Validity and reliability study of anatomy attitude scale in dental students
Kamber Kaşali̇, Didem Özkal Emi̇noğlu, Anvar Dadashov

TL;DR
This study adapts and validates a scale to measure dental students' attitudes toward anatomy, confirming its reliability and three-factor structure.
Contribution
The study modifies and validates the Anatomy Attitude Scale for dental students, confirming its three-factor structure and reliability.
Findings
The three-factor structure of the Anatomy Attitude Scale for Dental Students was confirmed.
The scale demonstrated acceptable reliability with Cronbach’s alpha of 0.588 and McDonald’s ω of 0.660.
Confirmatory factor analysis showed good fit indices (χ2/df = 2.492, RMSEA = 0.071, CFI = 0.922).
Abstract
The anatomy education contributes significantly to the cognitive and perceptive learning of students. The purpose of this study was to modify and assess the validity and reliability of the “Anatomy Attitude Scale for Medical School Students”, a tool used to assess medical students’ attitudes about anatomy, for use with dental students. The “Anatomy Attitude Scale for Dental Student (AASDS)” scale was tested on 297 students. Subsequently, the completed scale was administered to dental students in order to confirm its validity. Confirmatory factor analysis was used to evaluate construct validity. The reliability of the scale was assessed using test-retest, item correlations, split-half analysis, and Cronbach’s alpha coefficient. The statistical analysis was conducted using package programs. The accepted threshold for statistical significance was P < 0.05. The participants’ average age…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
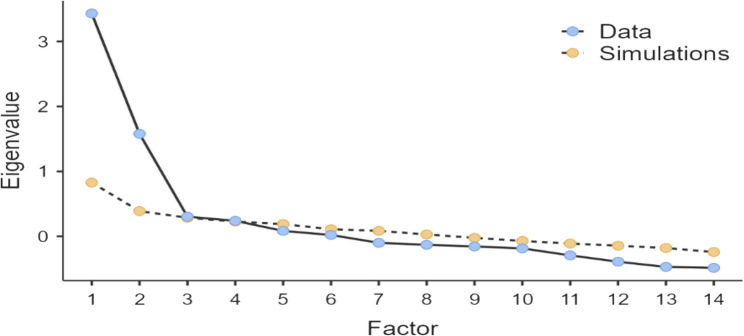 Figure 1
Figure 1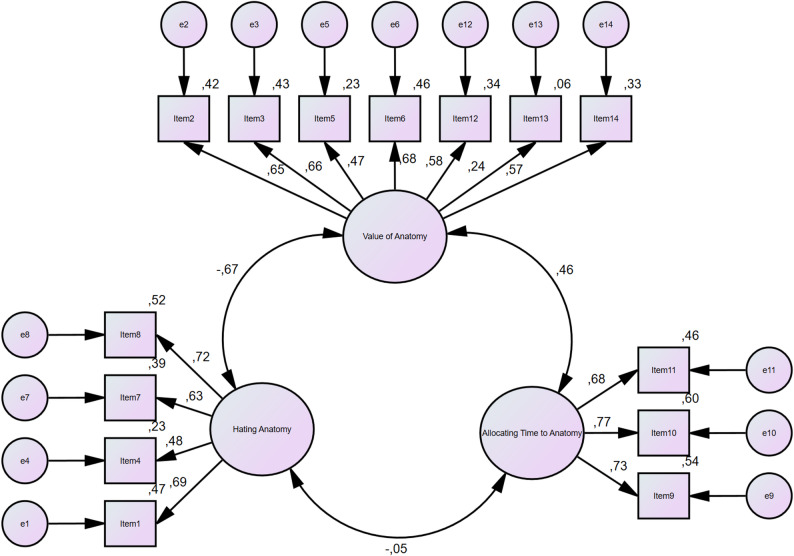 Figure 2
Figure 2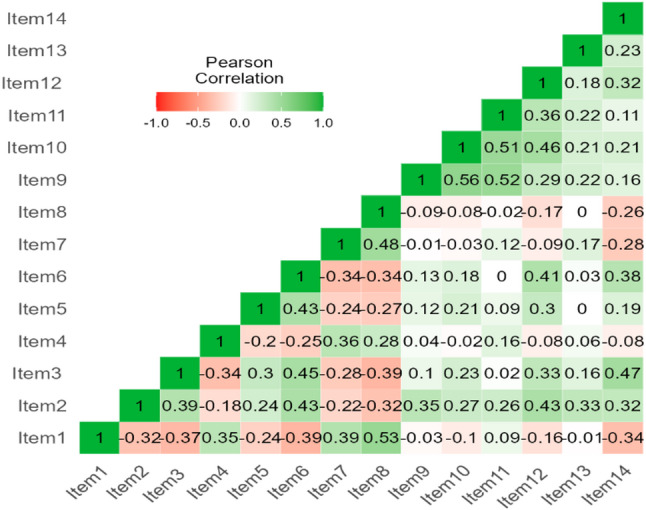 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnatomy and Medical Technology · Dental Anxiety and Anesthesia Techniques · Dental Research and COVID-19
Introduction
Anatomy is a fundamental medical study that investigates the organs constituting the human structure and form, the systems created by the integration of these organs, and their interrelationships [1, 2]. The teaching of anatomy contributes significantly to the cognitive and perceptive learning of students. In anatomy education, the integration of sensory experiences and psychomotor activities—such as visual-spatial recognition, model-based exploration, and dissection—enhances students’ cognitive engagement and learning outcomes [3]. Anatomy forms a fundamental component of dental education, providing the structural knowledge necessary for developing the fine motor skills and manual dexterity required in clinical dentistry [4–6]. The anatomy course establishes the foundation for the professional courses that students will undertake in subsequent years. For this reason, students should be very well trained in the subjects given in this course [7, 8]. Anatomy education is carried out in health-related institutions and colleges in the form of theoretical and practical course hours within the possibilities of the institutions. The aim of this course is to enable students studying in areas related to human health to learn the structure of the parts of the body and their relationships with each other. The contents of the courses are transferred to the students theoretically and supported by practice in practical courses. Cadavers, models, plastinated materials, anatomical modelling, radiological images, mobile augmented reality applications are used as practical course materials [4, 9–12]. The anatomy course, which starts to be taught in the first year of education, causes negative prejudices due to its intensive anatomical terminology. Anxiety manifests in students, adversely affecting their interest in the anatomy course and their ability to engage with subsequent coursework. Determining the views and attitudes of dental students about anatomy may be of great importance as a guide in preventing such possible negativities.
Attitude is an individual’s assessment of other persons, things, or ideas [13, 14]. Attitudes have three elements: the cognitive component, which includes ideas and beliefs about the object; the emotional component, which encompasses emotional reactions towards the object; and the behavioral component, which pertains to behaviors directed towards the object [15]. During the literature study, it was discovered that there is no “Anatomy Attitude Scale” that directly indicates the attitudes of dentistry school students toward anatomy and was established specifically for dental students. This condition justifies the creation of a measurement instrument that collects relevant and reliable data to evaluate dentistry students’ views regarding anatomy.
Anatomy education for dental and medical students is an extremely important for students in both fields. Although anatomy lessons are offered in both fields, there are some important differences in the content, scope, and evaluation methods. These differences arise because students in both fields may need different knowledge and skills. While anatomy education for medical students is aimed at evaluating the entire general anatomical formation of the body, anatomy education for dental students focuses more on head, neck, and tooth anatomy [16]. Anatomy education also constitutes the foundation upon which the motor and cognitive skills of dental students are built. Although manual dexterity and procedural skills are critical in dental training, these competencies depend on a solid understanding of the anatomical structures of the head and neck region. Detailed anatomical knowledge is essential for clinical practices such as local anesthesia, extractions, implant placement, endodontic access, and periodontal surgery, where even minor anatomical misinterpretations can cause complications including nerve or vascular injury. Therefore, anatomy serves as both the theoretical and practical basis for clinical dentistry. Understanding dental students’ attitudes toward anatomy can provide valuable feedback for improving educational strategies and ensuring safer, anatomy-based clinical performance [4–6].
The objective of this research is to adapt the “Anatomy Attitude Scale for Medical School Students,” which was established by Mehmet Ali Can in 2022 for students of the faculty of medicine, in a valid and reliable manner to show attitudes toward anatomy for dental students. In the light of the data to be obtained, new educational programmes can be developed to prevent students’ attitudes towards anatomy education, possible concerns and prejudices.
Materials and methods
Study design
The study is a two-stage observational validation study. In the first stage, Mehmet Alı Can was contacted via e-mail and the necessary permission was obtained for the adaptation of the scale for dentistry students [17]. Then, the necessary permission for the study was obtained from “Atatürk University Faculty of Dentistry Ethics Committee (No: 49, Date: 25/10/2023, Session number: 10/2023)”. The study followed the guidelines of the “Declaration of Helsinki”. Informed Consent obtained from all the participant.
Sample size
When type 1 error = 0.05, type 2 error = 0.20 (Power = 0.80) and Cronbach’s alpha is 80%, the minimum sample size required for our study is 180. Considering a 10% loss, this number has been set at 200.
Data collection tools
The data collecting instrument (survey) comprised sociodemographic questions such as age, gender, reasons for selecting the faculty of dentistry for dental students, and an anatomy attitude scale student questionnaire.
Anatomy attitude scale for medical school students
The scale is a 14-item self-assessment measure for evaluating medical students’ attitudes about anatomy [17]. The measure uses a 5-point Likert scale: strongly disagree (1), disagree (2), slightly agree (3), agree (4), and strongly agree (5). Scale objects are graded from 1 to 5 points. No items are scored in reverse. The scale includes three dimensions: (1) The importance of anatomy, (2) disliking anatomy, and (3) devoting time to anatomy. The total score received from the scale ranges from 14 to 70. Dimension ratings range from 7 to 35 points for the value of anatomy, 4 to 20 points for hating anatomy, and 3 to 15 points for allocating time to anatomy.
The procedures performed within the scope of adapting the scale to dentistry students
The “Anatomy Attitude Scale for Medical School Students” established for medical students was reviewed by two dentists, and only minor alterations were made to the questions for dentistry students. The “Anatomy Attitude Scale for Medical School Students” was first translated from English to Turkish, and then back to English. Then, the obtained form was reviewed by a language expert in terms of meaning and grammar. After the expert approval, the “Anatomy Attitude Scale for Dental Students” form was created for dental students and presented in Table 1.
Table 1. Dental students version of “Anatomy attitude scale for medical Students”ItemsFactorsItem1If I were the minister of health, I would abolish the anatomy course from dentistry faculties.*Item2Learning anatomy makes me happy.Item3I would not call a person who does not know anatomy a dentist.Item4If the most unnecessary courses are ranked, “anatomy” comes first.*Item5Anatomy information should be reminded at the beginning of each internship.Item6Recognising the human body with “anatomy” makes me feel like a dentist.Item7If I were in charge, I would remove anatomy information from the “Dentistry Speciality Examination”.*Item8If I were a dental education planner, I would recommend anatomy only as an elective course.Item9I would like to do a PhD in anatomy when I graduate.Item10Drawing anatomical figures makes me happy.Item11I watch anatomy videos in my free time.Item12Anatomy practical lessons are interesting.Item13I liked anatomy very much because of the lecturers.Item14Anatomy is the basis of other dentistry courses. Items written have negative meanings and scored reversely
A pilot study involving 25 dentistry students was carried out prior to data collection. The dental students who participated in the pilot study were selected from all years (1st, 2nd, 3rd, 4th, and 5th years). It was determined whether the students who participated in the pilot study understood the questions correctly. Then the actual data collection process started and the results of the students who participated in the pilot study were not included in the actual study.
Three hundred students were invited to the study. The study sample consisted of dental students enrolled in all academic years (1st to 5th year) at the Faculty of Dentistry, Atatürk University. The dental students who answered the questionnaire were asked to answer the same questionnaire again after 3 months.
Statistical analyses
The scale’s validity and reliability were examined using the statistical packages JAMOVI 2.2.2, AMOS v20.0 (Analysis of a Moment Structure), and SPSS v20.0 (Statistical Package for Social Sciences). Descriptive statistics are provided for the demographic data. The sociodemographic features were displayed as percentages or as mean ± standard deviation (SD). Scores on a scale are displayed as mean ± SD. Data analysis was performed using the Pearson correlation coefficient to examine the relationships among the sub-dimensions of the scale. The normality of each sub- dimension was assessed using the Shapiro–Wilk and Kolmogorov–Smirnov tests, and all sub-dimensions were found to be normally distributed. Therefore, the assumptions for applying the Pearson correlation were satisfied. The Cronbach’s alpha coefficient, McDonald’s omega, split half, correlation between forms, Guttman split-half coefficient, and Hotelling’s T-squared findings are provided for the scale’s internal consistency. Kaiser-Meyer-Olkin (KMO), Bartlett sphericity tests, Scree plots, and correlation matrices were employed to assess the construct validity of the scale. Furthermore, the correlation between the test and test-retest results was provided. Confirmatory factor analysis was employed to analyze the scale’s fit results. Fit indexes included the Tucker-Lewis index (TLI), Chi-square statistic (χ2), Chi-square degree of freedom ratio (CMIN/DF), root mean square error of approximation (RMSEA), standardised root mean square (SRMR), and comparative fit index (CFI). With a path diagram, the confirmatory factor analysis model is displayed. A p-value of less than 0.05 was deemed significant.
Results
The study included 292 of the 300 students accepted from dental schools (years 1–5). The response rate was 97%.
Characteristics of participants
The participants’ average age was 23 ± 2.73 years (18–28), with 63.4% being female. Table 2 shows the students’ sociodemographic characteristics.
Table 2. Sociodemographic characteristics of participantsSociodemographic characteristics N %GenderMale10736,6%Female18563,4%YearsYear 15017,1Year 24615,8Year 34716,1Year 47927,1Year 57024,0Why did you choose dentistry?Because my parents wanted me to.227,5%Because this is my ideal career.7626,0%Because it is a profession that makes money.4415,1%Because I have enough points.11037,7%Because it is good status in society4013,7%Do you want to be a dentist specialist in the future?Yes22577,1%No6722,9%Mean ± sdMed (Min-Max)Age23.22 ± 2.7324 (18–28)
Findings regarding the validity of the scale
Bartlett’s sphericity test and the Kaiser-Meyer-Olkin measure. The KMO value was 0.807, and Bartlett’s test of sphericity showed statistical significance (approx. = 1203.005, degrees of freedom (DF) = 91, P < 0.001). The dispersion point test revealed that the scale included three variables, and factors beyond the third were not explanatory (Fig. 1).
Fig. 1. Scree plot for factor analysis of the AASDS
Confirmatory factor analysis
The CFA model at the first level states, 7 items (items 2,3,5,6,12,13, and 14) are collected in the “Value of anatomy” subdomain, 4 items (items 1,4,7, and 8) in the “Hating anatomy” and 3 items (items 9, 10, and 11) in the “Allocating Time to Anatomy” subdomain (Table 3). Every item that makes up the model contributes in a statistically significant way (P < 0.05).
Table 3. Sub-dimensions of the “Anatomy attitude scale for dental student (AASDS)”ItemsFactorsMean ± SdFactor 1: Value of anatomy21,83 ± 5,38Item2Learning anatomy makes me happy.2,91 ± 1,23Item3I would not call a person who does not know anatomy a dentist.3,40 ± 1,22Item5Anatomy information should be reminded at the beginning of each internship.3,28 ± 1,18Item6Recognising the human body with “anatomy” makes me feel like a dentist.3,73 ± 1,08Item12Anatomy practical lessons are interesting.2,98 ± 1,24Item13I liked anatomy very much because of the lecturers.2,38 ± 1,31Item14Anatomy is the basis of other dentistry courses.3,16 ± 1,26Factor 2: Hating anatomy8,53 ± 3,68Item1If I were the minister of health, I would abolish the anatomy course from dentistry faculties.*1,96 ± 1,23Item4If the most unnecessary courses are ranked, “anatomy” comes first.*2,05 ± 1,28Item7If I were in charge, I would remove anatomy information from the “Dentistry Speciality Examination”.*2,23 ± 1,25Item8If I were a dental education planner, I would recommend anatomy only as an elective course.*2,28 ± 1,22Factor 3: Allocating Time to Anatomy6,44 ± 2,94Item9I would like to do a PhD in anatomy when I graduate.2,10 ± 1,14Item10Drawing anatomical figures makes me happy.2,27 ± 1,26Item11I watch anatomy videos in my free time.2,05 ± 1,15
Model fit of the scale
The first-level CFA model’s goodness-of-fit analysis supported the study’s original design (χ2/df = 2.492, RMSEA = 0.071, SRMR = 0,070, TLI = 0.900, CFI = 0.922). In our investigation, RMSEA, SRMR, TLI, and CFI all demonstrated an adequate fit. Table 4 shows the reference values for the goodness-of-fit analysis findings, as well as the most often used goodness-of-fit indices in the literature (Fig. 2).
Table 4. Anatomy attitude scale compliance indexes for dental studentsIndexes Reference ValueGood fitAcceptable fitMeasurementResultCMIN/DF0 < χ 2/Df ≤ 33 < χ 2/Df ≤ 52,492Good fitRMSEA0 ≤ RMSEA ≤ 0.050.05 < RMSEA ≤ 0.080.071 (0.057–0.084)Acceptable fitSRMR0 ≤ SRMR ≤ 0.050.05 < SRMR ≤ 0.100.070Acceptable fitTLI0.95 < TLI ≤ 10.90 < TLI ≤ 0.940.900Acceptable fitCFI0.95 < CFI ≤ 10.90 < CFI ≤ 0.940.922Acceptable fitCMIN/DF Chi-square degree of freedom ratio, RMSEA Root mean square error of approximation, SRMR Standardised root mean square, TLI Tucker-Lewis index, *CFI *Comparative fit index
Fig. 2. Path Diagram
Findings regarding the reliability of the scale
Cronbach’s alpha reliability coefficient was 0.588 for the entire scale and 0.745, 0.721, and 0.772 for the values of anatomy, hating anatomy, and allocating time to anatomy, respectively. Cronbach’s alpha values for the retest were 0.538 for the total scale and 0.728, 0.815, and 0.666 for the value of anatomy, hating anatomy, and allocating time to anatomy, respectively. The correlations between test and retest data were statistically significant (Table 5). In the factor, all items are strongly associated (Fig. 3). Cronbach’s alpha scores were 0.746 and 0.622 in the split-half study used to assess the scale’s reliability. Table 6 summarizes the split-half analysis findings. The scale is additive, according to the results of the analysis of variance, which was done to ascertain whether or not the scale items are additive (Nonadditivity: F = 1.875 P = 0.171 > 0.05). The measurement variation showed a significant difference (between measures, F = 74.430, P < 0.001). Using the Hotelling T2 test, it was determined whether the question means were equal. The results showed a significant difference in the averages (Hotelling’s T-squared = 454.763, F = 33.524, P < 0.001).
Table 5. The “Anatomy attitude scale for dental student (AASDS)” test and retest reliabilityMEANSDCronbach’s αMcDonald’s ωN of ItemsTestValue of anatomy3,1200,7690,7450,7587Hating anatomy2,1300,9220,7210,7274Allocating Time to Anatomy2,1500,9830,7720,7733Total2,6300,4850,5880,66014Re-TestValue of anatomy2,9700,8380,7280,7367Hating anatomy2,0200,9960,8150,8184Allocating Time to Anatomy1,8900,9640,6660,6933Total2,5200,4750,5380,65314TestValue of anatomyHating anatomyAllocating Time to AnatomyTotalRe-TestValue of anatomyr0,498−0,3040,2300,331p**< 0**,001< 0,001< 0,001< 0,001N268268269267Hating anatomyr−0,2370,4520,0080,071p< 0,001**< 0**,0010,8910,245N268268269267Allocating Time to Anatomyr0,321−0,0620,4440,421p< 0,0010,313**< 0**,001< 0,001N268268269267Totalr0,429−0,0180,3960,511p< 0,0010,771< 0,001**< 0**,001N268268269267r: Pearson Correlation, *p *statistical significance level
Fig. 3. Correlation matrix
Discussion
Although competence in dentistry arises from the integration of cognitive, psychomotor, and affective skills, anatomical knowledge forms the structural foundation upon which manual dexterity and clinical precision are built. Therefore, the Anatomy Attitude Scale for Dental Students (AASDS) evaluates attitudes toward this cognitive component, which indirectly supports psychomotor learning and overall professional development [4–6].
Anatomicy has a profound and antiquated connection to the history of dentistry and medicine. Both fields need understanding of the human body’s structure and functioning. However, there are also significant differences in anatomy teaching and emphasis between the two areas. Within the medical industry, anatomy is commonly seen as a comprehensive discipline that spans the entirety of the human body and is closely connected to clinical practice. Dental medicine was characterized as an integrated, yet distinct and autonomous, medical specialty, in part due to the historical contribution of anatomy to its development. The characterization of the maxillary sinus, salivary glands, tongue and lip muscles, and the microscopic anatomy of dental hard tissues form the foundation of anatomy education in the field of dentistry [5, 6].
The study of anatomy is approached differently by students of dentistry and medicine. The two fields’ approaches to teaching anatomy reflect these distinctions. Anatomy instruction and the application of this knowledge in future professions are advantageous for students in both disciplines [6].
The Anatomy Attitude Scale for Dental Students (AASDS) provides valuable insight into students’ perceptions and attitudes toward anatomy. Such understanding enables educators to recognize areas where students may feel less confident, disengaged, or anxious about anatomy learning. By identifying these areas, curriculum planners and instructors can design targeted educational interventions to enhance motivation and participation in anatomy-related activities. Moreover, understanding students’ attitudes through the AASDS not only benefits anatomy teaching itself but also indirectly contributes to the development of the manual dexterity and psychomotor competencies that are essential for professional dental practice. Overall, this emphasizes the importance of attitude assessment as a pedagogical tool that can guide curriculum development, improve teaching strategies, and ultimately support both cognitive and practical skill acquisition in dental education [4–6].
Study strengths and limitations
The study’s strength is that it gives researchers with a technique that has been demonstrated to be valid and reliable, as well as results that are comparable internationally. Furthermore, the AASDS is a brief scale that may be used to assess dental students’ attitudes about anatomy. In addition, the findings of this study may contribute to more effective use of time and resources allocated to anatomy in dental education. It can also be used to develop interventions to improve attitudes towards anatomy. However, the following limitations should also be recognised. The AASDS was designed to measure only attitudes towards anatomy. Different scales may need to be used to measure dental students’ knowledge of anatomy or their satisfaction with anatomy courses. During the study, no external factors that may affect students’ attitudes towards anatomy were considered.
Conclusions
The Anatomy Attitude Scale for dental students has been proven to be a viable and effective tool for measuring their attitudes toward anatomy. The 14-item, three-factor scale’s original structure was maintained throughout the validation process. Thus, the scale may be used as a tool to assess dental students’ ideas on anatomy. Note that the Anatomy Attitude Scale’s validity and reliability for dentistry students can change based on the demographic being examined and the context in which the scale is applied.