A Case of Suspected Pit Viper Bite in Rural Nepal: Lessons for Snakebite Care
Samuel D Horton, Karolina A Szarzanowicz, Nishad Bhatta

TL;DR
A woman in Nepal was treated with antivenom after a suspected pit viper bite, but the treatment was unnecessary and risky, highlighting the need for better snakebite care strategies.
Contribution
The paper emphasizes the importance of syndrome-led management and local ecology in reducing unnecessary antivenom use for snakebites.
Findings
Administering antivenom for pit viper bites is ineffective and increases anaphylaxis risk.
Serial coagulation testing and syndrome-based care are more reliable than species identification.
System-level improvements like community education and transport support can reduce iatrogenic harm.
Abstract
Pit viper envenoming is common across South Asia. Indian polyvalent antivenom (ASV) does not neutralise pit viper venom. Given the inherent uncertainty in snake species identification, the World Health Organisation (WHO) recommends a syndromic approach to guide ASV use. A 59-year-old woman was bitten on her right ring finger while cutting grass in the Terai farmland of eastern Nepal. Within one hour, she developed hand and forearm oedema with no bleeding or signs of neurotoxicity. Initial coagulation was normal: the 20-minute whole blood clotting test (20WBCT) clotted, prothrombin time (PT) was 12.4 seconds and international normalised ratio (INR) was 1.0. Urinalysis showed no haematuria. Ten vials of ASV were administered at a peripheral treatment centre with no immediate reaction. She was transferred to a tertiary hospital where she received intravenous (IV) fluids and analgesia and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
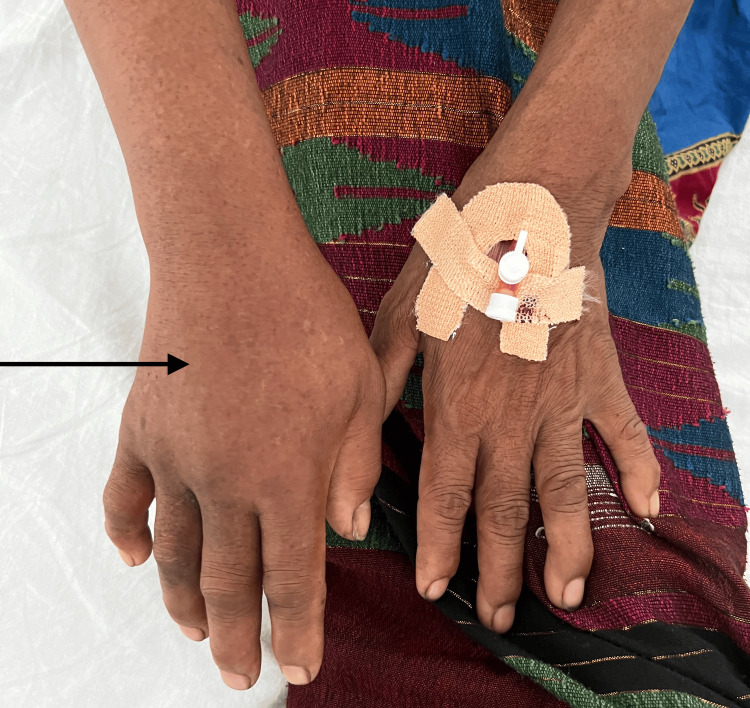 Figure 1
Figure 1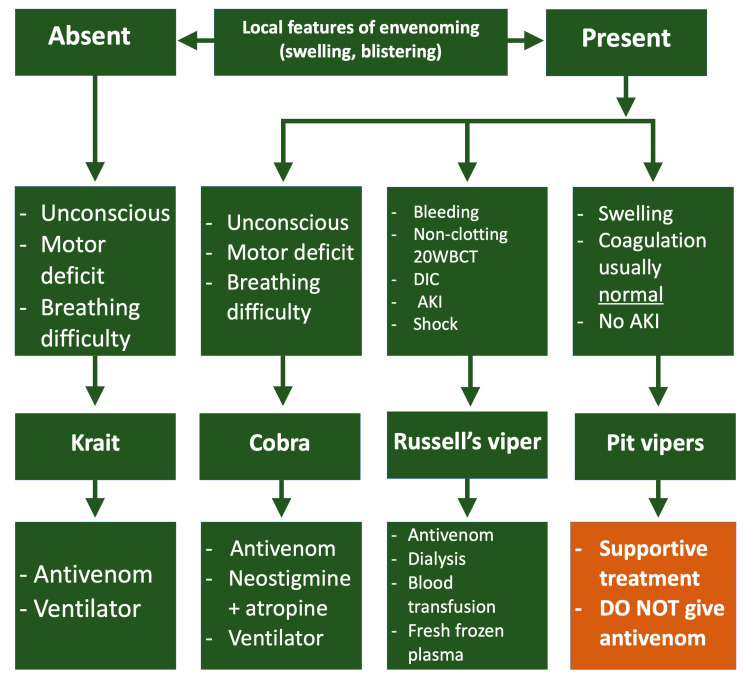 Figure 2
Figure 2| Parameter | Patient result | Reference range |
| 20WBCT | Clotted at 20 minutes | Clotting within 20 minutes = normal |
| PT | 12.4 seconds | 11.0-13.5 seconds |
| INR | 1.0 | 0.8-1.2 |
| Platelets | 233 | 150-400 × 109/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenomous Animal Envenomation and Studies · Marine Invertebrate Physiology and Ecology · Healthcare and Venom Research
Introduction
Snakebites are a major cause of morbidity and mortality across South Asia [1,2]. In Nepal, bites cluster with monsoon season agricultural work; pit vipers prevail in hill, mountain and farmland regions, while elapids (e.g., cobras and kraits) and Russell’s vipers can be found in the Terai lowland plains [2]. The main clinical syndromes are haemotoxicity (typically vipers), neurotoxicity (cobras and kraits) and local tissue injury without systemic effects [1,3]. In Nepal, most pit viper bites present with predominantly local effects; clinically significant coagulopathy is rare, although prolonged coagulopathy has been documented after confirmed white‑lipped pit viper envenoming [4].
Haemotoxic envenoming can cause a venom‑induced consumption coagulopathy (VICC). An important initial test to help confirm haemotoxic envenoming is the 20‑minute whole blood clotting test (20WBCT), a simple bedside test where venous blood in a glass tube is left undisturbed for 20 minutes and assessed for clot formation. Results should be complemented by prothrombin time (PT) and international normalised ratio (INR) when available [2,5].
Indian polyvalent antivenom (ASV) is an equine‑derived, polyvalent antibody‑fragment preparation (F(ab’)₂) raised against the “Big Four” venoms. Clinical effectiveness depends on species coverage and timely administration [2,3]. Anaphylaxis is a frequent complication of ASV; intramuscular adrenaline and airway equipment must be immediately available at the bedside, with prophylactic adrenaline given before ASV unless contraindicated (e.g., older patients with suspected ischaemic heart or cerebrovascular disease) [2,6-8].
The World Health Organisation (WHO) and Nepal’s national guidance therefore emphasise a syndromic approach: treat systemic envenoming with ASV when a covered species is plausible; if not, prioritise supportive care and serial assessment, and consider transfer [2,3,9,10]. WHO and Nepal guidance caution that lay colour descriptions are unreliable for species diagnosis. Where possible, identification should rely on expert review of a specimen or photograph, but obtaining these can pose a risk and is difficult to obtain retrospectively. Thus, treatment decisions should remain syndrome‑led [2,3].
Case presentation
A 59-year-old woman with no comorbidities was bitten on the right ring finger while hand-cutting grass in the Terai farmland in eastern Nepal on day 1. She reported a green snake. Within an hour, she developed burning pain and progressive oedema from finger to forearm. There were no initial signs of spontaneous bleeding (e.g., mucosal bleeding, gastrointestinal bleeding or visible haematuria) and no signs of neurotoxicity (e.g., ptosis, bulbar weakness or respiratory involvement). Later on day 1, she reached a peripheral treatment centre. Examination showed two puncture marks on the right ring finger, with marked oedema of the right hand and forearm; the contralateral hand is shown for comparison (Figure 1).
Right hand (arrow) showing oedema extending beyond the wrist following a suspected pit viper biteThe left hand (cannulated) is shown for comparison.
Laboratory findings at presentation are summarised in Table 1.
Ten vials of ASV were infused; no immediate reaction occurred. She also received intravenous (IV) crystalloid fluids, analgesia, limb elevation and tetanus prophylaxis. She was transferred later on day 1 to a tertiary teaching hospital in eastern Nepal. On arrival, she remained stable and non-neurotoxic. Repeat coagulation tests, including 20WBCT, remained normal. Renal function, electrolytes and venous blood gases were within normal limits. She was monitored from day 1 to day 3 on the acute medical unit. She remained stable with no coagulopathy or neurotoxicity and was discharged home on day 4 with improving swelling.
Discussion
Indian polyvalent antivenom (ASV) is effective in neutralising the venom of most venomous snakes found in India and Nepal, known as the “Big Four”: the spectacled cobra (Naja naja), common krait (Bungarus caeruleus), Russell’s viper (Daboia russelii) and saw‑scaled viper (Echis carinatus).
Although coagulopathy has occasionally been reported after white-lipped pit viper (Trimeresurus albolabris) bites [4], the normal 20WBCT, PT and INR in this patient indicated a low likelihood of systemic envenoming. As ASV does not neutralise pit viper venom, its use in this context exposed the patient to risk without a realistic prospect of benefit. Supportive care with serial examination and repeat coagulation testing would have been safer and consistent with guideline recommendations.
To aid decisions under diagnostic uncertainty, the WHO Guidelines for the Management of Snakebites outline a syndromic pathway [2], depicted as a flowchart in Figure 2.
Flowchart outlining a basic syndromic approach to snakebite management in Nepal20WBCT: 20-minute whole blood clotting test, DIC: disseminated intravascular coagulation, AKI: acute kidney injuryBased on the Nepal Ministry of Health, National Guideline for Snakebite Management in Nepal (2019)
As per the syndromic approach (Figure 2), the significant swelling in the absence of neurotoxicity and coagulopathy indicated that she was likely bitten by a pit viper. The management of this case deviated from the national guidance because ASV was administered when coverage was unlikely [2,3]. The WHO‑endorsed syndromic management recommends ASV only when systemic envenoming is present and ASV coverage is plausible [2]. The clinical picture was of local effects only with normal coagulation: no haematuria, a clotting 20WBCT, normal PT/INR and no neurotoxicity, thus most consistent with pit viper envenoming. The patient‑reported “green” snake was supportive but should not, on its own, guide treatment [2,3]. Furthermore, observation without development of coagulopathy is typical of most pit viper bites. They generally present with local effects only; thus, supportive care with serial testing is appropriate [3,11].
The use of ASV requires careful risk‑benefit consideration given the high rate of acute reactions. In a Sri Lankan randomised controlled trial, 61% of patients developed reactions, with 33% classified as anaphylaxis [12]. In this case from Nepal, administering ASV without plausible coverage exposed the patient to substantial iatrogenic risk with little prospect of benefit. The absence of a reaction does not imply benefit, nor does it justify off‑pathway use.
Where coverage is plausible, early ASV can be life‑saving [2]. Where coverage is unlikely, supportive care is safer [2,3]. Serial PT/INR provides a baseline for escalation and de‑escalation, complementing the 20WBCT and allowing teams to identify emergent or worsening coagulopathy or bleeding [2,3,5]. In peripheral facilities with limited monitoring, predefined triggers (e.g., persistently non‑clotting 20WBCT, rising INR, new bleeding or haemodynamic instability) can aid transfer decisions [2,3].
At presentation, simple changes can make a big difference: ensure the 20WBCT is performed in a clean, dry glass tube [2,5], obtain PT/INR to establish baseline and track coagulation [2] and avoid unnecessary intramuscular injections and non‑steroidal anti‑inflammatory drugs (NSAIDs) in patients at bleeding risk [2]. Then, when ASV is indicated, it should be given by slow intravenous infusion [12] with prophylactic adrenaline [6] (unless contraindicated), under close observation [7,8]. These steps help to reduce predictable hazards in snakebite care and suspected haemotoxic envenoming.
Snakebite outcomes depend on systems as much as bedside care. In Nepal, community education and organised rapid transport shorten pre‑hospital delay and are associated with lower mortality [1]. Regional plans aim to accelerate these gains by 2030 [9,10]. In the eastern Terai, Sharma et al. reported that a multi‑stakeholder awareness programme (village sessions, female health volunteers, posters/leaflets and engagement of traditional healers) combined with a volunteer motorcycle transport scheme was associated with faster presentation and referral. It found a reduction in case fatality from 10.5% to 0.5% and a fall in incidence from 502 to 315 per 100,000 in targeted villages, with no change in control villages [1]. These findings are consistent with the WHO strategy and national guidance, which advise locally tailored education, promotion of early care‑seeking and structured referral and transport networks [1,9,10].
Procurement and referral pathways should reflect local ecology [3,10]. Stocking antivenom products that match regional species reduces unnecessary and potentially harmful exposure and preserves supplies for covered syndromes [3,10]. Seasonal surveillance, feedback from referral centres and regular review of bite patterns help maintain stock. Early presentation should be encouraged, and serial coagulation testing performed as soon as possible to help guide decision‑making [1,9,10].
Regular audit helps assess and improve the safety and effectiveness of ASV use in local hospitals. Research has identified the following metrics: proportion of 20WBCTs performed [2,5], availability and use of same‑day PT/INR in suspected VICC [2], documentation of coverage plausibility before ASV is given [2,3], documentation that prophylactic adrenaline was given or contraindicated [7,8], bedside availability of adrenaline at time of administration [6] and recorded reaction rates to ASV [6].
The case highlights a training gap in services that is modifiable. Focused, case‑based teaching on the syndromic approach [2,3] and correct 20WBCT technique [5] would reduce non‑beneficial use of ASV. Preparedness for anaphylaxis further improves safety when antivenom is indicated [2,6]. Iterative review against the discussed measures helps ensure a syndrome‑led approach, preserves ASV supplies and reduces unnecessary morbidity and mortality from suboptimal treatment.
Conclusions
Treat syndromes, not species, reserving ASV for envenoming when coverage is plausible. In suspected pit viper envenoming with local‑only syndrome and normal coagulation, ASV should be avoided; supportive care, serial coagulation, and early transfer when appropriate must be prioritised instead. Use 20WBCT in clean glass as the first‑line bedside test for VICC and complement with PT/INR when available. Early anaphylaxis with adrenaline prophylaxis (if indicated) should be anticipated when ASV is given, with adrenaline kept readily available at the bedside. Targeted, case‑based education for regional services on the ASV guidelines should be provided, integrated with community education, rapid transfer programmes and regular closed‑loop audit.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effectiveness of rapid transport of victims and community health education on snake bite fatalities in rural Nepal Am J Trop Med Hyg Sharma SK Bovier P Jha N Alirol E Loutan L Chappuis F 1451508920132356828710.4269/ajtmh.12-0750 PMC 3748471 · doi ↗ · pubmed ↗
- 2National Guidelines for Snakebite Management in Nepal Epidemiology and Disease Control Division Ministry of Health and Population(Nepal) 2025 Kathmandu, Nepal Department of Health Services, Ministry of Health and Population 242019 http://www.edcd.gov.np/uploads/resource/5dec 92fc 9e 365.pdf
- 3Guidelines for the Management of Snakebites New Delhi: WHO SEARO World Health Organization 2025 New Delhi, India World Health Organisation 242016 https://www.who.int/publications/i/item/9789290225300
- 4Retrospective documentation of a confirmed white-lipped green pit viper (Trimeresurus albolabris Gray, 1842) bite in the south-central hills of Nepal Wilderness Environ Med Pandey DP Ghimire A Shrestha BR 79853020193073715510.1016/j.wem.2018.11.001 · doi ↗ · pubmed ↗
- 5The 20-minute whole blood clotting test (20WBCT) for snakebite coagulopathy-a systematic review and meta-analysis of diagnostic test accuracy P Lo S Negl Trop Dis Lamb T Abouyannis M de Oliveira SS 015202110.1371/journal.pntd.0009657 PMC 840503234375338 · doi ↗ · pubmed ↗
- 6Adverse reactions to snake antivenom, and their prevention and treatment Br J Clin Pharmacol de Silva HA Ryan NM de Silva HJ 4464528120162625612410.1111/bcp.12739 PMC 4767202 · doi ↗ · pubmed ↗
- 7Low-dose adrenaline, promethazine, and hydrocortisone in the prevention of acute adverse reactions to antivenom following snakebite: a randomised, double-blind, placebo-controlled trial P Lo S Med de Silva HA Pathmeswaran A Ranasinha CD 08201110.1371/journal.pmed.1000435 PMC 309184921572992 · doi ↗ · pubmed ↗
- 8Management of Snake Bite: Standard Treatment Guidelines Ministry of Health and Family Welfare Government of India 2025 New Delhi, India National Health Mission 292017 http://qps.nhsrcindia.org/sites/default/files/2021-05/Management%20of%20Snake%20Bite.pdf