Neovaginal Diversion Colitis Successfully Treated With Mesalazine Suppositories: Endoscopic Documentation of Healing
Shinichiro Kawatoko, Marimo Mori, Junji Umeno

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
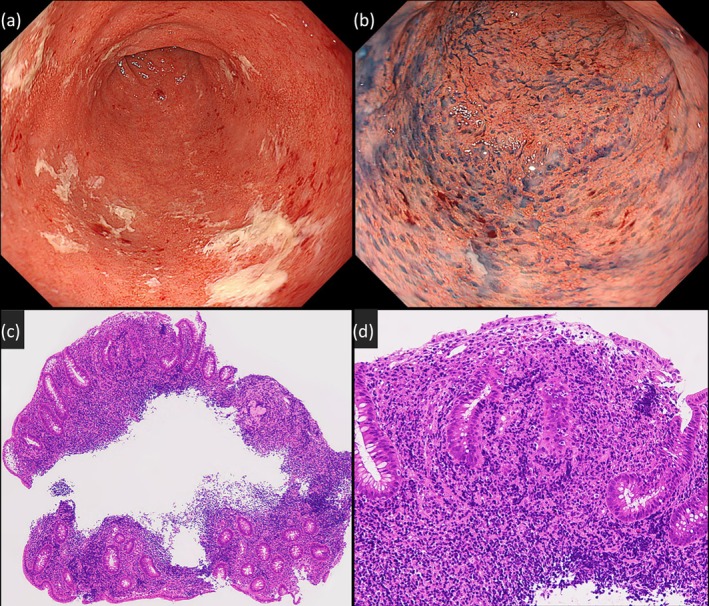 Figure 1
Figure 1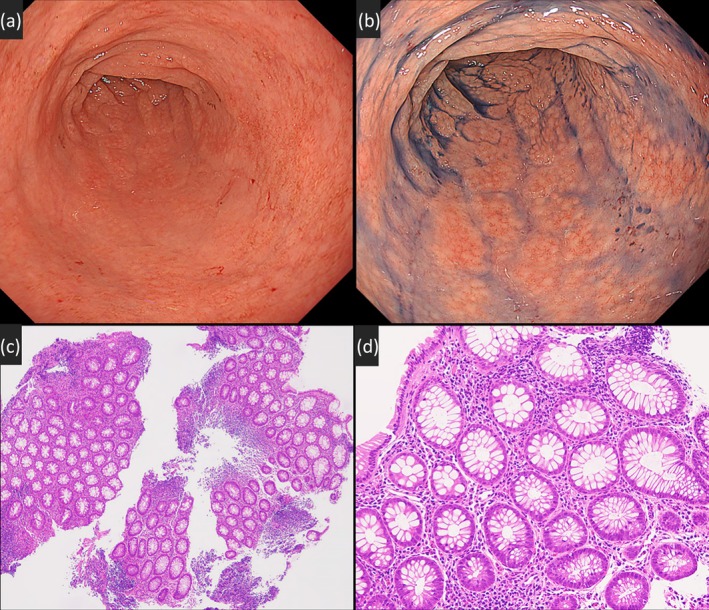 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGynecological conditions and treatments · Endometriosis Research and Treatment · Reproductive System and Pregnancy
A 41‐year‐old woman with Mayer–Rokitansky–Küster–Hauser syndrome (type I), a congenital absence of the uterus and upper vagina, underwent sigmoid colon vaginoplasty at age 18 and was followed at our gynecology department. She presented with a 10‐month history of intermittent neovaginal bleeding and dyspareunia. A manual neovaginal examination was unremarkable, but persistent symptoms prompted referral to our department (Gastroenterology) for further evaluation. Vaginoscopy (EVIS X1 and GIF‐XZ1200, Olympus Corp., Tokyo, Japan) revealed continuous erythema, edema, erosions, and loss of vascular pattern, resembling ulcerative colitis, in the neovaginal sigmoid colon (Figure 1a,b). Biopsy histology showed chronic active colitis with crypt distortion, cryptitis, and goblet cell depletion (Figure 1c,d). Bacterial culture and Treponema pallidum PCR were negative. Colonoscopy showed only minor aphthous erosions confined to the anal verge, with no lesions in the upstream rectum or colon. She had no gastrointestinal symptoms suggestive of ulcerative colitis, such as diarrhea, hematochezia, or abdominal pain. From these findings, she was diagnosed with isolated neovaginal diversion colitis. She was initially treated with intravaginal budesonide foam enemas (2 mg, once daily) for 7 weeks and advised to refrain from vaginal intercourse; however, symptoms persisted. Subsequently, mesalazine vaginal suppositories (1000 mg, once daily) were initiated with the aid of a vaginal prosthesis to facilitate drug delivery to the neovaginal blind end, resulting in marked symptom improvement within 1 week. Follow‐up vaginoscopy after 7 weeks demonstrated mucosal normalization, and histology confirmed resolution of inflammation (Figure 2). She resumed vaginal intercourse while continuing mesalazine suppositories, with only occasional trace bleeding and no other symptoms for 13 months. Neovaginal diversion colitis, also called “diversion neovaginitis,” may result from nutritional deprivation (e.g., short‐chain fatty acids) [1]. Despite treatments like short‐chain fatty acid enemas, mesalazine, or corticosteroids, no standardized treatment has been established [1, 2]. Accurate endoscopic and histological assessment enables effective medical management and preserves sexual function.
Author Contributions
Shinichiro Kawatoko designed the study, managed the patient's care, performed endoscopic evaluations, reviewed histological specimens, and drafted the manuscript. Marimo Mori and Junji Umeno critically reviewed and revised the manuscript for important intellectual content. All authors have read and approved the final version of the manuscript.
Funding
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1W. B. van der Sluis , M. B. Bouman , N. K. de Boer , B. M. Stubenitsky , D. M. de Leeuw , and A. A. van Bodegraven , “Diversion Neovaginitis After Sigmoid Vaginoplasty: Endoscopic and Clinical Characteristics,” Fertility and Sterility 105 (2016): 738–744.10.1016/j.fertnstert.2015.11.01326632208 · doi ↗ · pubmed ↗
- 2K. Tominaga , K. Kamimura , K. Takahashi , J. Yokoyama , S. Yamagiwa , and S. Terai , “Diversion Colitis and Pouchitis: A Mini Review,” World Journal of Gastroenterology 24 (2018): 1734–1747.29713128 10.3748/wjg.v 24.i 16.1734 PMC 5922993 · doi ↗ · pubmed ↗