ST-Segment Elevation Myocardial Infarction After Pegfilgrastim: Case Report and Review of Mechanistic Considerations
Collin Goetze, Henryk Dreger, Cheng-Ying Chiu

TL;DR
A cancer patient developed a heart attack after receiving pegfilgrastim, possibly due to high white blood cell and platelet counts causing blood clotting issues.
Contribution
First reported case of ST-segment elevation myocardial infarction linked to pegfilgrastim, highlighting a rare thromboembolic complication.
Findings
Acute STEMI occurred in a patient after pegfilgrastim, with coronary artery occlusion and no atherosclerosis.
Leukocytosis and thrombocytosis likely triggered the myocardial infarction via hyperviscosity and endothelial activation.
Thrombectomy improved blood flow, suggesting its value in such cases.
Abstract
Granulocyte-colony stimulating factors (G-CSFs) are widely used to prevent chemotherapy-induced neutropenia, but they have been linked to coronary neovascularization and prothrombotic effects. A 62-year-old man with small cell lung cancer developed an acute posterior ST-segment elevation myocardial infarction (STEMI) 1 day after receiving 6 mg of pegfilgrastim during his second chemo-immunotherapy cycle. Coronary angiography revealed an occluded right coronary artery without atherosclerosis. Aspiration thrombectomy significantly reduced thrombus burden, restoring TIMI flow grade 3. Initial blood tests showed leukocytosis (white blood cells: 82.13 × 109/L) and thrombocytosis (platelets: 773 × 109/L), which normalized at discharge. Transesophageal echocardiography excluded embolic sources, and hyperviscosity syndrome was considered. Marked leukocytosis and thrombocytosis after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
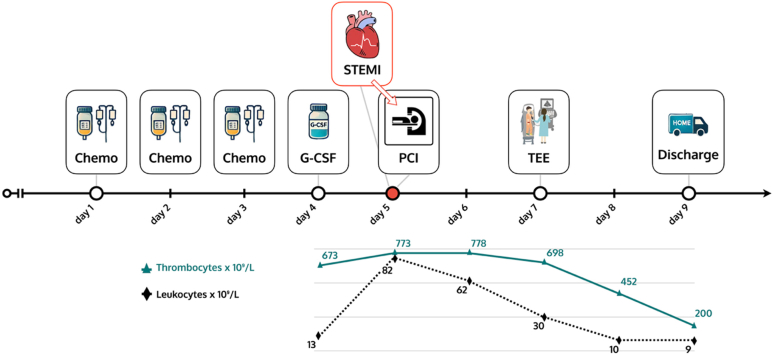 Figure 1
Figure 1 Figure 2
Figure 2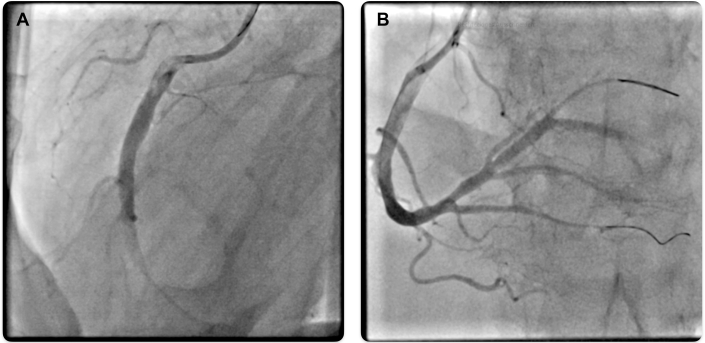 Figure 3
Figure 3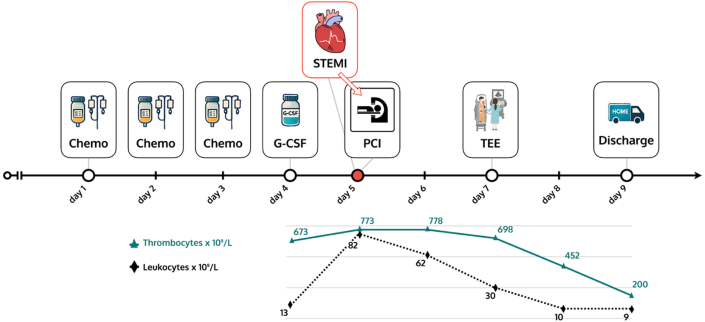 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeutropenia and Cancer Infections · Blood disorders and treatments · Chemotherapy-induced cardiotoxicity and mitigation
Visual SummaryTimeline Illustrating the Clinical Course and Laboratory DynamicsG-CSF = granulocyte-colony stimulating factor; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction; TEE = transesophageal echocardiography.
History of Presentation
A 62-year-old man presented with typical angina pectoris at the emergency department by ambulance. The electrocardiogram at admission showed ST-segment elevations in the inferior leads (Figure 1), and the patient was directly transferred to the cardiac catheterization laboratory.Take-Home Messages
- •G-CSF therapy, although an effective treatment for neutropenia, may in rare cases lead to leukocytosis-associated thromboembolic events, warranting careful monitoring in cancer patients.
- •This first documented case of STEMI after pegfilgrastim underscores the importance of recognizing and managing potential cardiovascular complications in vulnerable populations, with thrombectomy as a valuable adjunctive tool. Figure 1. Twelve-Lead ECG at Time of PresentationECG shows sinus rhythm with ST-segment elevation in leads II, III, and aVF and ST-segment depression in leads aVL and V_2_ to V_4_. ECG = electrocardiogram.
Past Medical History
The patient had been discharged from the department of pulmonology the day before, where he received the second cycle of systemic chemo-immunotherapy for metastatic small cell neuroendocrine lung carcinoma. The chemo-immunotherapy regimen included carboplatin, etoposide, and atezolizumab. Additionally, 6 mg of pegfilgrastim had been administered subcutaneously on day 4, which was the day before the presentation in our emergency department. Laboratory tests at the time of pegfilgrastim administration showed a slightly elevated white blood cell (WBC) and platelet count (WBCs: 13 × 10^9^/L, platelets: 673 × 10^9^/L).
The patient had no cardiac history except for paroxysmal atrial fibrillation and arterial hypertension. With a CHA_2_DS_2_-VA score of 1, anticoagulation had been omitted. Prior chest computed tomography scans performed for lung cancer staging did not reveal any calcified coronary plaques, thus no formal coronary calcium scoring had been performed.
Differential Diagnosis
Differential diagnosis included acute coronary syndrome from plaque rupture or erosion, thromboembolism or coronary spasm, as well as immune checkpoint inhibitor–associated pericarditis and myocarditis.
Investigations
Immediate cardiac catheterization was performed. Coronary angiography revealed an acute embolic occlusion of the right coronary artery (Figure 2A). Laboratory tests on admission revealed significantly elevated WBC (82.13 × 10^9^/L) and platelet counts (773 × 10^9^/L).Figure 2. Coronary Angiography(A) Coronary angiogram showing 99% occlusion of the RCA. (B) Coronary angiogram after thrombus aspiration in the mid-RCA, RPL, and PDA using the CAT RX aspiration catheter (Penumbra) and stent implantation in the RPL with TIMI flow grade 3. PDA = posterior descending artery; RCA = right coronary artery; RPL = right posterolateral branch.
Management
Successful retrieval of a macroscopically white thrombus from the right coronary artery was performed with CAT RX aspiration catheter (Penumbra). Given the ongoing high thrombus burden, balloon dilation in the posterior descending artery and the right posterolateral branch was performed, followed by additional thrombus aspiration. Because of a suspected vascular dissection in the right posterolateral branch, a 3.0 × 15 mm stent was implanted. Subsequently, a very good primary outcome with a TIMI flow grade 3 was observed (Figure 2B). The left coronary artery was unremarkable.
Transesophageal echocardiography was performed and ruled out intracardiac thrombus or patent foramen ovale as embolic causes.
The patient had not received granulocyte-colony stimulating factor (G-CSF) during the first cycle of chemo-immunotherapy, and his WBC counts before were within normal range, so the observed leukocytosis was likely due to pegfilgrastim administration. Over time, the significantly elevated WBC count fell, showing 62 × 10^9^/L on day 1 post-STEMI, 30 × 10^9^/L on day 2, and returning to the normal range at 9.6 × 10^9^/L on day 3. His platelet count fell but remained elevated, with levels at 773 × 10^9^/L on admission, 778 × 10^9^/L on day 1, 698 × 10^9^/L on day 2, and 452 × 10^9^/L on day 3.
Outcome
The patient's symptoms regressed rapidly during his hospital stay. Both WBC and platelet counts were within normal range at discharge. He was discharged home in good health.
Discussion
G-CSF and its pegylated form, pegfilgrastim, are used to prevent chemotherapy-related neutropenia. By expanding neutrophils, G-CSF lowers infection risk and supports uninterrupted chemotherapy.1 However, the administration of G-CSF is potentially associated with adverse effects. Among the less common but serious complications are hematologic abnormalities such as leukocytosis,1^,^2 which may pose risks for thrombotic events.
Healthy stem cell donors receiving G-CSF have not demonstrated a significantly increased risk of thromboembolic events after the administration of G-CSF compared with the general population.2 However, an increased rate of cardiac events such as in-stent restenosis when administering G-CSF after percutaneous coronary intervention3 has been observed in high-risk cardiac patients, possibly explained by proinflammatory properties inducing plaque destabilization.4^,^5 In addition, case reports and small case series have described a temporal association of myocardial infarction (including non-STEMI after filgrastim),6 limb ischemia,7 and other ischemic complications7 with G-CSF administration, suggesting a prothrombotic signal. In the current case, onset of acute myocardial infarction (AMI) occurred after G-CSF administration—a temporal link that warrants further investigation.
G-CSF exerts multiple effects on the cardiovascular system, among which the effects on inflammation and coagulation are the most notable with respect to ischemic complications. Leukocytosis secondary to G-CSF administration can precipitate leukostasis and hyperviscosity, with microvascular obstruction.2^,^8 Studies have shown that the release of proinflammatory cytokines (eg, IL-1β, TNF-α) after G-CSF has been associated with endothelial activation and heightened adhesiveness as well as leukocyte infiltration with increased tissue factor expression and formation of neutrophil extracellular traps (NETs) driving the thrombosis-inflammation circuit. In addition, augmentation of functional platelet activity resulting in augmentation of platelet aggregation has been described.4^,^5^,^7^,^9 Complementing these human data, in vivo murine work has demonstrated G-CSF–triggered, inflammation-associated cardiac thrombosis in susceptible states (eg, iron-loaded myocardium), which is mitigated by statin therapy.9 Taken together, G-CSF–induced leukocytosis and G-CSF–driven inflammation can promote cardiovascular complications, such as cardiac thrombosis.
The concomitant administration of immune checkpoint inhibitors such as atezolizumab may further augment proinflammatory signaling, potentially enhancing the risk of vascular complications when combined with G-CSF. This is biologically plausible, as both drug classes act through pathways that could create a synergistic prothrombotic environment in a milieu of cancer-related inflammation and myelosuppressive therapy, thereby increasing the vulnerability to acute ischemic events.
AMI is usually linked to traditional risk factors such as hypertension, hyperlipidemia, diabetes, and obesity.6 It is notable that our patient had no significant cardiac history aside from paroxysmal atrial fibrillation and arterial hypertension. The absence of radiographic evidence of coronary atherosclerosis on prior computed tomography imaging strengthens the likelihood that the acute event was precipitated by treatment-related factors rather than progression of pre-existing obstructive coronary artery disease. The presence of atrial fibrillation indicates an elevated thromboembolic risk, especially in the absence of anticoagulation therapy, and the probability that the embolic STEMI was induced by atrial fibrillation is greater than in a comparable individual without atrial fibrillation. However, a CHA_2_DS_2_-VA score of 1 did not warrant anticoagulation, as the estimated annual thromboembolic risk of 1.9%10 is considered below the treatment threshold according to current guideline-based risk stratification. Our patient's low-risk cardiac profile underscores the unusual nature of the AMI in the context of pegfilgrastim administration and raises important considerations regarding the safety profile of G-CSF in relation to potential cardiac complications.
Conclusions
To our knowledge, this is the first reported case of STEMI directly after G-CSF/pegfilgrastim administration. This case highlights a potential link between G-CSF treatment and acute myocardial infarction in cancer patients without significant cardiovascular history. Although G-CSF remains a valuable therapy for managing chemotherapy-induced neutropenia, clinicians should be vigilant for rare thromboembolic complications, particularly in patients with predisposing factors. Further research is necessary to better understand these risks and define vulnerable populations. Given the rarity of such events, systematic pharmacovigilance reporting and the establishment of registry-based datasets are essential to better define the incidence, risk factors, and outcomes of G-CSF–associated cardiovascular complications.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mhaskar R.Clark O.A.Lyman G.Engel A.B.T.Morganti Paladini L.Djulbegovic B.Colony-stimulating factors for chemotherapy-induced febrile neutropenia Cochrane Database Syst Rev 2014102014 CD 00303910.1002/14651858.CD 003039.pub 2PMC 714117925356786 · doi ↗ · pubmed ↗
- 2Tigue C.C.Mckoy J.M.Evens A.M.Trifilio S.M.Tallman M.S.Bennett C.L.Granulocyte-colony stimulating factor administration to healthy individuals and persons with chronic neutropenia or cancer: an overview of safety considerations from the research on adverse drug events and reports project Bone Marrow Transplant 403200718519210.1038/sj.bmt.170572217563736 · doi ↗ · pubmed ↗
- 3Kang H.J.Kim H.S.Zhang S.Y.Effects of intracoronary infusion of peripheral blood stem-cells mobilised with granulocyte-colony stimulating factor on left ventricular systolic function and restenosis after coronary stenting in myocardial infarction: the MAGIC cell randomised clinical trial Lancet 3639411200475175610.1016/S 0140-6736(04)15689-415016484 · doi ↗ · pubmed ↗
- 4Janoudi A.Shamoun F.E.Kalavakunta J.K.Abela G.S.Cholesterol crystal induced arterial inflammation and destabilization of atherosclerotic plaque Eur Heart J 372520161959196710.1093/eurheartj/ehv 65326705388 · doi ↗ · pubmed ↗
- 5Steppich B.A.Demetz G.Schulz S.Effects of G-CSF on systemic inflammation, coagulation and platelet activation in patients with acute myocardial infarction Thromb Res 1272201111912110.1016/j.thromres.2010.11.00421095620 · doi ↗ · pubmed ↗
- 6Bilir C.Engin H.Temi Y.B.Toka B.KarabağT.Acute myocardial infarction caused by filgrastim: a case report Case Rep Oncological Med 201220121210.1155/2012/784128 PMC 354417423326742 · doi ↗ · pubmed ↗
- 7Eckman P.M.Bertog S.C.Wilson R.F.Henry T.D.Ischemic cardiac complications following G-CSF Catheterization Cardiovasc Interventions 76120109810110.1002/ccd.2245520578094 · doi ↗ · pubmed ↗
- 8Jao G.T.Knovich M.A.Savage R.W.Sane D.C.ST-Elevation myocardial infarction and myelodysplastic syndrome with acute myeloid leukemia transformation Tex Heart Inst J 412201423423710.14503/thij-12-290524808792 PMC 4004476 · doi ↗ · pubmed ↗