Short-Term Outcomes of Cardiogenic Shock Treated With a Microaxial Flow Pump
Shunsuke Matsushita, Yuichi Sawayama, Kohei Osakada, Shunsuke Kubo, Yuichi Kawase, Takeshi Tada, Yasushi Fuku, Hiroyuki Tanaka, Kazushige Kadota

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
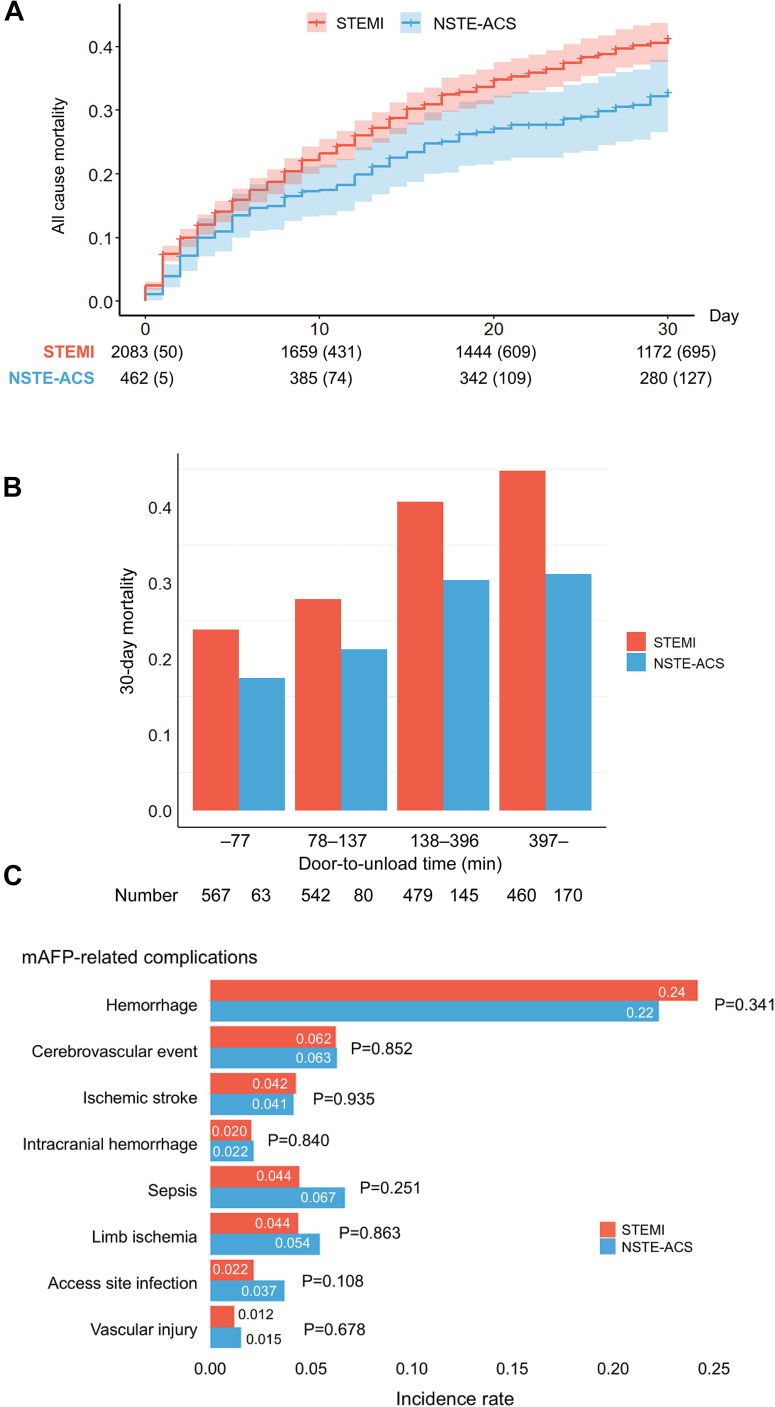 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Plasma and Flow Control in Aerodynamics · Refrigeration and Air Conditioning Technologies
The prognosis of acute coronary syndrome (ACS) has improved with reperfusion therapy advancements.1 However, patients presenting with cardiogenic shock (CS) continue to achieve poor outcomes, with in-hospital mortality rates of 40%-50%.1^,^2 Mechanical circulatory support devices, such as the microaxial flow pump (mAFP) (Impella, Abiomed), provide circulatory stability for patients with CS and are increasingly used in clinical practice.3 Robust clinical evidence was limited until recently, but the DanGer Shock (Danish–German Cardiogenic Shock) trial demonstrated mortality reduction with mAFP, clarifying its indications.4
Patients with non–ST-segment elevation acute coronary syndrome (NSTE-ACS) generally exhibit distinct pathophysiological characteristics from those with ST-segment elevation myocardial infarction (STEMI).5 Short-term prognosis varies in NSTE-ACS across studies,2^,^6, 7, 8 whereas mortality rates are consistently lower than in patients with STEMI.9 However, mortality rates remain alarmingly high in NSTE-ACS complicated by CS and may even exceed those of patients with STEMI with CS.2 Although mAFP is used for NSTE-ACS with CS, large-scale outcome data remain lacking.
Methods
We conducted a post hoc analysis using data from the J-PVAD (Japanese Registry for Percutaneous Ventricular Assist Devices), a nationwide registry of consecutive patients receiving mAFP in Japan. The study included patients treated for ACS and CS between February 1, 2020 and December 31, 2022. The study was approved by the Central Institutional Review Board (Osaka University, #17,232) and complied with the Declaration of Helsinki. The registry included 2,629 patients with ACS, of whom 2,545 patients met the inclusion criteria, including successful mAFP device insertion, identified ACS type, and available survival data. Patients were categorized into STEMI and NSTE-ACS groups. NSTE-ACS includes both non-STEMI and unstable angina. CS was defined as: 1) prolonged hypotension (systolic blood pressure [SBP] <90 mm Hg, the use of vasoactive inotropes to maintain SBP ≥90 mm Hg, or a ≥30-mm Hg decrease in SBP from baseline); and 2) signs of end-organ hypoperfusion. The primary endpoint was 30-day mortality after device implantation. Secondary outcomes included mAFP-related complications.
Adjusted HRs with 95% CIs were calculated with the Cox proportional hazard regression model. We included the following variables in the multivariable model: ACS type; age; sex; dyslipidemia; diabetes mellitus; prior ischemic stroke or transient ischemic attack; SBP at admission; out-of-hospital cardiac arrest; estimated glomerular filtration rate; simultaneous use of mAFP and extracorporeal membrane oxygenation (ECPELLA); door-to-unload time; and inotrope or vasopressor administration at mAFP placement.
Results
This study included 2,545 patients, with a mean age of 70 ± 12 years. Of the patients, 80% were male and 82% presented with STEMI (n = 2,083). Patients in the NSTE-ACS group were older than those in the STEMI group. Furthermore, the NSTE-ACS group exhibited a higher prevalence of atherosclerotic risk factors (Table 1). Regarding clinical presentation, patients with STEMI demonstrated lower SBP and higher lactate levels at admission. The utilization rate of inotropes and vasopressors at the initiation of mAFP was higher in the STEMI group (P < 0.001). Percutaneous coronary intervention was performed more frequently in STEMI, whereas coronary artery bypass graft was more common in NSTE-ACS. The duration of mAFP support was significantly longer in the STEMI group. Moreover, the median door-to-unload time was significantly shorter in the STEMI group. Treatment by ECPELLA was more frequent in the STEMI group than in the NSTE-ACS group. Figure 1A shows significantly higher 30-day mortality in STEMI than in NSTE-ACS (32% vs 26%, log-rank P = 0.01). STEMI was also independently associated with increased mortality in multivariable Cox analysis (HR: 1.46; 95% CI: 1.17-1.81; P < 0.001). When dividing into quartiles based on the door-to-unload time, the 30-day mortality was lower with shorter door-to-unload time, irrespective of ACS type (both P for trend < 0.05) (Figure 1B). Hemorrhage was the most prevalent complication (24%, n = 607), occurring at similar rates between groups (P = 0.34). Sepsis was reported in 123 patients (4.8%), with a lower incidence in the STEMI group (STEMI: 4.4% vs NSTE-ACS: 6.7%), although not statistically significant (Figure 1C).Table 1. Patient Characteristics and In-Hospital Management Based on Acute Coronary Syndrome TypesNOverall (N = 2,545)STEMI (n = 2,083)NSTE-ACS (n = 462)P ValueAge, y2,54572 (62-78)71 (61-78)74 (67-80)<0.001Male2,5452,031 (80)1,674 (80)357 (77)0.134Body mass index, kg/m^2^2,41823.5 (21.1-26.1)23.5 (21.2-26.1)23.5 (20.6-26.0)0.498Current smoker2,209802 (36)683 (38)119 (29)0.001Hypertension2,4221,652 (68)1,298 (66)354 (79)<0.001Dyslipidemia2,4281,261 (52)999 (51)262 (58)0.003Diabetes mellitus2,4571,084 (44)832 (41)252 (56)<0.001Hemodialysis2,417101 (4.2)53 (2.7)48 (11)<0.001Systolic blood pressure, mm Hg2,54593 (76-114)92 (75-112)98 (80-121)<0.001Heart rate, beats/min2,54590 (73-110)90 (73-110)90 (75-109)0.970Lactate, mmol/ L1,8764.2 (2.3-8.1)4.4 (2.4-8.2)3.6 (1.8-7.5)<0.001LVEF, %1,28930 (20-40)30 (20-40)30 (20-42)0.238OHCA2,531368 (15)325 (16)43 (9.4)<0.001Revascularization PCI2,5452,302 (90)1,904 (91)398 (86)<0.001 CABG2,545239 (9.4)158 (7.6)81 (18)<0.001mAFP device2,5450.700 Impella 2.587 (3.4)70 (3.4)17 (3.7) Impella CP2,380 (94)1,952 (94)428 (93) Impella 5.060 (2.4)46 (2.2)14 (3.0) Impella 5.518 (0.7)15 (0.7)3 (0.6)Duration of mAFP, day2,5423.6 (1.7-6.7)3.7 (1.8-6.7)3.0 (1.0-6.3)0.004Door-to-unload time, min2,506137 (77-396)122 (74-308)247 (115-1,297)<0.001mAFP before PCI1,5271,226 (80)997 (80)229 (83)0.169Successful weaning2,5451,680 (66)1,360 (65)320 (69)0.103ECPELLA2,545919 (36)772 (37)147 (32)0.034Values are median (Q1-Q3) or n (%). A 2-sided P value of <0.05 indicated statistical significance. N represents the total number of valid data available for the entire population.CABG = coronary artery bypass graft; ECPELLA = simultaneous use of mAFP and extracorporeal membrane oxygenation; LVEF = left ventricular ejection fraction; mAFP = microaxial flow pump; NSTE-ACS = non–ST-segment elevation acute coronary syndrome; OHCA = out-of-hospital cardiac arrest; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction.Figure 130-Day Survival and In-Hospital Complications by ACS Type(A) Cumulative incidence of 30-day all-cause mortality. Thirty-day mortality was significantly higher in ST-segment elevation myocardial infarction (STEMI) patients than in those with non–ST-segment elevation acute coronary syndrome (NSTE-ACS) (32% vs 26%; HR: 1.46; 95% CI: 1.17-1.81; P < 0.001). (B) Thirty-day mortality stratified by quartiles of door-to-unload time. A shorter door-to-unload time was associated with improved survival, irrespective of ACS type. (C) In-hospital complications. Sepsis occurred more frequently in NSTE-ACS patients, whereas the incidence of other complications did not differ significantly between groups. mAFP = microaxial flow pump.
Discussion
This nationwide registry analysis revealed that 30-day mortality was significantly higher in the STEMI group, and a shorter door-to-unload time was associated with improved survival. This time-mortality association remained significant in multivariable analysis for STEMI, but not for NSTE-ACS, likely due to the smaller sample size and different pathophysiological dynamics in the latter. These results suggest that early mAFP support is particularly critical in STEMI-related CS, and that prognostic factors may differ by ACS subtype.
The higher 30-day mortality in STEMI patients, despite more favorable risk profiles and shorter door-to-unload times, likely reflects the distinct pathophysiology of STEMI-related CS. In STEMI, acute coronary artery occlusion or critical flow limitation often causes rapid and extensive myocardial ischemia, leading to larger infarct size and more severe metabolic derangements.6^,^10 In our cohort, STEMI patients exhibited significantly higher lactate levels at presentation, suggesting profound tissue hypoperfusion and systemic stress. Even with timely revascularization and mechanical circulatory support, irreversible myocardial injury and inflammatory responses may precipitate multiorgan dysfunction in STEMI. Furthermore, STEMI may involve mechanical complications (eg, ventricular septal rupture), which further worsen outcomes.10 By contrast, NSTE-ACS is commonly associated with subtotal occlusion or fluctuating ischemia, allowing for more gradual hemodynamic deterioration and better tolerance of delayed support initiation. These differences in ischemic burden and shock dynamics likely contribute to the mortality gap between ACS subtypes.
This study has several limitations. This is a retrospective registry analysis, which is subject to selection bias and residual confounding. The lack of detailed procedural data, such as door-to-balloon time, use of rotational atherectomy, left main trunk bifurcation stenting, thrombosuction, and glycoprotein IIb/IIIa inhibitors, is an inherent limitation of the registry. Long-term outcomes and data on infarct-related artery or left ventricular ejection fraction were unavailable. Results may be influenced by institutional differences in protocols and operator experience. Quartile distribution was skewed in NSTE-ACS, limiting interpretation of time-mortality association. Nonetheless, this study provides meaningful insights into the differential characteristics and time-sensitive nature of mAFP therapy across ACS subtypes, reinforcing the need for tailored management strategies in CS.
Financial Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1García-García C.Oliveras T.El Ouaddi N.Short- and long-term mortality trends in STEMI-cardiogenic shock over three decades (1989–2018): the Ruti-STEMI-Shock registry J Clin Med 98202023983272703410.3390/jcm 9082398 PMC 7465647 · doi ↗ · pubmed ↗
- 2Anderson M.L.Peterson E.D.Peng S.A.Differences in the profile, treatment, and prognosis of patients with cardiogenic shock by myocardial infarction classification: a report from NCDR Circ Cardiovasc Qual Outcomes 66201370871510.1161/CIRCOUTCOMES.113.00026224221834 · doi ↗ · pubmed ↗
- 3Amin A.P.Spertus J.A.Curtis J.P.The evolving landscape of Impella use in the United States among patients undergoing percutaneous coronary intervention with mechanical circulatory support Circulation 141420202732843173507810.1161/CIRCULATIONAHA.119.044007 · doi ↗ · pubmed ↗
- 4Møller J.E.Engstrøm T.Jensen L.O.Dan Ger Shock Investigators Microaxial flow pump or standard care in infarct-related cardiogenic shock N Engl J Med 390152024138213933858723910.1056/NEJ Moa 2312572 · doi ↗ · pubmed ↗
- 5Abbott J.D.Ahmed H.N.Vlachos H.A.Selzer F.Williams D.O.Comparison of outcome in patients with ST-elevation versus non-ST-elevation acute myocardial infarction treated with percutaneous coronary intervention (from the National Heart, Lung, and Blood Institute Dynamic Registry)Am J Cardiol 100220071901951763106810.1016/j.amjcard.2007.02.083 · doi ↗ · pubmed ↗
- 6Martínez M.J.Rueda F.Labata C.Non-STEMI vs. STEMI cardiogenic shock: clinical profile and long-term outcomes J Clin Med 11122022355810.3390/jcm 1112355835743628 PMC 9224589 · doi ↗ · pubmed ↗
- 7Taha H.S.Gohar A.Ammar W.Predictors of short-term mortality in cardiogenic shock: insights from an Egyptian multicenter registry Egypt Heart J 7612024943906087610.1186/s 43044-024-00525-y PMC 11282039 · doi ↗ · pubmed ↗
- 8Tsai M.L.Hsieh M.J.Chen C.C.Prognosis of patients with cardiogenic shock following acute myocardial infarction: the difference between ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction Medicine (Baltimore)101362022 e 3042610.1097/MD.0000000000030426 PMC 1098043836086759 · doi ↗ · pubmed ↗