Circulating Orexin-A Levels in Patients With Schizophrenia, Bipolar Disorder, and Major Depressive Disorder: A Systematic Review and Meta-Analysis
Shatha Almahwzi, Samer Ghabashi, Wadha Alyami, Jana Alsolami, Rashid Juma, Sarah Alghamdi, Lojean Althobyane, Manar Alqahtani, Meshal Alotaibi

TL;DR
This study finds that orexin-A levels are significantly lower in schizophrenia and higher in major depressive disorder compared to healthy controls, suggesting its potential as a biomarker.
Contribution
The study provides the first meta-analysis comparing orexin-A levels across schizophrenia, bipolar disorder, and major depressive disorder.
Findings
Orexin-A levels are significantly decreased in schizophrenia compared to healthy controls.
Orexin-A levels are significantly increased in major depressive disorder compared to healthy controls.
Findings in bipolar disorder were inconclusive due to high heterogeneity.
Abstract
Orexin-A, a neuropeptide involved in regulating physiological processes, has potential implications in psychiatric disorders. Studies examining orexin-A levels in schizophrenia, bipolar disorder, and major depressive disorder have produced conflicting results, highlighting the need for further research. To address these inconsistencies, this meta-analysis aims to synthesize existing data on orexin-A levels across these disorders, clarifying its role and potential as a diagnostic or prognostic biomarker. This systematic review, registered with PROSPERO, investigated plasma orexin-A levels in schizophrenia, bipolar disorder, and major depressive disorder. Relevant studies were identified through PubMed and PsycINFO using specific keywords. Inclusion criteria targeted adult patients with these disorders and healthy controls, assessing quality and bias using the MINORS tool for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
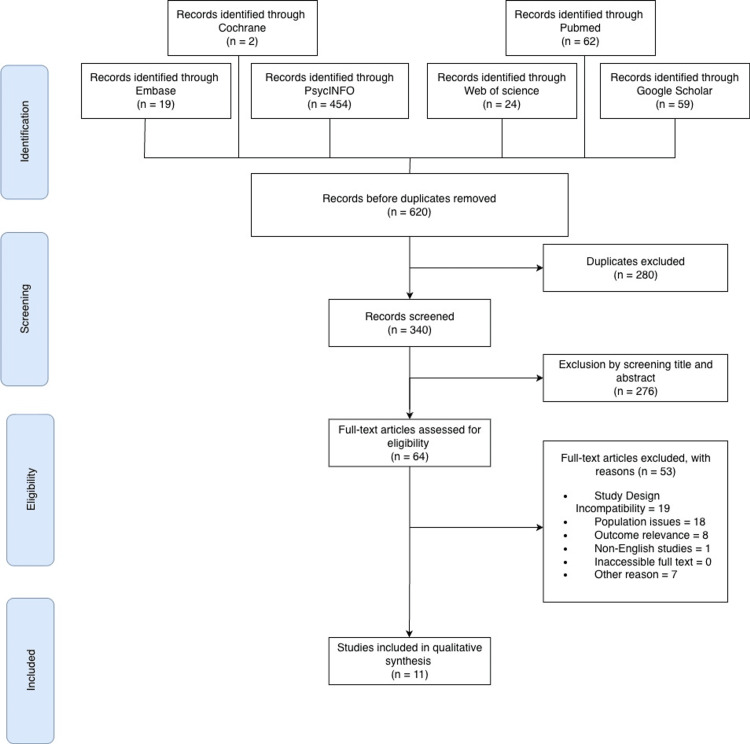 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4| Healthy group | Schizophrenia group | Bipolar group | Depression group | |||||||||||||
| Study ID | No. | Age/Mean (±SD) | BMI | M:F | No. | Age/Mean (±SD) | BMI | M:F | No. | Age/Mean (±SD) | BMI | M:F | No. | Age/Mean (±SD) | BMI | M:F |
| Basoglu, 2010 [ | 22 | 21.7 ± 1.1 | 22.4 ± 2.0 | - | 22 | 21.2 ± 0.75 | - | - | - | - | - | - | - | - | - | - |
| Sun, 2016 [ | 15 | 22.20 ± 2.14 | - | - | 13 | 18-45 | - | - | - | - | - | - | - | - | - | - |
| Lu, 2021 [ | 82 | 27.33 ± 9.41 | - | 1:1.16 | 13 | - | - | 27:34:00 | - | - | - | - | - | - | - | - |
| Wang, 2023 [ | 51 | 29.35 ± 8.41 | 22.6 kg/m² | 26(M):25(F) | - | - | - | - | - | - | - | - | 97 | 33.56 ± 14.11 | 22.18ᵃ / 24.22ᵇ | 33(M); 64(F) |
| Li, 2021 [ | 82 | 27.32 ± 9.40 | - | 38(M):44(F) | - | - | - | - | 57 | 25.04 ± 6.56 | - | 30(M); 27(F) | 74 | 27.58 ± 7.56 | - | 32(M); 42(F) |
| Tsuchimine, 2019 [ | 80 | 47.0 ± 14.2 | 21.9 kg/m² | 32(M); 48(F) | 80 | 36.8 ± 11.2 | 23.2 kg/m² | 38(M); 42(F) | 40 | 41.1 ± 12.1 | 23.4 kg/m² | 16(M); 24(F) | 80 | 43.7 ± 10.4 | 22.7 kg/m² | 37(M); 43(F) |
| Yu, 2023 [ | 54 | 27.94 ± 9.55 | 20.95 kg/m² | 23:31 | 54 | 22.02 ± 7.25 | 20.67 kg/m² | 26:28:00 | 52 | 28.92 ± 11.45 | 23.39 kg/m² | 21:31 | 35 | 30.26 ± 10.26 | 21.1 kg/m² | 15:20 |
| Chen, 2019 [ | 60 | 41.1 ± 9.65 | 24 kg/m² | 29:31:00 | 159 | 41.97 ± 9.26 | 25 kg/m² | 79:21:00 | - | - | - | - | 100 | 27.79 ± 7.1 | - | - |
| Jin, 2020 [ | 100 | 27.63 ± 7.6 | - | 41:59:00 | - | - | - | - | - | - | - | - | 75 | 26.79 | - | 39:36:00 |
| Li, 2024 [ | 74 | 27.36 | - | 32:42:00 | - | - | - | - | - | - | - | - | - | - | - | 32:43:00 |
| Chien, 2015 [ | 34 | 37.1 ± 10.6 | - | 20:14 | 127 | 38.8 ± 10.5 | - | 55:13:00 | - | - | - | - | - | - | - | - |
| Healthy group | Schizophrenia group | Bipolar group | Depression group | |||||||||
| Study ID | No. | Smoker | Comorbidities | No. | Smoker | Comorbidities | No. | Smoker | Comorbidities | No. | Smoker | Comorbidities |
| Basoglu, 2010 [ | 22 | 17 | - | 22 | 13 | - | - | - | - | - | - | - |
| Sun, 2016 [ | 15 | - | - | 13 | - | - | - | - | - | - | - | - |
| Lu, 2021 [ | 82 | - | - | 61 | - | - | - | - | - | - | - | - |
| Wang, 2023 [ | 51 | 8 | - | - | - | - | - | - | - | 97 | 15 | - |
| Li, 2021 [ | 82 | - | - | - | - | - | 57 | - | - | 74 | - | - |
| Tsuchimine, 2019 [ | 80 | 10 | - | 80 | 24 | - | 40 | 8 | - | 80 | 13 | - |
| Yu, 2023 [ | 54 | 6 | - | 54 | 22.0±2.2 | - | 52 | 8 | - | 35 | 7 | - |
| Chen, 2019 [ | 60 | 7 | 30 | 159 | 33 | 184 | - | - | - | 100 | - | - |
| Jin, 2020 [ | 100 | - | - | - | - | - | - | - | - | 75 | - | - |
| Li, 2024 [ | 74 | - | - | - | - | - | - | - | - | - | - | - |
| Chien, 2015 [ | 34 | - | - | 127 | 20 | - | - | - | - | - | - | - |
| Healthy group | Schizophrenia group | Bipolar Disorder group | Major Depression Disorder group | |||||
| Study ID | Value | p-value | Value | p-value | Value | p-value | Value | p-value |
| Basoglu, 2010 [ | 14.18 ± 33.7 | 0.015 | 18.9 ± 40.3 | 0.015 | - | - | - | - |
| Sun, 2016 [ | 168.81 ± 13.87 | <0.05 | 160.96 ± 11.70ᶜ / 181.44 ± 17.25ᵈ | 0.49 | - | - | - | - |
| Lu, 2021 [ | 45.58±9.63 (M) / 52.42±11.94 (F) / 49.25±11.39 | 0.007 | 43.3±4.09 (M) / 42.78±4.92 (F) / 42.78±4.89 | 0.001 (Total) / 0.094 (M) | - | - | - | - |
| Wang, 2023 [ | 1.330 ± 3.140 | 0.861 | - | - | - | - | 1.230 ± 1.270 ᶠ / 1.180 ± 8.50 ʰ | 0.861 |
| Li, 2021 [ | 49.25 ± 8.65 | <0.001 | - | - | 65.50 ± 4.03 | <0.001 | 59.04 ± 7.39 | <0.001 |
| Tsuchimine, 2019 [ | 108.8 ± 29.1 | - | 99.5 ± 35.7 | 0.007 | 88.2 ± 16.8 | 0.010 | 96.2 ± 27.5 | 0.089 |
| Yu, 2023 [ | 758.58 ± 215.44 (29.31 SE) | <0.001 | 602.56 ± 156.00 (21.22 SE) | <0.001 | 645.65 ± 225.91 (31.33 SE) | <0.001 | 602.56 ± 142.57 (24.1 SE) | <0.001 |
| Chen, 2019 [ | 600 ± 170 | <0.01 | Clozapine 1.54±0.60 / 1.89±0.50ᵉ / 1650.1±591.8ᵗ | <0.01 | - | - | - | - |
| Jin, 2020 [ | 24.13 ± 30.18 | <0.001 | - | - | - | - | 34.26 ± 36.68 | <0.001 |
| Li, 2024 [ | 12.77 | <0.001 | - | - | - | - | 27.20 | <0.0001(F) / 0.999(M) |
| Chien, 2015 [ | 38.8 ± 15.5 | <0.001 | 60.7 ± 37.9 | <0.001 | - | - | - | - |
| PANSS positive symptoms | PANSS negative symptoms | PANSS general psychopathology | ||||
| Study ID | - | p-value | - | p-value | - | p-value |
| Basoglu, 2010 [ | 21.4±4.1ᵃ / 14.9±4.5ᵇ / 11.3±4.5ᶜ | <0.001 | 24.5±8.5ʰ / 17.3±5.7ˢ / 16.2±7.4ᵏ | 0.003 | 49.4±6.9ᵐ / 37.9±11.0ʸ / 30.6±13.9ᶻ | <0.0001 |
| Sun, 2016 [ | 24.69ᵈ / 9.08ᵉ | 0.019 | 30.46ᵈ / 12.92ᵉ | 0.001 | 53.08ᵈ / 24.31ᵉ | 0.001 |
| Tsuchimine, 2019 [ | 13.8 ± 5.3 | - | 15.5 ± 6.2 | - | 31.3 ± 8.1 | - |
| Chien, 2015 [ | 7.97 ± 4.38 | 0.968 | 16.19 ± 6.31 | 0.057 | 6.18±3.16 / 11.11±3.66 / 7.78±2.95 | - |
| Study (Author, Year) | Study Design | Assessment Tool | Total Score | Risk of Bias |
| Sun, 2016 [ | Prospective Cohort | MINORS | 20/24 | Low |
| Basoglu, 2010 [ | Prospective Cohort | MINORS | 17/24 | Low-Moderate |
| Lu, 2021 [ | Case-Control | MINORS | 14/24 | Moderate |
| Li, 2021 [ | Case-Control | MINORS | 12/24 | Moderate |
| Wang, 2023 [ | Cross-sectional | AXIS | 19/20 | Low |
| Tsuchimine, 2019 [ | Cross-sectional | AXIS | 19/20 | Low |
| Yu, 2023 [ | Cross-sectional | AXIS | 18/20 | Low |
| Chen, 2019 [ | Cross-sectional | AXIS | 18/20 | Low |
| Jin, 2020 [ | Cross-sectional | AXIS | 18/20 | Low |
| Li, 2024 [ | Cross-sectional | AXIS | 18/20 | Low |
| Chien, 2015 [ | Cross-sectional | AXIS | 17/20 | Low-Moderate |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and Wakefulness Research · Mind wandering and attention · Sleep and Work-Related Fatigue
Introduction and background
Orexin, a neuropeptide that circulates in cerebrospinal fluid (CSF), plays a role in wakefulness, arousal, regulation of circadian rhythm, appetite, and cognitive function [1]. In the lateral hypothalamus, orexin is produced in two main forms: orexin-A and orexin-B (hypocretin-1 and hypocretin-2), which bind to orexin-1 and orexin-2 receptors, respectively, with considerable affinities [2].
Measuring orexin-A in cerebrospinal fluid (CSF) is essential for the diagnosis of narcolepsy type one, which is characterized by very low levels of orexin-A, as a value below 110 pg/ml is required to establish the diagnosis [3]. Radioimmunoassay (RIA) is a standard method with high specificity and sensitivity in orexin quantification [4]. Additional methods for orexin measurements include enzyme immunoassay (EIA) and fluorescence immunoassay (FIA) [5,6].
Orexin dysregulation was observed among psychiatric patients, highlighting orexin’s potential involvement in the pathophysiology of psychiatric disorders [1]. Several studies have investigated the orexins' role in schizophrenia and mood disorders [7-11]. For example, animal models of depression observed a reduction in the number and size of orexin neurons [7]. Additionally, depressive behavior was significantly reduced following intracerebral injection of orexin-A [8]. In human studies, polymorphism in the HCRTR1 gene, a gene that encodes orexin-1 receptors, was positively associated with major depressive disorder [9]. Brundin L et al. reported that patients with major depressive disorder had lower orexin-A levels [10]. However, another study revealed that orexin-A levels were higher in patients with depression compared to healthy controls [11].
In bipolar disorder (BP), evidence indicates that patients exhibit reduced orexin-A levels relative to controls [12]. Conversely, another study reported elevated orexin-A levels in patients with bipolar disorder compared to controls [13].
Altered orexin-A level was observed among schizophrenia patients and was linked to symptoms and treatment response. For example, a significant positive correlation has been found between orexin levels and sleep latencies in schizophrenia patients [14]. Furthermore, orexin-A level could be used to predict response to clozapine. Clozapine is an atypical antipsychotic medication that is used to treat resistant schizophrenia [15,16]. Elevated orexin-A level was significantly associated with clozapine response, as a study documented that the clozapine-responsive group has a high orexin-A level compared to the clozapine-resistant and antipsychotic-free groups [17]. Another study by Tsuchimine et al. reported that a subgroup of people with schizophrenia has higher levels of orexin-A than normal controls [12]. Furthermore, patients with schizophrenia with higher orexin-A levels had fewer negative and disorganized symptoms [18]. Conversely, a systematic review and meta-analysis deny observation of any abnormality in orexin-A concentration in patients with schizophrenia [19]. As these results seem contradictory, a comprehensive study is needed to overcome these inconsistencies. This study aims to investigate the relationship between plasma orexin-A levels in adult patients with schizophrenia, bipolar disorder, and major depressive disorder compared to healthy controls.
Review
Methodology
Review of the Literature
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20]. The study protocol was registered with PROSPERO with the following ID: CRD42024570341 [21]. Due to the nature of the study, ethical approval was not required. Relevant studies were identified in July 2024 by using the electronic databases of PubMed, PsycINFO, Web of Science, Embase, Google Scholar, and Cochrane Library. The following keywords were used: (Schizophrenia OR schizophrenic disorders OR dementia praecox OR bipolar disorders OR bipolar mood disorder OR depression OR depressive disorder) AND (orexin OR hypocretin OR orexin-A OR hypocretin-1 OR orexin-B OR hypocretin-2) AND (plasma OR serum) AND (measurement OR levels). The search was compliant with the PICO criteria [22]. To ensure the inclusion of the most recent evidence, an updated search was conducted in July 2025 using the same search strategy, focusing on PubMed and Google Scholar to identify any newly published studies. However, no additional studies met the inclusion criteria and were therefore not included in the final analysis. Deviations from the registered PROSPERO protocol included (1) the exclusion of bipolar disorder and certain subgroup analyses (antipsychotic medications in schizophrenia) from the quantitative meta-analysis due to extreme heterogeneity (I^2 > 90%) observed during preliminary analysis and (2) the decision to report results using standardized mean difference (SMD) rather than mean difference (MD) to account for variability in assay calibration and unit reporting (e.g., pg/mL vs. ng/L) across the included studies.
Inclusion and Exclusion Criteria
This systematic review included (a) adult patients diagnosed with schizophrenia, MDD, or bipolar disorder (DSM-IV/V or ICD-10); (b) studies with healthy control groups; (c) studies measuring plasma orexin-A levels; (d) randomized controlled trials or observational studies (cross-sectional, cohort, case-control); and (e) studies published in English.
Studies were excluded if they (a) involved participants with comorbid physical or neurological conditions known to independently alter orexin levels (e.g., narcolepsy, traumatic brain injury, or severe metabolic disorders) or (b) were non-original research articles, including reviews, meta-analyses, editorials, case reports, or conference abstracts.
Assigned reviewers independently screened each eligible study, and disagreements were resolved through discussion after retrieving the full text to determine whether inclusion and exclusion criteria were met.
Screening and Data Extraction
Three independent reviewers (SA, JA, and SMA) screened papers simultaneously and independently and reviewed them by title and abstract using the Rayyan search web and mobile app for systematic review [23]. The full text was then reviewed by three independent reviewers (MA, RJ, and WA) simultaneously. Data extraction was performed by two reviewers (SA and LA) for the following variables:
Study characteristics: first author name, publication year, country where the study was performed, and the study design, age, gender, body mass index, smoking, and medication status.
Primary outcome: the mean, standard deviation, and sample size of plasma orexin-A levels for patient and control groups.
Secondary outcomes: Positive and Negative Syndrome Scale (PANSS), Hamilton Depression Rating Scale (HAM-D), Brief Psychiatry Rating Scale (BPRS), Young Mania Rating Scale (YMRS), and Pittsburgh Sleep Quality Index (PSQI). To avoid duplication, the retrieved data were double-checked independently by two separate reviewers.
Assessment of Quality and Bias Risk
The methodological quality of the included studies was assessed using tools specific to their study designs.
For cross-sectional studies, the Appraisal tool for Cross-Sectional Studies (AXIS) was employed. This 20-item tool evaluates study design, target population, sampling, and reporting quality. Each item is scored as 1 (Yes) or 0 (No/Don’t Know), yielding a total score that indicates the overall quality of reporting and risk of bias.
For non-randomized studies (case-control and cohort): The Methodological Index for Non-Randomized Studies (MINORS) was used [24]. This instrument consists of 12 items for comparative studies, with each item scored from 0 to 2 (0 = not reported, 1 = reported inadequately, 2 = reported adequately). The total score ranges from 0 to 24 for comparative studies, with higher scores reflecting higher methodological quality. Two reviewers (RJ and WA) independently assessed each study, and disagreements were resolved through discussion.
Meta-Analysis of the Included Data
Statistical analyses were performed using Review Manager (RevMan) [Computer program], Version 5.4, The Cochrane Collaboration (Copenhagen, Denmark). The standardized mean difference, or weighted mean difference, with 95% confidence intervals, was calculated to compare the plasma orexin-A levels between patient and control groups. A random-effects model was employed to account for potential heterogeneity between studies. Also, potential differences between mental health disorders were examined by subgroup analyses by diagnostic category (schizophrenia, major depressive disorder, and bipolar disorder). Moreover, the statistical heterogeneity was evaluated using Cochrane's Q test and the I-squared (I²) statistic. To explore sources of heterogeneity and conduct subgroup analyses and meta-regression, considering study design, patient characteristics, and methodological factors. Assessment of publication bias using funnel plots was planned. However, due to the limited number of studies included in each subgroup analysis (n < 10), these tests were not performed, as they would lack sufficient statistical power to detect asymmetry. Sensitivity analyses were performed to assess the robustness of the findings, such as excluding studies with a high risk of bias or influential studies.
Results
The Literature Findings
In this study, a total of 620 articles were initially collected. After removing 280 duplicates, the remaining studies were screened for eligibility. These articles were sourced from several databases, including PubMed, Google Scholar, Embase, PsycINFO, Web of Science, and the Central Register of Controlled Clinical Trials (CENTRAL). Initially, the full texts of 64 articles were reviewed. However, after applying the exclusion criteria, only 11 articles published between January 2010 and March 2024 were included in the final analysis in Figure 1 [11-13,18,25-31]. Among these, there were two case-control studies, two prospective cohort studies, and seven cross-sectional studies. The characteristics of all the articles included are presented in Table 1.
PRISMA diagram
A Description of the Characteristics of the Included Studies
The total number of participants included in the selected studies was 1,778, comprising 824 men and 954 women. Among these, 654 were healthy controls, 514 had schizophrenia, 149 had bipolar disorder, and 461 were diagnosed with depression. All participants were adults with a normal body mass index (BMI) in Table 1. The number of smokers is identified in Table 2.
The pooled sample across the included studies consisted of healthy participants as well as individuals diagnosed with schizophrenia, major depressive disorder (MDD), and bipolar disorder (BD). Healthy participants (n = 654) had no history of medication use. Within the schizophrenia group (n = 514), 115 patients were first-episode and drug-naive, drawn from Lu et al. (n = 61) and Yu et al. (n = 54) [25,26]. Among the medicated schizophrenia patients, treatment regimens varied. For example, in Chien et al. [18], of 127 patients, 21 were on typical antipsychotics and 99 on atypical antipsychotics. Tsuchimine et al. reported extensive polypharmacy in 80 patients, including 52 on typical antipsychotics, 14 on atypical antipsychotics, and 17 on benzodiazepines [12]. Some studies specified particular medications, with 122 patients treated with clozapine, 20 on olanzapine, and 50 on other less obesogenic atypical antipsychotics like aripiprazole or amisulpride [27-29].
For depression (n = 461), 175 patients were first-episode and treatment-naive according to Jin et al. and Li et al. [11,30]. Medication use among treated patients was inconsistently reported: Wang et al. noted that 50 out of 97 patients (51.5%) were on medication, though the types of medication were unspecified [31]. Li et al. included 74 MDD patients but only clarified that benzodiazepines had not been used in the previous six months [13]. Tsuchimine et al. reported that 77 of 80 patients (96.2%) were on antidepressants, while Yu et al. found 18 of 35 patients (51.4%) were medicated with antidepressants [12,26].
In the bipolar disorder group (n = 149), no patients were medication-naive, and polypharmacy was common. Yu et al. described 52 patients, with 32 on mood stabilizers, 30 on antipsychotics, and 24 on antidepressants [26]. Similarly, Tsuchimine et al. reported 40 BD patients receiving treatments including antidepressants (18 patients), lithium (14 patients), and benzodiazepines (15 patients) [12]. Li et al. included 57 BD patients but did not specify medication regimens [13].
Patient Reported Outcomes, Complications, and Clinical Outcomes
Orexin A levels in patients with schizophrenia, major depressive disorder, and bipolar disorder groups are shown in Table 3.
Schizophrenia
In this review of six studies on the schizophrenia group, both Chen et al. and Chien et al. found that orexin-A levels were slightly higher in patients receiving less obesogenic antipsychotics compared to those on clozapine [18,27]. In Chien’s study, individuals with schizophrenia exhibited higher orexin-A levels than healthy controls, with increased orexin-A associated with fewer negative and disorganized symptoms [18]. Importantly, plasma orexin-A levels were not directly linked to the weight gain liability of these medications. Similarly, Basoglu et al. found that patients with schizophrenia had higher orexin A levels compared to healthy controls [29]. On the other hand, in Sun et al., orexin release was delayed by four hours following eight weeks of clozapine treatment [28]. Lu et al. and Yu et al. observed reduced orexin A levels in individuals with schizophrenia relative to control participants [25,26]. The changes in PANSS score are shown in Table 4.
Chen’s study involved patients who were using antipsychotic medications [27]. In contrast, the studies by Lu et al. included only participants who were not taking antipsychotic drugs [25]. Basoglu et al. and Sun et al. included participants who had been treated with olanzapine for six weeks and clozapine for eight weeks, respectively [28,29].
The meta-analysis revealed a significant decrease in orexin-A levels in the schizophrenia group compared to healthy controls (4 studies, 373 participants). The pooled standardized mean difference (SMD) was -0.38 (95% CI: -0.72 to -0.05; p = 0.03) (Figure 2). Moderate statistical heterogeneity was observed (I^2 = 54%, p = 0.09). This variability reflects the wide range of absolute values reported across different assay platforms.
Meta-analysis schizophrenia vs. control
To further investigate potential sources of heterogeneity, a subgroup analysis based on gender was conducted on two studies [18,25]. However, this analysis did not reveal any significant differences in orexin-A levels between males and females (two studies, SMD = -0.09, 95% CI: -0.38 to 0.20; I^2 = 0%, p = 0.55) (Figure 3).
Meta-analysis of schizophrenia and sex differences
Depression
In this review of eight studies on depression groups, Jin et al. and Li et al., which included treatment-naive and right-handed participants, reported an increase in orexin A levels [11,30]. Wang et al. found that orexin-A levels did not differ among the three groups of depression with and without childhood trauma and healthy controls [31]. Yu et al. found that orexin levels in patients with depression were lower compared to controls, while Tsuchimine et al. reported a decrease [12,26]. Li et al. observed elevated orexin A levels in patients with schizophrenia relative to the control group [13]. Some studies, including Yu et al. and Tsuchimine et al., were excluded from the meta-analysis due to differences in clinical characteristics and inclusion criteria (e.g., use of medications, handedness) [12,26].
For the depression group, a significant increase in orexin-A levels was observed (two studies, 314 participants). The pooled standardized mean difference (SMD) was 0.38 (95% CI: 0.15 to 0.60; p = 0.001) (Figure 4). Statistical heterogeneity was absent (I^2 = 0%), indicating consistent effect sizes across the included studies despite differing absolute baseline values.
Meta-analysis depression vs. control
Bipolar
In this review of three studies on bipolar groups, Li et al. found an increase in orexin A levels, Tsuchimine et al. reported reduced plasma orexin-A levels in patients with bipolar disorder, and Yu et al. observed a decrease [12,13,26]. A meta-analysis was not conducted for bipolar disorder studies due to high heterogeneity among them. This variability was mainly attributed to differences in inclusion criteria. For instance, Li et al. and Yu et al. included only right-handed participants, while Tsuchimine et al. did not apply any handedness restriction [12,13,26]. Additionally, Li et al. and Yu et al. differed in other participant characteristics, such as age and educational background [13,26]. These inconsistencies made it difficult to combine the data meaningfully in a meta-analysis.
Quality Assessment and Risk of Bias
The quality assessment revealed generally robust methodological standards across the included literature, as demonstrated in Table 5.
Non-randomized studies (MINORS): among the cohort and case-control studies, scores ranged from 12 to 20 out of a possible 24 points. One prospective cohort study achieved a high score of 20, indicating a low risk of bias, while the case-control studies scored between 12 and 14, reflecting moderate methodological quality due to limitations in prospective calculation of study size and follow-up reporting.
Cross-sectional studies (AXIS): the included cross-sectional studies demonstrated high reporting quality, with AXIS scores ranging from 17 to 19 out of 20. Strengths were noted in clear aims, appropriate study design, and justified discussions, while common limitations included the lack of justified sample size calculations and non-response bias analysis.
Discussion
To the best of current knowledge, this is the first systematic review and meta-analysis that provides insight into investigating plasma orexin-A levels across patients with schizophrenia (SCZ), bipolar disorder (BD), and major depressive disorder (MDD), synthesizing data from 11 studies involving 1,778 participants [11-13,18,25-31].
Orexin Dysregulation in Schizophrenia
The meta-analysis revealed that circulating orexin-A levels were significantly reduced in patients with schizophrenia (p = 0.03). While the effect size was small to moderate (SMD = -0.38), the direction of the effect was consistent. The moderate heterogeneity observed (I^2 = 54%) suggests that while the trend of reduced orexin is consistent, the magnitude of this reduction varies, likely due to differences in assay sensitivity or medication effects (e.g., clozapine vs. other antipsychotics).
This finding aligns with previous research highlighting the potential role of orexin deficiency in the pathophysiology of the disorder. Previously, Lu et al. highlighted the potential role of orexin deficiency in schizophrenia in support of this finding [25]. Orexin is a neuropeptide that plays a role in arousal, circadian rhythms, and wakefulness [1]. Recent evidence also implicates orexins in attention and cognitive function, with animal models of orexin deficiency exhibiting significant cognitive impairment [1,32]. Consequently, the present findings imply that the observed orexin deficiency may constitute a neurobiological mechanism underlying the cognitive deficits and negative symptoms commonly observed in schizophrenia.
Subgroup Analysis by Gender
Contrary to earlier reports suggesting gender-specific alterations, this meta-analysis observed no gender-based differences in orexin-A levels among schizophrenia patients [25]. This supports the conclusion by Li et al. that orexin-A dysregulation in this population is likely a core feature of the disorder, independent of sex [19].
Role of Antipsychotics
The systematic review indicates that patients treated with antipsychotics, particularly clozapine, exhibit lower orexin-A levels. Basoglu et al. similarly reported that patients treated with atypical antipsychotics displayed reduced peptide levels [29]. This agreement with Chen et al. suggests a potential confounding influence of medication [27]. It remains difficult to disentangle whether reduced orexin-A is an intrinsic trait of schizophrenia or a secondary effect of antipsychotic treatment, given that clozapine has been shown to disrupt circadian rhythms and delay orexin release phases.
Orexin Dysregulation in Major Depressive Disorder
In contrast to schizophrenia, the meta-analysis revealed significantly elevated orexin-A levels in patients with MDD compared to controls. This result is consistent with findings by Jin et al. [11]. Given orexin’s role in emotional regulation and the sleep-wake cycle, these elevated levels may reflect a state of physiological hyperarousal often seen in depression with insomnia [1]. Clinically, this supports the mechanism of dual orexin receptor antagonists (DORAs), such as suvorexant, which improve symptoms in patients with depression by dampening this overactive signaling [33]. However, variance exists in the literature, with some studies reporting reduced levels. This discrepancy highlights the need to account for clinical heterogeneity, such as depression subtypes (e.g., atypical vs. melancholic), which may present with different arousal profiles [12,26].
Orexin Dysregulation in Bipolar Disorder
A quantitative meta-analysis was not conducted for the bipolar disorder subgroup due to extreme statistical heterogeneity (I^2 > 90%). This statistical variance likely reflects profound methodological and clinical heterogeneity, specifically differences in patient mood states (e.g., acute mania versus bipolar depression) and medication regimens (e.g., lithium versus antipsychotics) across the included studies. Consequently, these findings are summarized qualitatively. For instance, Tsuchimine et al. reported lower plasma orexin-A levels in patients with bipolar disorder, whereas Yu et al. observed significantly higher levels [12,26]. This contradiction suggests that orexin dysregulation in bipolar disorder may be state-dependent, fluctuating between manic and depressive episodes, rather than serving as a static trait marker.
Limitations
This study is subject to several limitations. First, significant clinical heterogeneity was observed, particularly regarding potential confounders such as body mass index (BMI) and smoking status, which are known to modulate orexin physiology. These variables were inconsistently reported across studies, preventing a fully adjusted meta-regression. Second, the restriction to English-language publications may have introduced selection bias. Third, the majority of included studies utilized small sample sizes (n < 100), limiting statistical power and increasing the risk of Type II errors [34]. Finally, the variability in assay methods (RIA vs. ELISA) and unit reporting (pg/mL vs. ng/L) across studies complicates the direct comparison of absolute plasma concentrations.
Future recommendations
To address these limitations, future research should employ longitudinal designs to assess orexin-A stability across different disease phases, particularly in bipolar disorder. Researchers are encouraged to standardize assay protocols and report results in uniform units (pg/mL) to facilitate valid quantitative synthesis. Furthermore, large-scale, multi-center studies that control for metabolic confounders (BMI, medication status) are necessary to confirm the diagnostic utility of plasma orexin-A biomarkers. Clinically, these results suggest divergent therapeutic avenues: exploring orexin agonists for schizophrenia-associated cognitive deficits and orexin antagonists for depression-associated hyperarousal.
Conclusions
This meta-analysis demonstrates a divergent pattern of neuroendocrine dysregulation, characterized by significantly reduced plasma orexin-A levels in schizophrenia and elevated levels in major depressive disorder. Conversely, the high heterogeneity observed in bipolar disorder suggests that orexin-A alterations may be state-dependent (fluctuating between manic and depressive episodes) or modulated by psychotropic medications, rather than serving as a static trait marker. Clinically, these results imply distinct therapeutic avenues: potential utility for orexin agonists in addressing negative symptoms in schizophrenia, versus orexin antagonists to manage hyperarousal in depression. Future research must prioritize longitudinal designs controlling BMI and medication to validate orexin-A as a differential diagnostic biomarker.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The hypocretin/orexin system: an increasingly important role in neuropsychiatry Med Res Rev Chen Q de Lecea L Hu Z Gao D 1521973520152504400610.1002/med.21326 · doi ↗ · pubmed ↗
- 2Orexin receptors: pharmacology and therapeutic opportunities Annu Rev Pharmacol Toxicol Scammell TE Winrow CJ 2432665120112103421710.1146/annurev-pharmtox-010510-100528 PMC 3058259 · doi ↗ · pubmed ↗
- 3The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias Arch Neurol Mignot E Lammers GJ Ripley B 155315625920021237449210.1001/archneur.59.10.1553 · doi ↗ · pubmed ↗
- 4Proteomic analysis of egg white heparin-binding proteins: towards the identification of natural antibacterial molecules Sci Rep Guyot N Labas V Harichaux G 27974620162729450010.1038/srep 27974 PMC 4904793 · doi ↗ · pubmed ↗
- 5CSF beta-amyloid levels are altered in narcolepsy: a link with the inflammatory hypothesis?J Sleep Res Liguori C Placidi F Albanese M 4204242320142463566210.1111/jsr.12130 · doi ↗ · pubmed ↗
- 6Cerebrospinal fluid melanin-concentrating hormone (MCH) and hypocretin-1 (HCRT-1, orexin-A) in Alzheimer's disease P Lo S One Schmidt FM Kratzsch J Gertz HJ 08201310.1371/journal.pone.0063136 PMC 364673623667582 · doi ↗ · pubmed ↗
- 7Genotype-dependent effect of ACTH 1-24 on grooming and yawning in two inbred strains of rats Neuropeptides Eguibar JR Barajas M Moyaho A 2832883820041546419310.1016/j.npep.2004.05.003 · doi ↗ · pubmed ↗
- 8I.c.v. administration of orexin-A induces an antidepressive-like effect through hippocampal cell proliferation Neuroscience Ito N Yabe T Gamo Y 72073215720081895215210.1016/j.neuroscience.2008.09.042 · doi ↗ · pubmed ↗