Staged approach to bilateral severe carotid stenosis: a case report and literature review
Heitor Cabral Frade, Manmeet Kaur, Julia Aigbogun, Muhammad Zeeshan Memon, Arun Chhabra, Akm Muktadir, Hashem Shaltoni

TL;DR
A staged approach to treating severe blockages in both carotid arteries may reduce risks like hyperperfusion syndrome compared to simultaneous treatment.
Contribution
This case report and literature review highlight the benefits of staged bilateral carotid artery stenting in reducing complications.
Findings
Staged bilateral carotid artery stenting (BCAS) may reduce periprocedural complications like hyperperfusion syndrome.
The patient achieved functional independence after undergoing a staged BCAS approach.
Both simultaneous and staged BCAS are feasible, but staged BCAS appears safer in certain cases.
Abstract
Carotid atherosclerotic disease (CAD) is a major cause of stroke, often requiring a combination of medical and surgical interventions. Current guidelines have established well the role of interventions such as carotid endarterectomy and carotid artery stenting (CAS) for unilateral carotid disease. However, there is still a paucity of evidence on the timing, procedural order, and complication rate of these procedures when there is bilateral carotid involvement. Hyperperfusion syndrome (HPS), with or without associated intracerebral hemorrhage, although rare, is a major source of morbidity and mortality after carotid interventions, especially in the setting of bilateral CAD. In select cases, staged bilateral CAS (BCAS) appears to attenuate periprocedural risks, including HPS. A 62-year-old male presented with acute dysarthria and right-sided face and upper extremity weakness, amounting…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
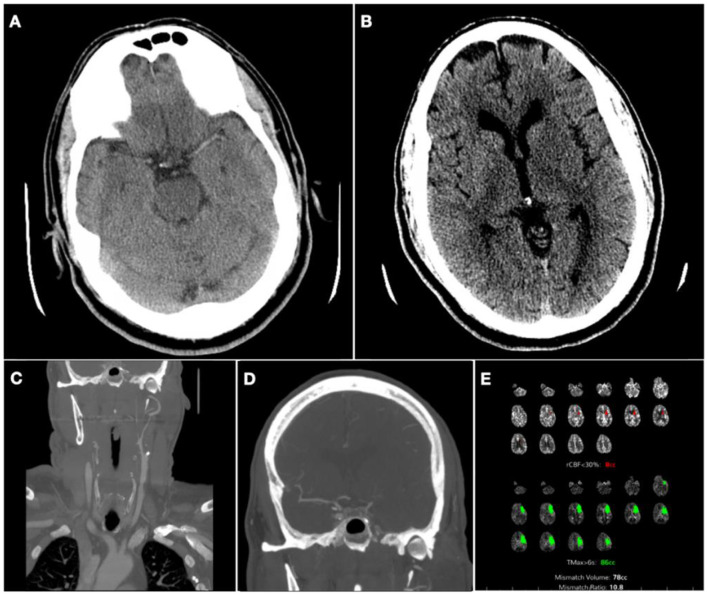 Figure 1
Figure 1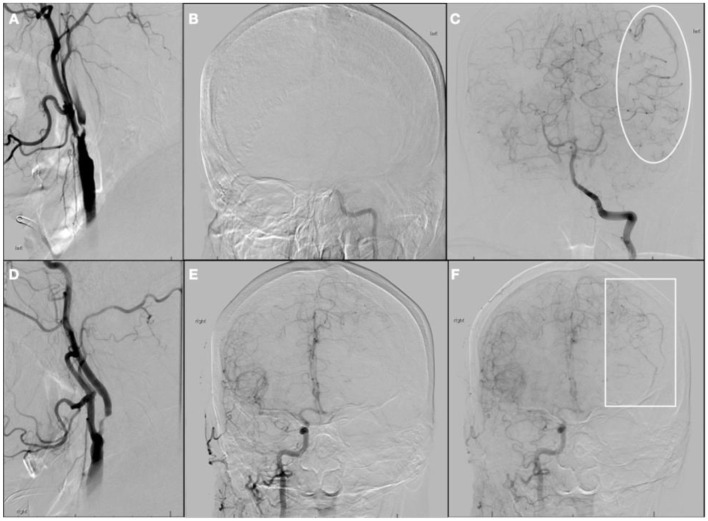 Figure 2
Figure 2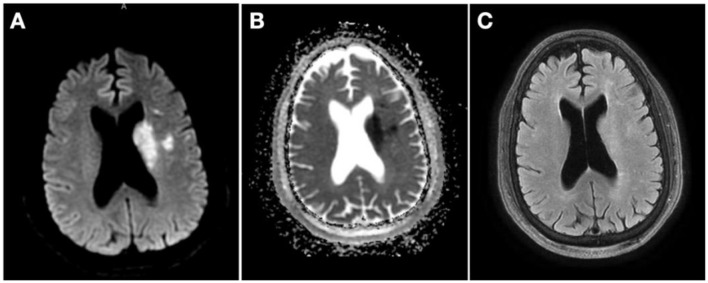 Figure 3
Figure 3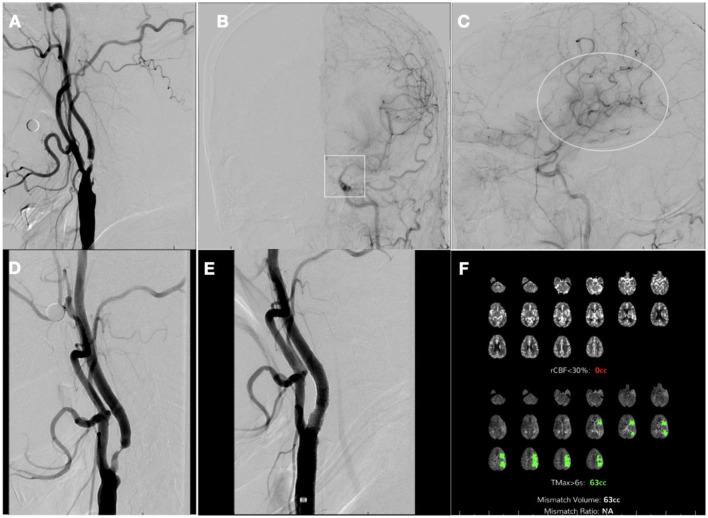 Figure 4
Figure 4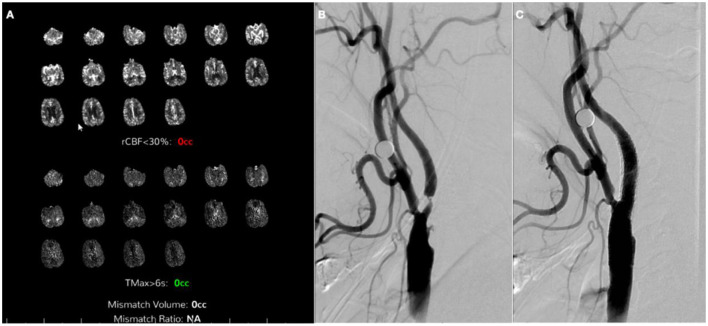 Figure 5
Figure 5|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
|
| ||||||
|
| 9 | SimBCAS (9) | 0 | 0 | 0 | 0 |
|
| 10 | SimBCAS (10) | 0 | 0 | 0 | 0 |
|
| 39 | SimBCAS (39) | 1 (2.6%) | 2 (5.1%) | 1 (2.6%) | 1 (2.6%) |
|
| 3 | Staged BCAS | 0 | 0 | 0 | 0 |
|
| 57 | SimBCAS (17) | 1 (5.8%) | 1 (5.8%) | 1 (5.8%) | 2 (11.7%) |
| Staged BCAS (40) | 1 (2.5%) | 0 | 0 | 0 | ||
|
| 2 | Staged ipsilateral CEA, contraleral CAS | 1 (50%) | 0 | 0 | 0 |
|
| 120 | SimBCAS (120) | 3 (2.5%) | 5 (4.2%) | 1 (0.8%) | 1 (0.8%) |
|
| 27 | SimBCAS (21), staged BCAS (6) | 0 | 1 (3.7%) | 0 | 0 |
|
| 42 | SimBCAS (42) | 2 (4.8%) | 1 (2.4%) | 0 | 0 |
| Staged BCAS (26) | 0 | 1 (3.8%) | 0 | 0 | ||
|
| 30 | SimBCAS (24) | 4 (16.7%) | 2 (8.3%) | NR | 1 (4.2%) |
| Staged BCAS (6) | 0 | 0 | NR | 0 | ||
|
| 12 | SimBCAS (8) | 0 | 0 | 0 | 0 |
| Staged BCAS (4) | 0 | 0 | 0 | 0 | ||
|
| 39 | SimBCAS (39) | 2 (5.1%) | 2 (5.1%) | 0 | 0 |
|
| 6 | SimBCAS (6) | 0 | 0 | 0 | 0 |
|
| 8 | Same-day ipsilateral CEA, contralateral CAS (5) | 1 (20%) | 0 | 0 | 0 |
| Same-day contralateral CAS, ipsilateral CEA (3) | 0 | 0 | 0 | 0 | ||
|
| 70 | SimBCAS (70) | 4 (5.7%) | 1 (1.4%) | 0 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and Carotid Artery Diseases · Oropharyngeal Anatomy and Pathologies · Cardiovascular Health and Disease Prevention
Introduction
Carotid atherosclerotic disease (CAD) is responsible for 15%−20% of strokes (Chaturvedi et al., 2005), which has motivated several interventional trials over the last decades. Although relatively rare to justify screening in asymptomatic individuals, CAD in its various forms—intima-media thickening, carotid plaque, carotid stenosis—has increased by ~60% between 2000 and 2020 (Song et al., 2020).
Several guidelines have addressed carotid artery stenosis treatment with intensive medical management or surgical management based on symptoms and severity of stenosis (Abbott et al., 2015). In acute symptomatic occlusions, carotid artery stenting (CAS) and carotid endarterectomy (CEA) with or without prior intravenous thrombolysis (IVT) provide the best recanalization and functional outcomes when compared to IVT or intra-arterial thrombolysis alone (Bonati et al., 2021). However, there is a paucity of evidence addressing symptomatic CAD when there is bilateral severe carotid stenosis, which is known to have higher risks of cerebral hyperperfusion syndrome (HPS) with or without intracerebral hemorrhage (ICH; Ouriel et al., 1999; Son et al., 2013).
HPS is a rare but potentially fatal complication of carotid revascularization through different methods. It is attributed to a post-procedural increase in cerebral blood flow associated with impaired cerebrovascular autoregulation. Clinically, it may present with headache, seizures, or transient neurologic dysfunction. Perfusion imaging may reveal a significant interval increase in cerebral blood flow. In some cases, HPS may be associated with ICH and almost always with poor outcomes (Moulakakis et al., 2009).
Multiple strategies for how to approach bilateral carotid stenosis with different combinations of simultaneous or staged CEA and CAS have been reported by different centers (Fukuda et al., 2003; Henry et al., 2005; Liu et al., 2015; Oshita et al., 2020). In a large prospective study of 747 patients with unilateral and bilateral carotid disease, 78 patients were treated for bilateral CAD by initially stenting the symptomatic carotid, followed by stenting the contralateral carotid, and had complication rates similar to the patients with unilateral CAD (Diehm et al., 2008).
Although intervention on the symptomatic carotid artery is still the standard approach in cases of bilateral severe carotid stenosis, there might be a role for an intervention of the asymptomatic carotid artery first in select cases as has been reported in a more recent case series. Eight patients with bilateral carotid stenosis underwent simultaneous CEA and CAS in two distinct orders according to clinical and angiographic characteristics. Patients who had a favorable angiographic profile underwent CEA of the symptomatic side followed by contralateral CAS. If pre-procedure angiography showed blood flow to the symptomatic anterior cerebral artery (ACA) coming from contralateral circulation via the anterior communicating artery (Acomm), the contralateral carotid artery would be intervened first by CAS, followed by CEA of the symptomatic side. Although none of the eight participants suffered ischemic complications or death, one of the five patients who had CEA of the symptomatic side first developed HPS (Xu et al., 2016).
Staged bilateral carotid stenting is a technique used in treating bilateral CAD that involves performing angioplasty and stenting on one carotid artery at a time, with an interval between procedures. This approach has been suggested in cases of bilateral carotid artery stenosis to reduce the risk of complications associated with simultaneously treating both arteries, such as intraoperative hemodynamic depression, HPS, or ICH.
We hereby report a case of acute stroke associated with severe bilateral carotid stenosis that was managed with IVT followed by staged bilateral CAS, starting with the asymptomatic carotid artery.
Case report
A 62-year-old male with a history of hypertension, atrial fibrillation post-ablation not on anticoagulation, and HIV on highly active antiretroviral therapy woke up with dysarthria and right-sided upper extremity and facial weakness. He was immediately taken to our hospital, ~7.5 h after last seen normal and 4 h from the midpoint of sleep. The National Institute of Health Stroke Scale (NIHSS) score at presentation was 6. Non-contrast head computerized tomography showed a dense left middle cerebral artery (MCA) sign (Figure 1A) and decreased gray-white matter differentiation on the left lentiform nucleus, with an Alberta Stroke Program Early CT Score of 9 (Figure 1B). Computed tomography (CT) angiogram showed severe right ICA stenosis and complete occlusion of the left proximal ICA (Figure 1C). There was a tandem occlusion of the M1 segment of the left MCA, but the left proximal ACA was perfused via a patent Acomm (Figure 1D).
Pre-thrombolytic non-contrast computerized tomography (CT), CT angiogram (CTA), and CT perfusion (CTP). (A) Axial CT head showing left dense middle cerebral artery (MCA) sign; (B) Axial CT Head, showing decreased gray-white matter differentiation on left lentiform nucleus; (C) CTA of neck coronal view: proximal left internal cerebral artery occlusion; (D) flow reconstitution of distal ICA flow and occlusion of proximal left MCA. (E) CTP showing core of 8cc, penumbra of 86cc, and mismatch ratio 10.8 on the left MCA territory.
CT perfusion (CTP) was pursued to guide acute management, and it showed a core infarct volume of 8cc in the left MCA territory and a penumbra volume of 86cc, with a mismatch volume of 78cc and a ratio of 10.8 (Figure 1E). Upon those findings, the patient received IVT and was taken to the neurointerventional suite for possible mechanical thrombectomy (MT) of the left ICA.
During the cerebral angiogram, performed under moderate sedation, he was noted to have progressive improvement of symptoms, with near-total resolution of expressive aphasia and dysarthria and an NIHSS score of 3. Digital subtraction images revealed a near-complete occlusion of the proximal left ICA (Figure 2A), with tandem occlusion of the left terminal ICA (Figure 2B). There was flow to the MCA territory through leptomeningeal collaterals from the posterior cerebral arteries (Figure 2C). There was also severe proximal right ICA stenosis (Figure 2D). There was partial collateral flow to the left terminal carotid branches via the patent anterior communicating complex (Figure 2E) and leptomeningeal collaterals off the left anterior cerebral arteries (Figure 2F). The risks of acute endovascular intervention were deemed to outweigh the benefits in the setting of rapidly improving symptoms and NIHSS score of 3, upon partial recanalization after IVT, so the procedure was aborted.
Digital subtraction angiogram at initial presentation. (A) Left common carotid artery (CCA) injection, neck lateral view; (B) Left CCA injection, head anterior-posterior (AP) view showing non-opacification of terminal left internal carotid artery (ICA); (C) Left vertebral artery injection, head AP view, with collateral supply to middle cerebral artery (MCA) territory on late arterial phase (ellipse); (D) Right CCA injection, neck lateral view; (E) Right CCA injection, head AP view showing cross-filling of L anterior cerebral artery on early arterial phase; (F) Right CCA injection, head AP view showing collateral supply to MCA territory on late arterial phase (rectangle).
The patient was admitted for further stroke management and remained clinically stable, with residual deficits of mild right upper extremity weakness and mild expressive aphasia. Brain magnetic resonance imaging (MRI) obtained ~12 h after presentation confirmed small acute infarcts on the left subcortical frontal lobe and basal ganglia (Figures 3A–C). The patient was started on dual antiplatelet therapy with aspirin and clopidogrel 24 h after IVT.
Magnetic resonance imaging (MRI) 12 h from presentation. (A) MRI diffusion-weighted imaging showing multiple hyperintense foci on left basal ganglia and left subcortical frontal lobe; (B) MRI apparent diffusion coefficient with corresponding hypointensity in the same territories; (C) MRI fluid-attenuated inversion recovery showing mild hyperintensity in the same territories.
One week later, the patient underwent a repeat diagnostic cerebral angiogram to reevaluate severe bilateral carotid stenosis, which revealed persistent severe cervical left ICA stenosis (Figure 4A) but interval recanalization of the left ICA terminus and associated early hyperemia within left MCA territory (Figures 4B, C). The risks of revascularization of the proximal left ICA, given the risk of hyperperfusion, were discussed with the patient, as well as the potential benefit from contralateral ICA stenting in light of the interhemispheric cross-filling. The decision was made to pursue two-stage stenting, starting with the asymptomatic severe right proximal ICA stenosis, followed by the left ICA. The patient underwent successful right ICA stenting without complications (Figures 4D, E) and had an uneventful overnight ICU stay with no neurological or hemodynamic alterations. A repeat CTP the next day showed no core yet a still large penumbra area at risk (Tmax > 6 s) on the MCA territory, 63cc (Figure 4F). He was discharged that day following the procedure with plans to return to undergo stenting of the left internal carotid.
Digital subtraction angiography 1 week after initial presentation and post-stenting computerized tomography perfusion (CTP). (A) left common carotid artery (CCA) injection, neck lateral view; (B) left CCA injection, head anterior–posterior view showing terminal left internal carotid artery (ICA) recanalization (square); (C) left CCA injection, lateral view showing early hyperemia on left middle cerebral artery (MCA) territory (ellipse); (D) right CCA injection, neck lateral view pre-stenting; (E) right CCA injection, neck lateral view post-stenting; (F) CTP 1 day after right ICA stenting showing no core and penumbra of 63cc on left MCA territory.
Four weeks after the first procedure, the patient was readmitted for the second stage of stenting. There was interval clinical improvement with only residual minimal aphasia. The patient finally underwent left ICA stenting without complications (Figure 5). On a 90-day follow-up assessment, the patient continued to improve to full resolution of previous weakness and speech impairment and was able to resume their previous activities.
Computerized tomography perfusion (CTP) and digital subtraction angiography 1 month after contralateral stenting. (A) CTP 28 days after right internal carotid artery stenting showing no core or penumbra on left middle cerebral artery territory; (B) Left common carotid artery (CCA) injection, neck lateral view pre-stenting; (C) Left CCA injection, neck lateral view post-stenting.
Discussion
The management of bilateral severe carotid stenosis has not been separately addressed by the different guidelines on CAD management over the last two decades (Abbott et al., 2015; Bonati et al., 2021), although single-center experience reports have suggested different approaches may be feasible. We decided to report this case due to our unique approach involving intravenous thrombolytic use, fighting the temptation to pursue mechanical thrombectomy, and the delayed staged stenting of both carotid arteries, starting with the asymptomatic side to prevent the risk of hyperperfusion, based on clinical improvement and angiographic collateral flow.
Our patient presented in the morning of symptom recognition after last seen well the prior evening at bedtime. Despite the unclear timing of symptom onset, wake-up strokes have now been addressed by different randomized clinical trials (Davis et al., 2008; Ma et al., 2019; Ringleb et al., 2019; Thomalla et al., 2018). After the publication of the WAKE-UP trial, some of these trials lost clinical equipoise and had to be terminated before achieving their predetermined sample size. Nonetheless, a meta-analysis of four trials that used CT or MRI-based perfusion methods to indicate thrombolytic use showed benefits in functional outcomes (Campbell et al., 2019).
Despite the patient also planning for endovascular intervention for acute proximal left ICA occlusion (ICAO) with initially evolving deficits, the interval clinical improvement associated with recanalization of proximal ICA, as well as angiographic evidence of collateral supply to main left MCA territory through Acomm and leptomeningeal vessels, leading to the deferral of the procedure. In acute ICAO, CAS performance has been reported mostly in retrospective single-center studies, with excellent recanalization rates and worse outcomes, particularly in tandem occlusions (Jovin et al., 2005). Successful recanalization is known to be affected by factors such as length of the occlusion, composition of thrombus or plaque, and adequacy of collateral circulation (Tang et al., 2022).
Besides the technical difficulties, even successful recanalization of acute cervical ICAO may be associated with complications such as procedural hemodynamic depression, myocardial infarction (MI), and HPS following the procedure. HPS has been associated with symptomatic stenosis of >90%, contralateral stenosis ≥80%, and poor intracerebral collaterals (Abou-Chebl et al., 2004; Coutts et al., 2003). Our patient had all these risk factors except for a relatively preserved collateral flow, predominantly through Acomm, yet it was diminished due to the severe right carotid stenosis.
To date, there have been 15 single-center case series of patients undergoing simultaneous or staged bilateral carotid interventions in which authors accounted for hyperperfusion syndrome as a potential complication (Table 1). Most of these series evaluated only simultaneous bilateral CAS (SimBCAS), but four included both SimBCAS and staged bilateral carotid stenting (BCAS) with segregated outcomes (Henry et al., 2005; Li et al., 2014; Liu et al., 2010; Oshita et al., 2020). Across all series, HPS was only reported in one case of staged BCAS (Henry et al., 2005), while it affected up to 16% of cases of SimBCAS (Henry et al., 2005; Li et al., 2014; Liu et al., 2010; Oshita et al., 2020). There was no fatal outcome in the patients who underwent staged BCAS, but there were two deaths in patients who had SimBCAS, one of which was attributed to HPS (Henry et al., 2005).
Among patients who undergo bilateral staged interventions, several approaches have been reported by different centers (Diehm et al., 2008; Fukuda et al., 2003; Liu et al., 2015; Xu et al., 2016). In a series of eight patients with bilateral carotid stenosis who underwent same-day CEA of the symptomatic side and CAS of the asymptomatic side, the authors opted to start with CAS of the asymptomatic side in three patients that had ACA of the side planned to undergo CEA supplied by contralateral side, similarly to our approach in this case. The remaining five patients had CEA of the symptomatic side first. Although both groups did not suffer stroke, MI, or death, there was one case of hyperperfusion injury in the group that had CEA of the symptomatic carotid first (Xu et al., 2016).
We opted to pursue our first stage a few days later and the second stage 4 weeks after the first intervention. The timing of intervention in symptomatic carotid stenosis has been a topic of debate among interventionists, but a recent systematic review suggests better outcomes when it is pursued within 2 weeks of first symptoms (Rerkasem et al., 2020). There has been no consensus, however, on the optimal timing of the second procedure in staged BCAS. Five case series reported the timing of staged CAS in a total of 75 patients. Except for one of these studies, in which patients had a staged intervention done 24 h to 1 week after the first procedure (Henry et al., 2005), all the other studies reported second-stage CAS 1–12 weeks after the first intervention (Hashimoto et al., 2023; Henry et al., 2005; Hokari et al., 2014; Li et al., 2014; Oshita et al., 2020).
Although this has not been the first case of staged stenting starting from the asymptomatic side (Hashimoto et al., 2023; Xu et al., 2016), it is the first case to the authors' knowledge in which a patient preemptively received IVT in extended window before planned staged BCAS with interval improvement in ipsilateral anterograde flow, as well as improvement in perfusion imaging suggestive of optimized collateral flow and cerebrovascular autoregulation.
Our approach may not be extrapolated to every case of bilateral severe carotid stenosis, but it highlights the importance of staged stenting in bilateral carotid stenosis due to the higher risk of HPS. In selected cases, this could be attenuated by CAS of the asymptomatic carotid first, followed by delayed stenting of the symptomatic carotid after optimization of collateral flow based on angiographic and perfusion imaging.
Conclusion
Carotid artery stenosis is a major risk factor for stroke. Bilateral carotid artery stenosis poses a challenge to interventionists in deciding the optimal approach, sequence, and timing of bilateral procedures due to the additional risk of hyperperfusion syndrome even after uncomplicated recanalization. In these patients, a tailored approach based on the patient's symptomatic side and angiographic and perfusion imaging features may provide the safest approach to avoid hyperperfusion, often starting with the intervention of the asymptomatic carotid side.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbott A. L.Paraskevas K. I.Kakkos S. K.Golledge J.Eckstein H. H.Diaz-Sandoval L. J.. (2015). Systematic review of guidelines for the management of asymptomatic and symptomatic carotid stenosis. Stroke 46, 3288–3301. 10.1161/STROKEAHA.115.00339026451020 · doi ↗ · pubmed ↗
- 2Abou-Chebl A.Yadav J. S.Reginelli J. P.Bajzer C.Bhatt D.Krieger D. W. (2004). Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: risk factors, prevention, and treatment. J. Am. Coll. Cardiol. 43, 1596–1601. 10.1016/j.jacc.2003.12.03915120817 · doi ↗ · pubmed ↗
- 3Alurkar A.Karanam L. S. P.Nayak S.Oak S. (2012). Simultaneous bilateral carotid stenting in a series of 9 patients: a single-center experience with review of literature. J. Clin. Imaging Sci. 2:72. 10.4103/2156-7514.10430523393629 PMC 3551520 · doi ↗ · pubmed ↗
- 4Bonati L. H.Kakkos S.Berkefeld J.de Borst G. J.Bulbulia R.Halliday A.. (2021). European Stroke Organisation guideline on endarterectomy and stenting for carotid artery stenosis. Eur. Stroke J. 6, I–XLVII. 10.1177/2396987321101212134414302 PMC 8370069 · doi ↗ · pubmed ↗
- 5Campbell B. C. V.Ma H.Ringleb P. A.Parsons M. W.Churilov L.Bendszus M.. (2019). Extending thrombolysis to 4·5–9 h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data. Lancet 394, 139–147. 10.1016/S 0140-6736(19)31053-031128925 · doi ↗ · pubmed ↗
- 6Chaturvedi S.Bruno,; A., Feasby,; T., Holloway,; R., Benavente,; O., Cohen,; S. N.,. (2005). Carotid endarterectomy-an evidence-based review report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Am. J. Opthalmol. 41, 238–239. 10.1016/j.ajo.2005.11.03116186516 · doi ↗ · pubmed ↗
- 7Chen M. S.Bhatt D. L.Mukherjee D.Chan A. W.Roffi M.Kapadia S. R.. (2004). Feasibility of simultaneous bilateral carotid artery stenting. Catheteriz. Cardiovasc. Interv. 61, 437–442. 10.1002/ccd.1074215065133 · doi ↗ · pubmed ↗
- 8Coutts S. B.Hill M. D.Hu W. Y.Sutherland G. R.Findlay J. M.Dempsey R. J.. (2003). Hyperperfusion syndrome: toward a stricter definition. Neurosurgery. 53, 1053–1058. 10.1227/01.NEU.0000088738.80838.7414580271 · doi ↗ · pubmed ↗