et al., 2003), suggesting higher fecundity. In the present study, we aimed to investigate whether women with atopic dermatitis also exhibit higher fecundity, measured as TTP and less use of infertility treatment, than those without atopic dermatitis.
Materials and methods
Ethical approval
The Committee for Health Research Ethics Approval (VEK) in Denmark approved the data collection in the Danish National Birth Cohort (DNBC) (KF 01-471/94), and the Danish Data Protection Agency approved the DNBC (journal number 2012-41-0379). The data handling was approved by Statens Serum Institut (SSI) and is covered by SSI’s general approval (No. 18/04608). The DNBC Steering Committee approved this study (Ref. no. 2020-28), and it is registered by the Danish Data Protection Agency, Aarhus University (2016-051-000001, rec No. 1150). According to Danish legislation, Institutional Review Board approval is not required for register-based research. The participants in this manuscript have given written informed consent to the publication of their case details at enrollment.
Study population
This study used data from the DNBC (Olsen et al., 2001; Olsen, 2012), a population-based cohort comprising more than 100 000 pregnancies. Recruitment for the DNBC took place between 1996 and 2002 during the first antenatal visit with the general practitioner (GP). Approximately half of Denmark’s GPs participated in recruiting the women. Around 60% of those invited agreed to participate, and thereby, the DNBC included 30% of all pregnant women in Denmark during the period (Nohr et al., 2006). The women provided information on their lifetime history of atopic dermatitis, lifestyle factors, demographics, health, diseases, TTP, and potential use of infertility treatment twice during pregnancy, at around gestational weeks 17 and 30, using computer-assisted telephone interviews. We excluded 574 women due to missing data on atopic dermatitis and TTP. Women who reported eczema (n = 867) rather than atopic dermatitis were also excluded from the main analysis. Thus, the final study population included 88 713 women (Fig. 1).
Flowchart participants according to atopic dermatitis and fecundity in the Danish National Birth Cohort (DNBC), 1996–2002, Denmark.
Exposure: atopic dermatitis
The women were defined as having had atopic dermatitis if they, in the first interview in the DNBC, reported ever to have had doctor-diagnosed atopic dermatitis (‘Yes, ever had/have atopic dermatitis’ vs ‘No, never had atopic dermatitis’) (Supplementary File S1). The 867 women reporting eczema, but not doctor-diagnosed atopic dermatitis, were excluded from the main analysis as eczema may or may not reflect atopic dermatitis, introducing diagnostic uncertainty and potential misclassification (Fig. 1). They were included in a sub-analysis.
In a sub-analysis, data from the second interview at gestational week 30 on active atopic dermatitis during pregnancy were used to confirm the exposure and ensure that the women had active atopic dermatitis in adulthood. Moreover, to explore women with an atopic constitution, we utilized information on other atopic conditions: asthma, allergic rhinitis, and food allergies from the first interview during pregnancy, since these conditions share genetic factors with atopic dermatitis and are associated with increased disease severity of atopic dermatitis (Ferreira et al., 2017; Silverberg, 2019). Furthermore, having multiple atopic conditions increases the likelihood that women with atopic dermatitis are classified correctly.
Outcomes: measures of fecundity
Fecundity was measured as TTP and the use of infertility treatment. From the first DNBC interview, the women were asked whether the pregnancy was planned or unplanned. Women with planned pregnancies were asked to provide their TTP in five prespecified categories. Further, women who answered ‘yes’ to the question: ‘Did you get any infertility treatment prior to this pregnancy?’ were placed in the infertility treatment category, regardless of their reported TTP. This study categorized fecundity into seven categories (TTP <1 month, 1–2 months, 3–5 months, 6–12 months, >12 months, pregnant after infertility treatment, and unplanned).
TTP was also analyzed as two dichotomized outcomes, restricted to planned pregnancies, as unplanned pregnancies might represent either the most or the least fecund women (Bonde et al., 2006). Women who conceived following infertility treatment were classified as having a TTP >12 months, in line with Danish regulations requiring at least 12 months of attempted conception before public funding of infertility treatment is granted (Alsbjerg, 2025). We examined two dichotomous outcomes: subfecundity (TTP ≥6 months vs <6 months as the reference) and infertility (TTP >12 months vs ≤12 months as the reference), consistent with previous studies (Guldbrandsen et al., 2014).
Covariates
We used directed acyclic graphs (Greenland et al., 1999; Pearl, 2010; Cinelli et al., 2024) to identify potential confounding variables (Supplementary Fig. S1). The following variables were included in the statistical model: Socioeconomic status (the highest of the couple), maternal age at birth, pre-pregnancy BMI, lifestyle factors (smoking and alcohol consumption in early pregnancy, for further adjustment for socioeconomic status), and calendar year. Maternal age at birth was obtained from the Danish Medical Birth Registry, while the remaining variables were retrieved from the first interview in the DNBC (Bliddal et al., 2018). See Table 1.
Statistical analyses
In the main analysis, we applied a multinomial logistic regression model to estimate adjusted relative risk ratios (RRR) with 95% CIs comparing women with atopic dermatitis to women without it, according to fecundity (TTP and infertility treatment), in seven categories. A TTP of 1–2 months was selected as the reference group.
Multivariable logistic regression models were conducted as a sensitivity analysis and for all sub-analyses, with TTP modeled as a binary outcome for both subfecundity and infertility. We estimated odds ratios (ORs) with 95% CIs. An OR <1 indicates a lower likelihood of subfecundity or infertility compared with the reference group of women without atopic dermatitis.
Sub-analyses
We conducted statistical analyses using STATA 18 (StataCorp LLC, College Station, TX, USA). We conducted three sub-analyses. First, we explored the women reporting active atopic dermatitis in pregnancy and subfecundity and infertility, keeping the group with a history of atopic dermatitis before pregnancy without active symptoms in a separate category. The exposure was categorized as: (i) no atopic dermatitis; (ii) atopic dermatitis before pregnancy; and (iii) active atopic dermatitis during pregnancy. Second, we included the women who reported eczema (n = 867) in the multinomial logistic regression models, as eczema could be atopic dermatitis. The exposure was categorized as: (i) neither atopic dermatitis nor eczema; (ii) atopic dermatitis; (iii) eczema.
Third, we examined women who reported multiple atopic symptoms (e.g. atopic dermatitis, asthma, allergic rhinitis, and food allergies) and infertility (TTP >12 months). The analysis was categorized as: (i) no atopic disease; (ii) only atopic dermatitis; (iii) atopic dermatitis and one other disease; (iv) atopic dermatitis and two or more atopic diseases; and (v) Not atopic dermatitis but other atopic diseases.
Missing data were well below 5% and evenly distributed across exposure categories, suggesting that the risk of bias from complete case analyses is minimal (Lee et al., 2021). All models were fitted using robust variance estimation to account for dependencies between pregnancies by the same individual.
Results
In total, 88 713 women were included in the study, of which 3641 (4.1%) reported doctor-diagnosed atopic dermatitis (Fig. 1) and 700 had active atopic dermatitis at gestational week 30. Women with atopic dermatitis were, on average, younger, had a higher socioeconomic status, and were more often non-smokers than women without atopic dermatitis. Further, they had a higher prevalence of asthma (20%), allergic rhinitis (30%), and food allergies (8%) than women without atopic dermatitis (Table 1).
We found that women with atopic dermatitis had a lower risk of the longest TTP categories (6–12 months, RRR: 0.91 (95% CI: 0.81: 1.02) and >12 months, RRR: 0.83 (95% CI: 0.72: 0.96)) and infertility treatment (RRR: 0.81 (95% CI: 0.69; 0.94)) than those without atopic dermatitis. The logistic regression model supported these findings with an OR for infertility of 0.85 (95% CI: 0.77; 0.95) and an OR for subfecundity of 0.89 (95% CI: 0.82; 0.96) in women with atopic dermatitis compared to those without atopic dermatitis (Fig. 2 and Supplementary Tables S1 and S2).
Main analysis of atopic dermatitis and fecundity. The multinomial logistic regression according to atopic dermatitis and fecundity in seven categories, with 1–2 months and no atopic dermatitis as the reference, among 88 713 pregnant women, of which 3641 had atopic dermatitis. Results are shown as relative risk ratios with 95% CI. TTP, time to pregnancy. Adjusted for socioeconomic status (highest of the couple), alcohol drinking and smoking in early pregnancy, body mass index, age at birth, and calendar year.
Sub-analyses
In the first sub-analysis, women who reported active atopic dermatitis during pregnancy had a lower OR of infertility (0.76, 95% CI: 0.60; 0.96) than women without atopic dermatitis; women who had atopic dermatitis but not during pregnancy had an OR of infertility of 0.86 (95% CI: 0.76; 0.97) (Fig. 3). The second sub-analysis, which included women who reported having eczema, showed no association between eczema and fecundity (Supplementary Table S3). In the third sub-analysis of women considered to have an atopic constitution, only women with atopic dermatitis without other atopic conditions had an OR <1 of infertility compared to women without any atopic condition (Fig. 4).
Sub-analysis of active atopic dermatitis and subfecundity and infertility. The logistic regression model according to active atopic dermatitis and subfecundity and infertility among 71 977 pregnant women. In total, 2555 women had atopic dermatitis before pregnancy and 700 had active atopic dermatitis during pregnancy. Unplanned pregnancies are excluded, whereas the use of infertility treatment is included in TTP >12 months. In total, 6579 did not answer the question regarding active atopic dermatitis in interview 2 at gestational week 30. Results are shown as odds ratios with 95% CI. AD, atopic dermatitis; TTP, time to pregnancy. Adjusted for socioeconomic status (highest of the couple), alcohol drinking and smoking in early pregnancy, body mass index, age at birth, and calendar year.
Sub-analyses of atopic diseases (atopic dermatitis, asthma, allergic rhinitis, and food allergy). The logistic regression model according to atopic dermatitis, asthma, allergic rhinitis, and food allergy in a combined variable and infertility among 78 123 pregnant women. Overall, 60 348 (76.8%) had no atopic disease, 1948 (2.5%) had only atopic dermatitis, 815 (1.0%) had atopic dermatitis and one other atopic disease, 496 (0.6%) had atopic dermatitis and two other atopic diseases, and 14 516 (18.5%) did not have atopic dermatitis but had other atopic diseases. Results are shown as odds ratios with 95% CI. AD, atopic dermatitis; TTP, time to pregnancy. Adjusted for socioeconomic status (highest of partners), alcohol drinking and smoking in early pregnancy, body mass index, age at birth, and calendar year. Unplanned pregnancies are excluded from this analysis.
Discussion
In this large cohort study, we found that women with a history of atopic dermatitis had higher fecundity, including a slightly shorter TTP and a lower likelihood of using infertility treatment. The sub-analyses supported the findings from the primary analysis, and the data analysis on women with active atopic dermatitis during pregnancy showed a stronger association. However, the analysis of atopic constitutions did not show a dose–response relationship with the number of atopic conditions.
We had comprehensive and unique information from 88 713 women in early-to-mid pregnancy about the exposure, outcome, and covariates. The comprehensive self-reported data also allowed us to adjust for multiple important potential confounding variables, thereby reducing the risk of confounding. The self-reported information on doctor-diagnosed atopic dermatitis was a major strength of the study since it allowed us to include women with self-reported atopic dermatitis diagnosed by the GPs or by a private dermatologist. However, with a potential risk of recall bias. The interviews covered a variety of questions on health and lifestyle and did not focus on atopic dermatitis, suggesting that potential misclassification is nondifferential. We excluded women who reported unspecified eczema from the exposure group to avoid misclassification of atopic dermatitis. In a sub-analysis, including the women with eczema, there was no association between eczema and fecundity, likely because the women with eczema encompassed a broad range of skin diseases. We did not include diagnosis codes from the Danish National Patient Register (DNPR), as these are only available for hospital-diagnosed patients in Denmark. Approximately 80% of those suffering from atopic dermatitis experience a mild course of the disease (Ballardini et al., 2013) and will probably never be treated at the hospital and, thereby, never be registered in the DNPR (Lynge et al., 2011). Moreover, we expect that women with a prior diagnosis of atopic dermatitis would report this during the DNBC interview, minimizing the risk of misclassification.
Misclassification of fecundity is a possibility, as TTP reflects couple-level fecundity, not just female fecundity. However, any misclassification is likely non-differential, since it is improbable that the partners of women with atopic dermatitis systematically differ from those of women without atopic dermatitis. There is a potential risk of bias due to recall since participants were asked to remember their TTP in the first trimester. However, Jukic et al. (2016) found that women can accurately recall their TTP, though some uncertainty might persist, even when measured shortly after conception. Furthermore, because participants reported TTP categorically, we could not directly calculate fecundability, the probability of conceiving in one menstrual cycle (Eisenberg et al., 2023). Accurate calculations of fecundability require longitudinal TTP data from pregnancy-planner cohorts. In our study, infertility treatment was self-reported, which may have led to some misclassification. A validation study revealed poor agreement between the self-reported infertility treatment and the national IVF register, due to ambiguities in the wording of the DNBC questionnaire. Nevertheless, the self-reported infertility treatment was found to be a valid indicator of sub-fertility (Hvidtjørn et al., 2009), which was the primary focus of the present study. Any misclassification is assumed to be non-differential.
Unplanned pregnancies were included in the main analysis, since it is informative to examine whether women with atopic dermatitis were more or less likely to report unplanned pregnancies. In the present study, 78 556 (89%) of the women reported their pregnancy to be planned, and we observed that women with atopic dermatitis were less likely to have an unplanned pregnancy. Unplanned pregnancies may occur more frequently among both the most and the least fecund women (Bonde et al., 2006). If more highly fecund women without atopic dermatitis are represented in this group, it could explain our results.
The DNBC only includes women who have successfully become pregnant. If atopic dermatitis were to increase sterility or early losses, it would remain undetectable in a study of pregnant women. Consequently, the present study cannot provide insights into women who never conceive. If women with atopic dermatitis experience higher rates of infertility, they may be underrepresented in the study sample, resulting in selection bias. However, exposures that cause sterility will also affect TTP and the use of infertility treatment, and the selection bias will likely only be a theoretical problem rather than a practical one (Olsen, 1999; Weinberg et al., 2021). In our study population, 4% of women had atopic dermatitis, aligning with the prevalence reported by the European Task Force on Atopic Dermatitis/European Academy of Dermatology and Venerology in 2015 for adults (Wollenberg et al., 2016). However, a study on identifying adult atopic dermatitis in questionnaires found that the prevalence varied extensively based on how the question was phrased, and the question, similar to the one asked in DNBC, resulted in the lowest prevalence (Jepsen and Flyvholm, 2007). Since the prevalence found in our cohort matches the estimated prevalence in Europe, we do not expect atopic dermatitis to be strongly associated with participation in our cohort.
The DNBC comprises a higher proportion of women with higher socioeconomic status, which may not directly bias the estimate but could limit its generalizability (Nohr et al., 2006; Jacobsen et al., 2010).
A limitation of the study is the lack of information on the treatment of atopic dermatitis, which would have enabled us to classify the women by disease severity. Consequently, the exposure group probably included mild and severe cases of atopic dermatitis, which could bias our results toward the null. Further, effective treatment of atopic dermatitis could reduce systemic inflammation, thereby minimizing its impact on reproductive parameters (Vakirlis et al., 2024). However, we had data on active atopic dermatitis during pregnancy. We conducted this analysis to explore a higher possibility of increased inflammation before pregnancy, assuming women reporting active dermatitis during pregnancy had more inflammation and a compromised skin barrier function before conceiving, potentially affecting their TTP more substantially than women without atopic dermatitis in adulthood. Some women with atopic dermatitis experience improvement of symptoms during pregnancy, and only 700 of the women in our cohort reported active atopic dermatitis. We observed a slightly stronger association between TTP and women reporting active atopic dermatitis during pregnancy. To investigate the exposure and the hypothesis that Th2 inflammation may confer specific advantages, we conducted sub-analyses including other atopic diseases, as these conditions are associated with severe atopic dermatitis (Silverberg, 2019). The results for atopic dermatitis in combination with asthma, allergic rhinitis, and food allergies showed no association. The group with only atopic dermatitis showed the same results as the main analysis. This may be explained by greater heterogeneity in symptoms and medication use among other atopic diseases, or by the possibility that women with multiple atopic conditions experience more severe disease (Silverberg, 2019; Thyssen et al., 2023), resulting in differences in outcomes between mild and severe atopic dermatitis.
Research on fecundity and fertility in women with atopic dermatitis and other atopic conditions remains limited. In our research, we have previously investigated atopic dermatitis and reproductive outcomes. We found no differences in age in attaining several pubertal milestones among children with atopic dermatitis (Kjersgaard et al., 2025a) and no indication of an adverse effect on reproductive health in young men with atopic dermatitis (Kjersgaard et al., 2025b).
A cohort study by Karmaus and Eneli (2003) examining TTP in women with either atopic dermatitis, allergic rhinitis, or asthma found no significant difference in TTP between women with or without atopic conditions (Karmaus and Eneli, 2003). Three studies have investigated fertility using the total number of children as an outcome; two found slightly higher fertility rates among mothers with atopic dermatitis or other atopic conditions (Nilsson et al., 1997; Karmaus and Eneli, 2003; Tata et al., 2007). In contrast, a more recent cohort study found a strong association between a diagnosis of atopic dermatitis and infertility (Horev et al., 2022). A case-control study by Hanzlikova et al. (2009) observed that women with atopic dermatitis were less likely to be in the group experiencing recurrent pregnancy loss, infertility treatment failure, or infertility; although the results were not significant (Hanzlikova et al., 2009). In addition, Karmaus and Eneli (2003) found no difference in rates of spontaneous abortion between women with and without atopic diseases. These discrepancies in the literature may stem from grouping all atopic diseases into a single category, the differences in defining atopic dermatitis, variations in confounder control, and the fact that diagnoses of atopic dermatitis and infertility can be influenced by several external factors, including socioeconomic status and access to healthcare (Andersen et al., 2019; Brautsch et al., 2023; ESHRE, 2023). Together, these limitations highlight the need for further research to better clarify the relationship between specific atopic conditions and reproductive outcomes.
Our findings align with our hypothesis that atopic dermatitis may provide an immunological advantage for conception and enhance our understanding of immune-related factors in fertility and pregnancy. The underlying reasons for these results remain unclear but may involve the Th2-skewed immune system, which could create a unique environment favorable for implanting and supporting early pregnancy. However, this explanation is likely an oversimplification, as a successful pregnancy depends on a complex balance of Th1/Th2 and regulatory T cells/Th17 throughout the pregnancy (Wang et al., 2020). Moreover, the immunopathology of atopic dermatitis is considerably more complex and includes, in the chronic phase, a Th1 activation (Weidinger et al., 2018). It is also plausible that outcomes differ between mild and severe forms of atopic dermatitis. Another potential explanation could be that women with atopic dermatitis had higher levels of Vitamin D. A study found that patients with atopic dermatitis carrying FLG loss-of-function mutations had higher vitamin D levels, and higher Vitamin D levels are associated with higher fecundability, possibly due to uterine receptivity and embryonic implantation (Jukic et al., 2019; Khatib et al., 2024). It is also possible that the observed association is driven by alternative underlying mechanisms or due to bias.
Conclusion
We found that women with atopic dermatitis had shorter TTP and less use of infertility treatment. These results are reassuring for the large proportion of women with atopic dermatitis. Future studies could further investigate the underlying mechanisms behind these findings. Moreover, the hypothesis should be tested in a population that is not conditioned on pregnancy, ensuring the inclusion of women who never achieve pregnancy.
Supplementary Material
hoaf077_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alsbjerg B, Gøtke H, Madsen LD. Infertilitet - forløbsbeskrivelse. 2025. Available from: https://www.sundhed.dk/sundhedsfaglig/information-til-praksis/midtjylland/almen-praksis/patientbehandling/patientforloeb/forloebsbeskrivelser-icpc/w-svangerskab-foedsel-svangerskabsforebyggelse/infertilitet/ (19 December 2025, date last accessed).
- 2Andersen YMF , Egeberg A, Skov L, Thyssen JP. Demographics, healthcare utilization and drug use in children and adults with atopic dermatitis in Denmark: a population-based cross-sectional study. J Eur Acad Dermatol Venereol 2019;33:1133–1142.30633387 10.1111/jdv.15424 · doi ↗ · pubmed ↗
- 3Arab A , Hadi A, Moosavian SP, Askari G, Nasirian M. The association between serum vitamin D, fertility and semen quality: a systematic review and meta-analysis. Int J Surg 2019;71:101–109.31561004 10.1016/j.ijsu.2019.09.025 · doi ↗ · pubmed ↗
- 4Ballardini N , Kull I, Söderhäll C, Lilja G, Wickman M, Wahlgren CF. Eczema severity in preadolescent children and its relation to sex, filaggrin mutations, asthma, rhinitis, aggravating factors and topical treatment: a report from the BAMSE birth cohort. Br J Dermatol 2013;168:588–594.23445315 10.1111/bjd.12196 · doi ↗ · pubmed ↗
- 5Bieber T , Paller AS, Kabashima K, Feely M, Rueda MJ, Ross Terres JA, Wollenberg A. Atopic dermatitis: pathomechanisms and lessons learned from novel systemic therapeutic options. J Eur Acad Dermatol Venereol 2022;36:1432–1449.35575442 10.1111/jdv.18225 · doi ↗ · pubmed ↗
- 6Bliddal M , Broe A, Pottegard A, Olsen J, Langhoff-Roos J. The Danish Medical Birth Register. Eur J Epidemiol 2018;33:27–36.29349587 10.1007/s 10654-018-0356-1 · doi ↗ · pubmed ↗
- 7Bonde JP , Joffe M, Sallmén M, Kristensen P, Olsen J, Roeleveld N, Wilcox A. Validity issues relating to time-to-pregnancy studies of fertility. Epidemiology 2006;17:347–349.16810093 10.1097/01.ede.0000210239.80406.46 · doi ↗ · pubmed ↗
- 8Brautsch LAS , Voss I, Schmidt L, Vassard D. Social disparities in the use of ART treatment: a national register-based cross-sectional study among women in Denmark. Hum Reprod 2023;38:503–510.36370443 10.1093/humrep/deac 247 · doi ↗ · pubmed ↗