Severely displaced rib fractures are independently associated with reduced pulmonary function at 3 months
Yu-Hao Wang, Szu-An Chen, Yu-San Tee, Ling-Wei Kuo, Chi-Tung Cheng, Sheng-Yu Chan, Shih-Ching Kang, Chi-Hsun Hsieh, Fausto Catena, Chien-An Liao

TL;DR
Severely displaced rib fractures are linked to worse lung function three months after injury, even in non-flail chest cases.
Contribution
Identifies displaced rib fractures as an independent risk factor for reduced pulmonary function in trauma patients.
Findings
Each additional displaced rib increases odds of FVC < 80% by 31% at 3 months post-trauma.
Effect is strongest in patients with non-flail chest injuries.
Three or more displaced fractures is the optimal cutoff for predicting impaired pulmonary function.
Abstract
Multiple rib fractures are common injuries resulting from blunt chest trauma. However, the effect of rib fracture displacement on pulmonary ventilation remains unclear. This study aimed to investigate the effect of severely displaced ribs on pulmonary ventilation function (PVF) 3 months post-trauma. This retrospective case–control study was conducted at Chang Gung Memorial Hospital. Patients with multiple rib fractures (≥ 3) who underwent chest computed tomography (CT) from January 2019 to September 2023 were included. Patient demographics, injury severity, and rib fracture morphology were assessed. Displaced rib fractures were defined as bicortical displacements observed on CT. PVF was measured using forced vital capacity (FVC) and forced expiratory volume in 1 s. Univariate and multivariate logistic and linear regression analyses were performed to determine whether displaced rib…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
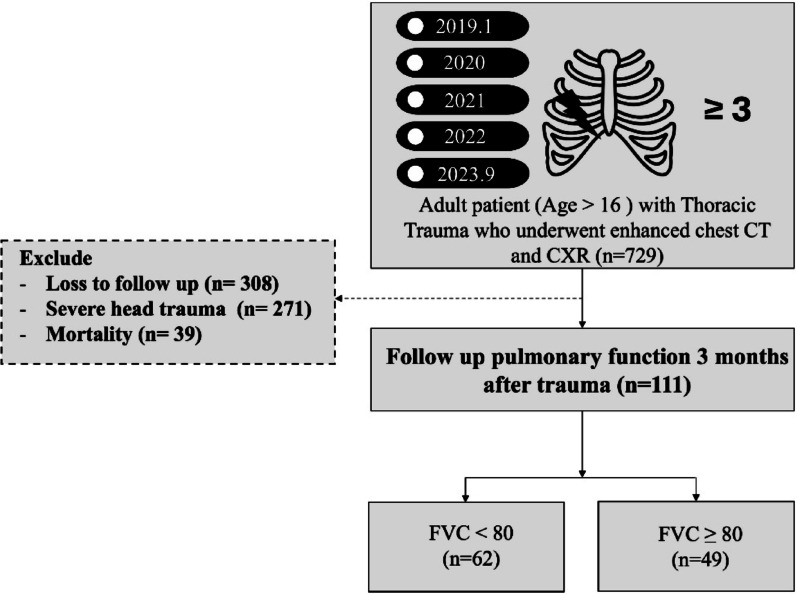 Figure 1
Figure 1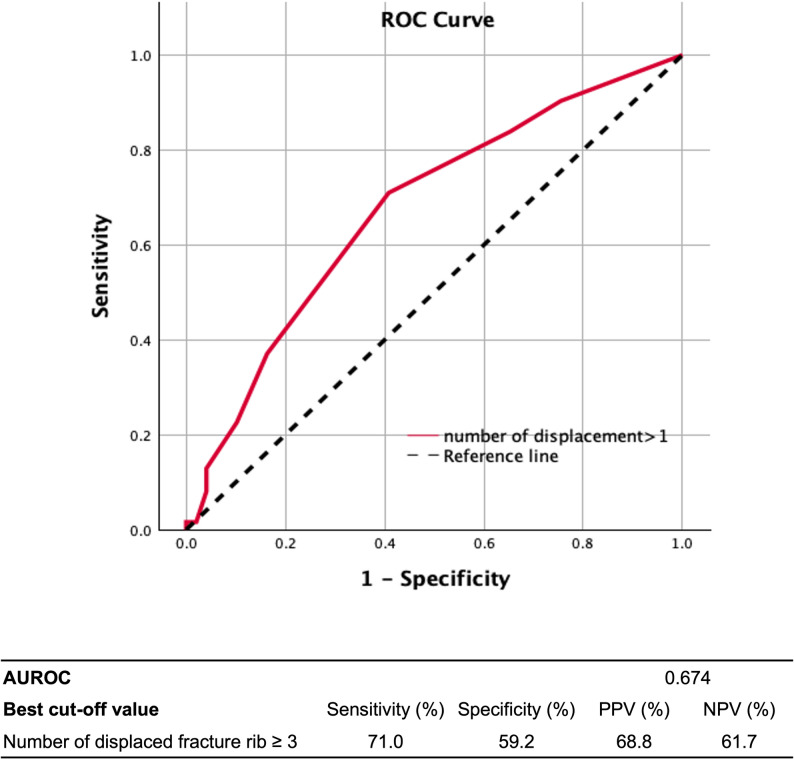 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Child Abuse and Related Trauma · Automotive and Human Injury Biomechanics
Introduction
Multiple rib fractures are the most common injuries resulting from blunt chest trauma, with incidence rates of 39–58% in patients with blunt chest trauma and 5–10% in those with all types of trauma [1–4]. Rib cage deformity decreases pulmonary ventilation function (PVF), increasing pulmonary complications and mortality rates, especially in patients with a flail chest—a chest wall deformity caused by fractures in three consecutive segmental ribs [5–9].
Surgical rib fixation has significantly increased over the years [10, 11]. Currently, the most robust evidence shows that surgical rib fixation is favorable for patients with flail chest. In these patients, surgical intervention reduces pain, decreases pulmonary complications, and shortens the duration of mechanical ventilator use [12]. Additionally, rib fixation in flail chest improved PVC within 3 months [13]. However, the indications for rib fixation in patients with a non-flail chest remain unclear. A prospective study suggested that severely displaced rib fractures are an indication of a non-flail chest [14]. Displacement severity is related pain intensity [15]. Therefore, although rib fixation may benefit these patients, supporting evidence is scarce. Furthermore, the effect of severely displaced rib fractures on respiration remains unclear. Therefore, we aimed to determine the impact of the number of severely displaced ribs on PVF at the 3-month follow-up.
Materials and methods
Study design and patient selection
This single-center, retrospective, case–control analysis was conducted at Chang Gung Memorial Hospital. The selected cohort comprised adult patients (age > 16 years) with multiple rib fractures (≥ 3) who underwent chest CT scans at our institution between January 2019 to September 2023. Patients with severe head trauma (head abbreviated injury scale (AIS) score ≥ 4), in-hospital mortality, or missing 3-month PVF data were excluded.
The collected data included demographic details, medical history (including chronic obstructive pulmonary disease (COPD) or asthma), other comorbidities, smoking history, trauma mechanism, injury severity (measured using the AIS), associated injuries. We defined lung contusion as a score of at least 4 points on the Blunt Pulmonary Contusion 18 (BPC18) scoring system, which includes the moderate (4–6 points) and severe (7–18 points) categories. Surgical rib fixation details (including interval and number of ribs fixed), severe hemothorax (defined as > 50% lung cavity in either plain film or CT, and pneumothorax were also recorded. Rib fracture score was calculated as the total number of rib fractures, multiplied by 2 if there are bilateral fractures, plus an age factor (51–60 = 1; 61–70 = 2; 71–80 = 3; > 80 = 4) to reflect general disease severity [16].
Morphology of rib fracture
The morphology of the rib fractures was assessed using chest CT scans, categorizing them as unilateral or bilateral. Flail chest was defined as the “radiographic flail,” which is the presence of three or more adjacent ribs fractured in two or more places, as confirmed by chest computed tomography (CT) scans. Fracture sites were classified as lateral, posterior, or combined. Severely displaced rib fractures were defined as exhibiting bicortical displacement, displacement, or ≥ 100% displacement.
Indication of rib fixation in our facility
In this cohort, surgical rib fixation was performed based on three specific indications:
- Flail Chest: This includes patients with a clinically evident flail chest or a radiologically confirmed flail chest.
- Severely Displaced Rib Fractures: This includes cases with severely displaced rib fractures, typically defined as having a displacement of more than one cortex.
- Other Associated Conditions: For patients without a flail chest or severely displaced fractures, surgery was indicated for impending or actual respiratory failure not attributable to lung contusion, inability to wean off of mechanical ventilation, or inadequate pain control.
Follow-up protocol and pulmonary function test
Patients underwent pulmonary function tests 3 months post-trauma. We employed a predictive equation to calculate the expected lung function based on patient age and height[17]. The ratios of the measured to predicted values were used as observational indices for subsequent statistical analyses. PVF measurements included Forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV_1_). All measurements were routinely performed by a respiratory specialist, using a portable pulmonary function detector. Each index was measured three times, and the mean values were used for the ratio calculations.
Statistical analysis
SPSS 29.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Descriptive statistics are expressed as numbers and percentages for categorical variables and as means, standard deviations, minima, and maxima for numerical variables. For comparisons between the two groups, an independent t-test was used for numerical variables, Pearson’s chi-square test for large-sample-sized categorical variables, and Fisher’s exact test for small-sample-sized categorical variables. Univariate and multivariate logistic regression analyses were conducted, with “low forced vital capacity (< 80%)” used as the dependent variable to determine the risk factors for deteriorating pulmonary function. The receiver operating characteristic (ROC) curve and Youden index were used to determine the best cutoff value for the number of displaced rib fractures affecting pulmonary vital capacity. A p value < 0.05 was considered significant.
Results
Overall, 729 eligible patients were identified. Figure 1 shows the patient selection flowchart**.** Ultimately, 111 patients were included; their key demographic and clinical details are reported in Table 1. Among the 73 patients who underwent rib fixation, 67 (91.7%) had severely displaced rib fractures, and 38 (52.1%) had a flail chest. Only six (8.2%) patients underwent rib fixation for other reasons, such as respiratory failure or uncontrolled pain, without having either a flail chest or a severely displaced fracture. Patients were divided into two groups based on their FVC at the 3-month follow-up: the FVC ≥ 80% group (n = 49) and the FVC < 80% group (n = 62) (Table 2). Patients with an FVC of < 80% had significantly higher Rib Fracture score (mean 8.4 vs. 11.2, p value: 0.026) and more rib fractures than did those with an FVC of ≥ 80% (p = 0.033). The number of severely displaced rib fractures was also significantly higher in the FVC < 80% group than in the FVC ≥ 80% group (p = 0.003). Bilateral rib fractures were more common in the FVC < 80% group than in the FVC ≥ 80% group (p = 0.043). Flail chest was observed in 48.4% of patients with an FVC of < 80% and in 32.7% of patients with an FVC of ≥ 80%, although this difference was not significant (p = 0.095). No significant differences were observed in age, sex, smoking status, presence of COPD or asthma, associated injuries, injury severity score (ISS), or lung contusions between the two groups. While the rib fixation rate was similar between the two groups, time from injury to rib fixation was significantly longer in the FVC < 80% group (4.6 ± 2.2) compared with the FVC ≥ 80% group (3.8 ± 1.5) (p = 0.044).Fig. 1. Flowchart of the patient selection protocol of the present study. This flow diagram illustrates the study process and outcomes in a cohort of patients with thoracic trauma who underwent enhanced chest CT and CXR between January 2019 and September 2023. The number of patients initially evaluated is 729. Patients lost to follow-up (n = 308), those with severe head trauma (n = 271), or those who died (n = 39) were excluded. The remaining 111 patients underwent follow-up pulmonary function testing 3 months post-trauma. These patients were categorized based on their forced vital capacity (FVC) values: 62 patients had FVC < 80, and 49 patients had FVC ≥ 80Table 1Characteristics of the study cohort (n = 111)Variablen (%), Mean ± SD (min–Max)Sex (male/female)75 (67.6%)/36 (32.4%)Age57.3 ± 14.2 (17 − 87)Smoking28 (25.2%)COPD^a^ or asthma3 (2.7%)Mechanism Motorcycle collision75 (67.6%) Fall22 (19.8%) Motor vehicle collision6 (5.4%) Pedestrian3 (2.7%) Bicycle3 (2.7%) Other2 (1.8%)Associated injury Head AIS^b^ ≥ 39 (8.1%) Chest AIS^b^ 4105 (94.6%) 56 (5.4%) Abdominal AIS^b^ ≥ 35 (4.5%) ISS^c^21.3 ± 5.4 (16–41) Rib fracture score9.95 ± 6.4 (4–44) Lung contusion88 (79.3%) Pneumothorax51 (45.9%) Severe hemothorax^d^6 (5.4%)Rib fracture morphology Patients with bilateral ribs fracture15 (13.5%) Patients with flail chest46 (41.4%) Number of fractured ribs7.1 ± 2.7 (3–22) Patients with severely displaced fractures93 (83.8%) Number of severely displaced fractures3.2 ± 2.5 (0–14) Fracture site Lateral19 (17.1%) Posterior16 (14.4%) Combined76 (68.5%)Patients with rib fixation73 (65.8%) Number of ribs surgically fixed3.9 ± 1.2 (2–7) Length of hospital stay11.2 ± 6.0 (2–36) Length of ICU stay2.7 ± 3.9 (0–18)Pulmonary function test (3 months post-trauma) FVC^e^77.2 ± 20.2 (40–125) FEV_1_^f^77.8 ± 19.7 (25–133)^a^Chronic obstructive lung disease^b^Abbreviated injury scale^c^Injury severity score^d^Hemothorax more than half of lung volume^e^Forced vital capacity f. Forced expiratory volume in 1 sTable 2Comparison of patients with FVC^e^ ≥ 80% and FVC^e^ < 80% 3 months post traumaFVC^e^ ≥ 80% (n = 49)FVC^e^ < 80% (n = 62)p valueSex (male/female)32 (65.3%)/17 (34.7%)43 (69.4%)/19 (30.6%)0.687Age55.8 ± 14.2 (17–84)58.5 ± 14.3 (26–87)0.322Smoking11 (22.4%)17 (27.4%)0.661COPD^a^ or asthma0 (0.0%)3 (4.8%)0.254Head AIS^b^ ≥ 36 (12.2%)3 (4.8%)0.180Chest AIS^b^0.692 447 (95.9%)58 (93.5%) 52 (4.1%)4 (6.5%)Abdominal AIS^b^ ≥ 32 (4.1%)3 (4.8%)1.000ISS^c^21.0 ± 5.4 (16–36)21.6 ± 5.4 (16–41)0.597Rib Fracture Score8.4 ± 4.4 (4–26)11.2 ± 7.5 (4–44)0.026Lung contusion35 (71.4%)53 (85.5%)0.070Pneumothorax20 (40.8%)31 (50.0%)0.335Severe hemothorax^d^4 (8.2%)2 (3.2%)0.403Rib fracture pattern Patients with bilateral ribs fracture3 (6.1%)12 (19.4%)0.043 Patients with flail chest16 (32.7%)30 (48.4%)0.095 Number of fractured ribs6.5 ± 2.1 (4–13)7.6 ± 3.0 (3–22)0.033 Patients with severely displaced fractures37 (75.5%)56 (90.3%)0.360 Number of severely displaced fractures2.4 ± 2.2 (0–9)3.8 ± 2.6 (0–14)0.003 Fracture site0.068 Lateral12 (24.5%)7 (11.3%) Posterior9 (18.4%)7 (11.3%) Combined28 (57.1%)48 (77.4%) Patients with rib fixation44 (71.0%)29 (59.2%)0.194 Number of ribs surgically fixed3.9 ± 1.2 (2–7)3.9 ± 1.1 (2–6)0.906^a^Chronic obstructive lung disease^b^Abbreviated injury scale^c^Injury severity score^d^Hemothorax more than half of lung volume^e^Forced vital capacity^f^Forced expiratory volume in 1 s
Univariate and multivariate logistic regression analyses were conducted to identify factors influencing lung function 3 months post-trauma (Table 3). In the univariate analysis, several factors were associated with FVC of less than 80%. Flail chest and bilateral rib fracture demonstrated odds ratios (ORs) of 1.93 (95% confidence interval (CI): 0.89–4.21, p = 0.096) and 3.68 (95% CI 0.98–13.87, p = 0.054), indicating a significant difference. The number of rib fractures and fracture sites classified as combined were significantly associated with lower FVC (OR: 1.20, 95% CI 1.01–1.43, p = 0.039 and OR: 2.57, 95% CI 1.13–5.85, p = 0.024, respectively). Notably, severe displacement showed a significant impact (OR: 3.03, 95% CI 1.04–8.78, p = 0.041). The number of severely displaced fractured ribs also differed significantly between the groups. Each additional severely displaced rib fracture increased the odds of a patient having FVC < 80% at 3 months post-trauma by 31% (OR: 1.31, 95% CI 1.09–1.57, p = 0.004).Table 3. Logistic regression analysis of factors affecting lung function (FVC < 80%) 3 months post-traumaUnivariate logistic regressionMultivariate logistic regressionOdds Ratio (95% CI)p valueOdds Ratio (95% CI)p valueSex (male/ female)1.20 (0.54 to 2.67)0.651Age1.01 (1.00 to 1.04)0.319Head AIS^a^0.74 (0.47 to 1.17)0.193Chest AIS^a^1.62 (0.28 to 9.24)0.587Abdominal AIS^a^1.11 (0.72 to 1.71)0.649Smoking1.31 (0.55 to 3.12)0.550Lung contusion2.36 (0.92 to 6.03)0.0741.00 (0.30 to 3.30)0.993Pneumothorax1.45 (0.68 to 3.09)0.336Severe hemothorax^b^0.38 (0.07 to 2.14)0.269Patients with flail chest1.93 (0.89 to 4.21)0.0960.73 (0.25 to 2.19)0.577Patients with bilateral ribs fracture3.68 (0.98 to 13.87)0.0542.53 (0.48 to 13.27)0.274Number of fractured ribs1.20 (1.01 to 1.43)0.0391.01 (0.78 to 1,30)0.945Fracture site Lateral0.39 (0.14 to 1.09)0.073 Posterior0.57 (0.19 to 1.65)0.296 Combined2.57 (1.13 to 5.85)0.0240.73 (0.25 to 2.19)0.297Patients with severely displaced fractures3.03 (1.04 to 8.78)0.041Number of severely displaced fractures1.31 (1.09 to 1.57)0.0041.27 (1.02 to 1.58)0.032Patients with rib fixation1.69 (0.77 to 3.72)0.195Number of ribs surgically fixed0.98 (0.65 to 1.47)0.904^a^Abbreviated injury scale^b^Hemothorax more than half of lung volume
In the multivariate analysis, the number of severely displaced ribs remained a significant risk factor for decreasing PVF (adjusted OR: 1.27, 95% CI 1.02–1.58, p = 0.032). Other factors including sex; age; AIS scores for head, chest, and abdominal injuries; rib fixation; and smoking were not considered significant risk factors for decreasing PVF 3 months post trauma in the multivariate analysis.
The subgroup analysis revealed different factors affecting lung function in patients with and without flail chest (Table 4). Among patients without flail chest (n = 65), those with FVC < 80% had a significantly higher Rib Fracture Score (mean: 9.3 v.s. 6.8, p = 0.021), and higher incidence of bilateral rib fractures (15.6% vs. 0%, p = 0.024). They also had more rib fractures on average (6.6 ± 2.3 vs. 5.6 ± 1.4, p = 0.026) and more severely displaced fractures (2.9 ± 2.0 vs. 1.6 ± 1.6, p = 0.002). However, in patients with flail chest (n = 46), there were no significant differences between the FVC < 80% and FVC ≥ 80% groups in terms of Rib fracture Score, bilateral rib fractures, number of rib fractures, number of severely displaced fractures, rib fixation rates, or lung contusion rates. We further performed univariate and multivariate linear regression analyses in patients without flail chest and found that the number of severely displaced fractures severely affected pulmonary function 3 months post-trauma in both univariate and multivariate analyses (Table 5).Table 4. Factors affecting lung function 3 months post-trauma in patients with and without flail chestFVC ≥ 80%FVC < 80%p valuePatient without flail chest (n = 65)(n = 33)(n = 32)Rib Fracture Score6.8 ± 1.9 (4–12)9.3 ± 5.5 (4–30)0.021Patients with bilateral ribs fracture0 (0.0%)5 (15.6%)0.024Fracture site Combined12 (36.4%)18 (56.3%)0.108Number of fractured ribs5.6 ± 1.4 (4–8)6.6 ± 2.3 (3–14)0.026Patients with severely displaced fractures21 (63.6%)27 (84.4%)0.057Number of severely displaced fractures1.6 ± 1.6 (0–6)2.9 ± 2.0 (0–6)0.002Patients with rib fixation16 (48.5%)19 (59.4%)0.379Lung contusion20 (60.6%)20 (62.5%)0.126Patient with flail chest (n = 46)(n = 16)(n = 30)Rib Fracture Score11.6 ± 6.0 (6–26)13.2 ± 8.8 (6–44)0.532Patients with bilateral ribs fracture3 (18.8%)7 (23.3%)1.000Fracture site Combined16 (100.0%)30 (100.0%)1.000Number of fractured ribs8.2 ± 2.2 (4–13)8.7 ± 3.4 (5–22)0.305Patients with severely displaced fractures16 (100.0%)29 (96.7%)1.000Number of severely displaced fractures4.2 ± 2.2 (2–9)4.8 ± 2.8 (0–14)0.214Patients with rib fixation13 (81.3%)25 (83.3%)1.000Lung contusion15 (93.8%)28 (93.3%)1.000Table 5Subgroup analysis of factors affecting FVC (%) 3 months post-trauma in patients without flail chest (n = 65)Univariate linear regressionp valueMultivariate linear regressionp valueB (95% CI)B (95% CI)Patients with bilateral ribs fracture − 17.18 (− 35.87 to 1.50)0.071 − 5.62 (− 26.54 to 15.30)0.593Number of fractured ribs − 2.73 (− 5.31 to − 0.15)0.038 − 1.36 (− 4.36 to 1.63)0.366Fracture site: combined − 10.21 (− 20.13 to − 0.28)0.044 − 5.96 (− 16.88 to 4.97)0.280Number of severely displaced fractures − 3.81 (− 6.36 to − 1.25)0.004 − 3.03 (− 5.80 to − 0.25)0.033Patients with rib fixation − 6.70 (− 16.81 to 3.42)0.191Number of ribs surgically fixed1.51 (− 6.99 to 10.01)0.720Lung contusion − 13.13 (− 23.69 to − 2.56)0.016 − 2.37 (− 15.40 to 10.66)0.717Pneumothorax − 0.95 (− 11.45 to 9.56)0.858Severely hemothorax^a^ − 14.08 (− 55.45 to 27.29)0.499^^R-squared of the multivariate linear model 0.194; F: 2.792, Sig. 0.025^^FVC: Forced vital capacity^a^Hemothorax more than half of the lung volume
Another subgroup analysis was performed based on whether patients underwent rib fixation. In patients who underwent rib fixation, we compared those with FVC ≥ 80% and FVC < 80%. The only significant difference was the number of severely displaced fractures (mean 3.21 vs. 4.52, p = 0.025), which suggests that even after rib fixation, a higher number of severe displaced fractures is associated with a poor pulmonary function outcome. Furthermore, in this subgroup, patients with multiple severe displaced fractures (≥ 3) had a poorer 3-month post-trauma FVC (mean: 72.4% vs. 83.5%, p = 0.038) and a higher proportion of patients with FVC < 80% (69.1% vs. 33.3%, p = 0.016). On the other hand, in patients without rib fixation, there was no significant difference in the number of severely displaced fractures between those with FVC ≥ 80% and FVC < 80%. Likewise, there was no significant difference in pulmonary function outcomes between the groups with and without multiple severe displaced fractures (≥ 3) (Supplementary Tables 1 and 2).
To determine the optimal cutoff value for the number of severely displaced rib fractures affecting pulmonary function 3 months post-trauma, ROC curve analysis and Youden index were used. The analysis identified three or more severely displaced rib fractures as the optimal cutoff value with a sensitivity of 71.0%, specificity of 59.2%, positive predictive value of 68.8%, and negative predictive value of 61.7% (Fig. 2).Fig. 2. Number of severely displaced rib fractures and FVC < 80 at 3 months post-trauma—ROC curve analysis. The receiver operating characteristic (ROC) curve illustrates the diagnostic performance of the number of severely displaced rib fractures in predicting forced vital capacity (FVC) < 80 at 3 months post-trauma. The area under the ROC curve (AUROC) is 0.674, suggesting moderate discriminative ability. The best cutoff value identified for the number of displaced rib fractures is ≥ 3. At this threshold, the sensitivity is 71.0%, specificity is 59.2%, positive predictive value (PPV) is 68.8%, and negative predictive value (NPV) is 61.7%
Discussion
To our knowledge, this study is the first to investigate the correlation between displaced rib fractures and pulmonary function outcomes 3 months post-trauma. The definition of displaced rib fractures varies in the literature, with bicortical displacement being the most commonly cited [18]. Bugaev proposed a three-dimensional equation to evaluate the displacement; however, its complexity limited its practical application [19]. Previous studies have suggested that displaced rib fractures independently increase the risk of pneumonia and respiratory failure, and tracheostomy [15, 20–22]. However, no previous studies have specifically linked these fractures to long-term pulmonary function outcomes. Our study found that bicortical displacement in rib fractures significantly affected pulmonary function outcomes 3 months post-trauma.
Previous studies have investigated the correlation between displaced rib fractures and increased opioid use, which indicated more severe pain [15]. This pain may limit deep breathing capacity, leading to shallow breathing and atelectasis, which can further affect PVF. Another possible pathophysiological mechanism is that the increased displacement in rib fractures suggests higher impact energy, leading to increased tissue damage and inflammation. Although not previously demonstrated specifically in rib fractures, displaced fractures are a known risk factor for other bones’ nonunion [23–25]. These factors can predispose patients to a further compromised respiratory function.
Many medical facilities and clinical studies have considered significantly displaced rib fractures as indications for surgical rib fixation [26, 27]. Randomized multicenter trials have demonstrated that surgical fixation of non-flail chest rib fractures can significantly shorten hospital stay in intubated patients [28]. Pieracci et al. further observed a lower rate of intrapulmonary complications and reduced pain in patients with three or more displaced rib fractures who underwent surgical rib fixation [14]. However, our study did not find a significant difference in 3-month PVF outcomes between patients with and without surgical rib fixation. Selection bias occurred because patients with flail chest and severely displaced fractures underwent surgical rib fixation at our facility, indicating a higher severity of rib fractures in this group. Therefore, the efficacy of rib fixation for improving pulmonary ventilation remains unclear.
Subgroup analysis showed that, within the flail chest subgroup, no significant difference was found in displaced rib fractures between patients with and without pulmonary function impairment. This is largely due to the prevalence of displaced rib fractures in most patients with flail chest. However, a lower PVF tended to correlate with a higher number of displaced rib fractures, although this was not statistically significant. Conversely, in the non-flail chest subgroup, displaced rib fractures significantly affected PVF outcomes. This underscores the importance of displaced rib fractures as a crucial factor affecting PVF outcomes in patients with a non-flail chest, indirectly suggesting the potential benefits of surgical rib fixation in this subgroup.
When considering rib fixation, it's notable that even after surgery, patients with more severely displaced fractures had significantly worse pulmonary function. This highlights the importance of fracture severity. This may be due to more severe underlying damage and the fact that fixation often targets only the 3rd to 10th ribs, potentially missing other severe fractures. Conversely, in patients without rib fixation, there was no significant difference in pulmonary function. This could be due to a selection bias, as most patients with multiple severe fractures were likely referred for surgery. Additionally, while 60–70% of this group had displaced fractures, the average was only one or two, which may not be severe enough to significantly impact pulmonary function.
Our study had several limitations. First, the substantial loss to follow-up may have compromised the overall reliability of the results. Furthermore, the lack of long-term follow-up, such as at 6 months and 1 year, reduces the value of the findings. Second, we lacked pre-injury PVF data, which is a common challenge in trauma studies. Additionally, we lacked data on early postinjury pulmonary function, which would have provided a more comprehensive understanding of the immediate impact of rib fractures on pulmonary function. Furthermore, there was a lack of analysis regarding the quantity of hemothorax and pneumothorax, as well as the proportion of patients who used chest tubes. Third, we did not collect data on pain level or pulmonary complications, which are crucial factors in evaluating patient outcomes and treatment effectiveness. Finally, our study did not conclusively determine the efficacy of surgical rib fixation in the management of displaced rib fractures.
Conclusions
Severely displaced rib fractures significantly impair PVF 3 months post-trauma, particularly in patients with a non-flail chest. Each additional severely displaced rib increased the odds of a patient having FVC < 80% at 3 months post-trauma by 31% (OR = 1.31), with three or more displaced ribs constituting the critical threshold. Therefore, more attention should be given to assessing rib displacement degree when managing chest trauma. Further research is required to evaluate the potential benefits of surgical rib fixation in patients with a non-flail chest and severe rib displacement.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Easter A. Management of patients with multiple rib fractures. Am J Crit Care. 2001;10:320–7, quiz 8–9.11548565 · pubmed ↗