Nitric Oxide-Releasing Thixotropic Hydrogels as Antibacterial and Hemocompatible Catheter Locks
Wuwei Li, Loren Liebrecht, Surendra Poudel, Rebecca Goodhart, Sayaji More, Jade Montano, Derek Lust, Qingguo Xu, Martin Mangino, Xuewei Wang

TL;DR
This paper introduces a new gel-based catheter lock that prevents bacterial contamination and blood clots using nitric oxide.
Contribution
The first gel-based catheter lock is developed, combining thixotropic hydrogel with nitric oxide for antibacterial and hemocompatible properties.
Findings
The hydrogel provides a physical barrier to slow bacterial migration and reduce drug loss.
Nitric oxide released from the gel effectively prevents biofilm formation on catheter surfaces.
The gel demonstrates excellent hemocompatibility and reduces clot adhesion.
Abstract
Catheters are indispensable medical tools for accessing blood vessels, hollow organs, and body cavities to facilitate medication delivery and fluid drainage. However, they also serve as major entry points for bacterial contamination and trigger foreign body responses, necessitating locking strategies that are both bactericidal and biocompatible. This study introduces the first gel-based catheter lock, in contrast to conventional liquid locks. The gel is a poloxamer-based hydrogel formulated with 2-hydroxypropyl α-cyclodextrin (HP-αCD). HP-αCD forms supramolecular complexes with the poloxamer to enhance gelation and with the nitric oxide (NO) donor to modulate NO release kinetics. This thixotropic gel can be injected into the catheter lumen when the catheter is not in use and withdrawn when vascular access is needed. The gel matrix provides a physical barrier that slows bacterial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 1
1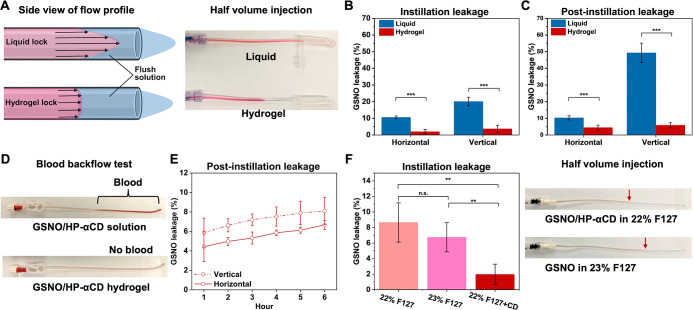 2
2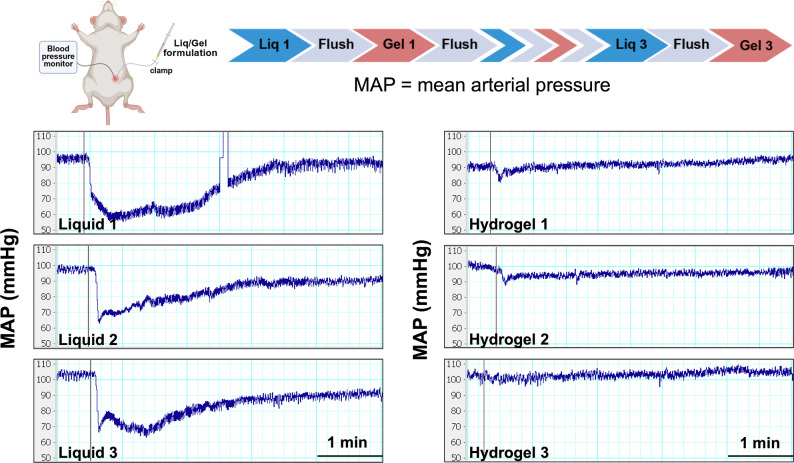 3
3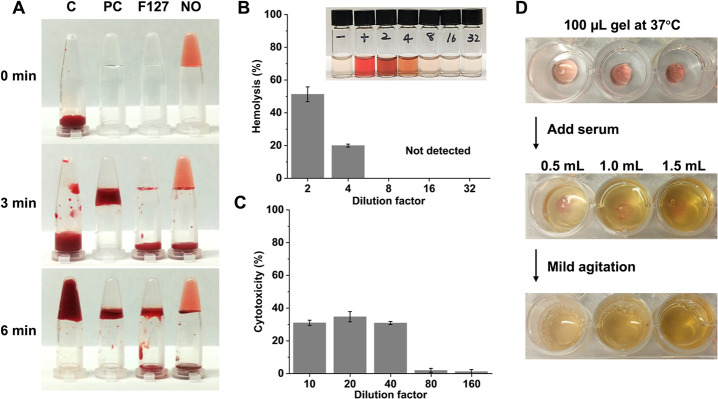 4
4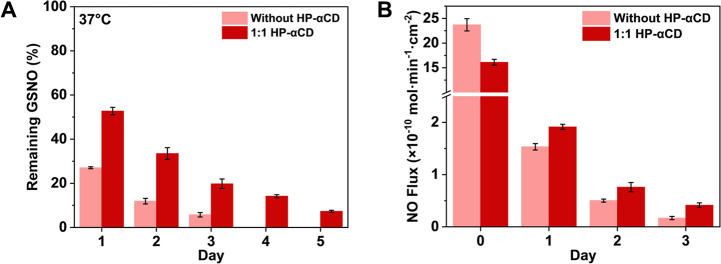 5
5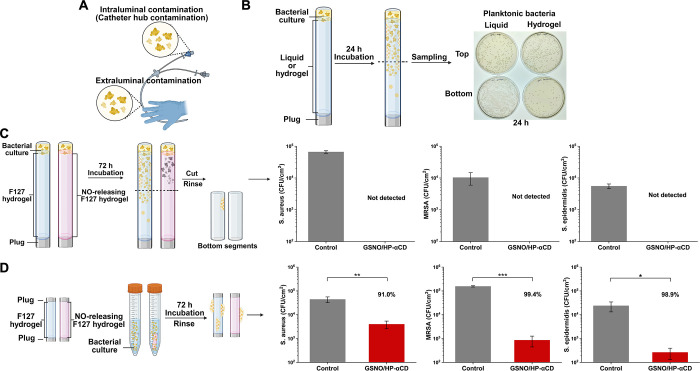 6
6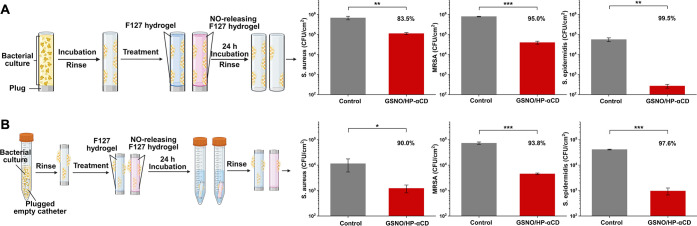 7
7- —National Heart, Lung, and Blood Institute10.13039/100000050
- —Virginia Commonwealth University10.13039/100009238
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHydrogels: synthesis, properties, applications · Polymer Surface Interaction Studies · Wound Healing and Treatments
Introduction
1
Central venous catheters (CVCs) are an essential component of modern medical care, routinely used for hemodialysis, chemotherapy, and parenteral nutrition.? While they provide immediate and reliable vascular access, CVCs are associated with two major complications: thrombus-related dysfunction and catheter-related bloodstream infections (CRBSIs).? In the context of hemodialysis, catheter dysfunction occurs at a rate of approximately 0.5 to 3.4 episodes per 1000 catheter-days, often necessitating catheter removal.? According to the Centers for Disease Control and Prevention (CDC) Surveillance Summary of Bloodstream Infections in Outpatient Hemodialysis Facilities (2014–2019), 63% (98,502 out of 156,805) of reported bloodstream infections occurred in patients with CVCs.? CRBSIs are a major contributor to hospitalization and mortality in this population and also impose a substantial financial burden, with estimated costs per episode ranging from 11,591.?
In response to the significant morbidity and healthcare burden associated with catheter occlusion and infection, catheter coating strategies have been developed to address these complications. Coatings such as pyrolytic carbon, albumin, elastin-like polypeptides, and heparin have shown promise in maintaining catheter patency, while antimicrobial coatings, such as chlorhexidine/silver sulfadiazine, minocycline/rifampin, and platinum/silver, have demonstrated efficacy in reducing infection risk. ?,? However, despite progress in both research and clinical translation, coating-based approaches face key limitations. First, a limited amount of drugs can be loaded into the thin coating. Second, the addition of surface coatings often leads to increased manufacturing costs, which may limit widespread clinical adoption. Third, coatings cannot be adjusted, replaced, or replenished during the course of treatment. Compared to catheter coatings, the catheter lock technique provides superior cost efficiency and functional adaptability, enabling the use of formulations that can be modified or replaced as needed.? When a CVC is not in use, its lumens are filled with lock solutions that are designed to maintain catheter patency.? Anticoagulants such as heparin, ethylenediaminetetraacetic acid (EDTA), and trisodium citrate are commonly used in lock solutions to prevent and treat catheter thrombosis.? In parallel, a wide range of antibiotics (e.g., vancomycin, gentamicin, ciprofloxacin) and antiseptics (e.g., alcohol, taurolidine, trisodium citrate) solutions have been employed for antimicrobial lock therapy. ?,?,? In clinical practice, it is common to combine anticoagulant and antimicrobial agents in a single lock formulation to address both major complications simultaneously. For example, in 2023, the U.S. Food and Drug Administration (FDA) approved DefenCath, a taurolidine-heparin (antiseptic + anticoagulant) lock solution, for the reduction of CRBSIs in adults with kidney failure undergoing chronic hemodialysis via CVCs.?
Although the catheter lock technique is a simple and practical approach to address both CVC-related complications, its broader application is limited by the unintended entry of lock solution into systemic circulation, even when the instilled volume does not exceed the priming volume of the catheter. ?−? ? ? Several studies have demonstrated that patients receiving heparin catheter locks after dialysis become systemically anticoagulated, with partial thromboplastin time values exceeding 200 s, far above the normal range of 25–35 s. ?,?,? The systematic anticoagulation leads to a higher risk of bleeding and heparin-induced thrombocytopenia. Similarly, in a study involving ethanol lock therapy, 8 out of 9 patients experienced systemic adverse effects, including transient light-headedness, euphoria, and nausea, indicating ethanol leakage into the bloodstream.? The leakage of lock solutions is primarily due to the absence of a physical barrier between the lock solution and contacting fluids. During instillation, a lock solution is injected to replace the pre-existing flush solution within the catheter lumen.? Due to the flow characteristics of Newtonian fluids, approximately 15–20% of the lock solution is immediately spilled into the bloodstream when the injection volume equals the lumen capacity. ?,? Following instillation, the lock solution continues to be progressively lost over time due to the absence of any physical boundary between the lock and circulating blood. ?,? Therefore, it is conceptually intuitive that introducing a physical interface between a lock and its contacting fluid could mitigate leakage caused by unrestricted mixing.
Hydrogels have been widely utilized in biomedical and pharmaceutical fields, such as drug delivery and tissue engineering, due to their high water content, tunable mechanical properties, permeability, and excellent biocompatibility. ?,? With advances in biomaterials, a growing number of injectable hydrogels have emerged and are being explored in applications such as bioengineered 3D printing and localized drug administration.? Given their semisolid nature, injectable hydrogels may fulfill the aforementioned need by serving as an alternative to traditional liquid lock solutions, forming a boundary between a lock and other fluids to minimize catheter lock leakage. However, to the best of our knowledge, no hydrogels have been reported for use as catheter locks.
Herein, we present a Pluronic F127-based injectable and withdrawable hydrogel designed as a viable alternative to traditional catheter lock solutions. In light of the dual clinical needs of CVCs, we select S-nitrosoglutathione (GSNO)/2-hydroxypropyl α-cyclodextrin (HP-αCD) complex as a model therapeutic agent and incorporated it into the hydrogel matrix. Given the potent antimicrobial and antithrombotic properties of nitric oxide (NO), ?−? ? ? ? various NO-releasing compounds, including GSNO, ?,? low-molecular-weight N-diazeniumdiolates,? S-nitroso*-N*-acetyl-penicillamine-conjugated ampicillin,? and S-nitroso-N-acetyl-L-cysteine ethyl ester,? have been previously added to lock solutions to mitigate the infectious and thrombotic complications of CVCs. However, all previous NO-releasing locks are based on solutions. In this work, we explore a new concept of hydrogel-based NO-releasing catheter locks with the aim of minimizing drug leakage and reducing systemic side effects. GSNO is selected as the NO donor in this work because it is an endogenous molecule naturally present in the human body, which minimizes safety concerns compared to synthetic NO-releasing agents.
Materials and Methods
2
Chemicals
and Reagents
2.1
Poloxamer 407 (Pluronic F127) was purchased from Spectrum Chemical Mfg. Corp. Sodium phosphate dibasic (Na_2_HPO_4_), sodium hydroxide (NaOH), l-glutathione reduced (GSH), sodium nitrite, sodium dodecyl sulfate (SDS), fetal bovine serum (FBS), and penicillin/streptomycin were purchased from MilliporeSigma. Luria–Bertani (LB) broth powder and agar were purchased from Thermo Fisher Scientific. HP-αCD was purchased from Cyclodextrin-Shop. Laponite-XLG (silicate nanoplatelet) is a gift from BYK USA lnc. Tryptic soy broth (TSB) was purchased from BD Biosciences. Eagle’s Minimum Essential Medium (EMEM), murine fibroblast L929 and bacterial strains, including Gram-positive strains: S. aureus (25923), methicillin-resistant S. aureus (MRSA, BAA-2312), and S. epidermidis (12228); Gram-negative strains: E. coli (53496), K. pneumoniae (BAA-1705), and P. aeruginosa (BAA-1744) were purchased from the American Type Culture Collection (ATCC).
Synthesis and Characterization of GSNO
2.2
GSNO was synthesized by nitrosating GSH in an acidic nitrite solution. In brief, 4.59 g (14.94 mmol) of GSH were dissolved in 29.87 mL of 0.5 M hydrochloric acid (14.94 mmol). The mixture was stirred at 0 °C for 10 min. Subsequently, 1.03 g (14.94 mmol) of sodium nitrite was added, and the reaction was stirred at the same temperature for 40 min, ensuring the flask was protected from light. Afterward, 10 mL of cold acetone was added to the mixture and stirred for an additional 10 min. The GSNO precipitate was collected through vacuum filtration and thoroughly washed with cold deionized water. Finally, the GSNO was freeze-dried and stored in the dark at −20 °C until further use. GSNO was characterized by ^1^H NMR (400 MHz, DMSO) and ^13^C NMR (100 MHz, DMSO) spectroscopy to confirm its structure; full spectra and peak assignments are provided in the Supporting Information (Figure S1).
Preparation of NO-Releasing Solutions and
Hydrogels
2.3
HP-αCD powder was weighed and dissolved in 0.1 M Na_2_HPO_4_ to make a 0.5 M HP-αCD stock solution. Then, 168.16 mg of GSNO was added to 1 mL of the HP-αCD stock, and NaOH was gradually introduced to adjust the pH to 7.4 and facilitate dissolution of GSNO. The Pluronic F127 stock solution (29 w/v%) was prepared using a standard cold method. Briefly, F127 powder was slowly added to 0.1 M cold phosphate buffer (pH = 7.4) under continuous stirring at 4 °C, and the mixture was stirred overnight until a clear, homogeneous solution was obtained. For the solution-based formulations, the GSNO/HP-αCD stock was diluted 5-fold with the phosphate buffer. For the hydrogel formulations, the GSNO/HP-αCD stock was blended with 29 w/v% F127 hydrogel in its liquid state and diluted with phosphate buffer in an ice bath to obtain the 0.1 M concentration of GSNO and HP-αCD, as well as different final concentrations of F127.
Rheological Measurements
2.4
The rheological tests were conducted using an Anton Paar MCR 702e rheometer equipped with a Peltier device for precise temperature control. A parallel plate geometry was used, featuring a 25 mm diameter upper plate and a fixed gap of 0.5 mm. A solvent trap was used throughout the experiments to prevent solvent loss by evaporation and preserve sample hydration. The shear viscosity (η) of the gels was measured under steady shear flow conditions across a range of shear rates (γ̇) from 0.01 to 1000 s^–1^. Amplitude sweep tests were conducted on gels maintained at 37 °C to identify the upper strain limit (γL) of the linear viscoelastic region and to determine the yield stress (σ_0_). Self-healing tests were performed using strain step oscillatory measurements at a fixed angular frequency (ω) of 10 rad/s. The strain amplitude was alternated every 300 s, starting with a small strain (1%) in the linear viscoelastic region, followed by a large strain (100%) within the nonlinear regime, and then returned to 1% to assess recovery. The elastic modulus (G′) and viscous modulus (G″) were recorded throughout to evaluate the energy stored and dissipated during each deformation cycle and to monitor structural recovery.
Evaluation of Leakages of Catheter Locks
2.5
To evaluate lock leakage under conditions mimicking clinical use, an in vitro catheter model was developed to mimic the essential features of a standard CVC, including a proximal connector compatible with a Luer-lock syringe, a flexible catheter body, a functional clamp, and an end-cap.
Leakage during Instillation
2.5.1
The catheter was prefilled with bubble-free saline and clamped to mimic a clinical catheter flush procedure. A Luer-lock syringe was filled with a solution or hydrogel formulation at a volume matching the internal volume of the catheter. The syringe with the hydrogel was warmed in a 37 °C incubator for 5 min to enable the gelation. The Luer-lock syringe was then connected to the connector of the catheter. The catheter was positioned either horizontally or vertically. After opening the clamp, the formulation was slowly and steadily infused into the catheter. The fluid flowing out of the distal end of the catheter was collected in a 1.5 mL microcentrifuge tube for subsequent quantification.
The percentage of GSNO leakage is defined as the ratio of the GSNO detected from the microcentrifuge tube to that infused into the catheter. The total infused GSNO was calculated from the known formulation concentration (0.1 M) and the injection volume of 0.22 mL. The leaked GSNO was quantified by measuring the absorbance of the collected fluid at 335 nm in a 96-well plate using a Varioskan LUX Multimode Microplate Reader. By multiplying the measured concentration by the collected volume in the microcentrifuge tube, the amount of leaked GSNO was obtained. Each formulation was tested with n = 5 replicates.
Leakage Postinstillation
2.5.2
The catheter was first locked with a solution or hydrogel. The clamp was closed and the proximal end of the catheter was capped. The catheter was then placed in a 37 °C incubator, either horizontally or vertically. The catheter tip was immersed in 1 mL of PBS solution in a tube that was sealed to prevent evaporation. At designated time points, the PBS was sampled to quantify the spilled GSNO via absorbance at 335 nm. The GSNO leakage was calculated as described above. Each formulation was tested with n = 3 replicates.
Blood Backflow Assays
2.5.3
The blood backflow assay followed the same procedure as described for the postinstillation leakage test, with the catheter tip immersed in 1 mL of rat blood containing 3.2% (w/v) sodium citrate instead of PBS. The catheters were hung vertically in the incubator.
In
Vivo Rat Experiment to Estimate the Lock Leakage
2.6
An adult male Sprague–Dawley rat (318 g, Envigo) was anesthetized via inhalation of isoflurane (1–2% in medical-grade oxygen) under spontaneous breathing. The anesthetic depth was adjusted to the minimal level necessary to abolish spinal and canthal reflexes. A polyethylene catheter (PE-50 tubing, BD Intramedic) was inserted into the femoral artery for continuous monitoring of hemodynamic variables, including mean arterial pressure (MAP), recorded via a disposable pressure transducer using a PowerLab data acquisition system (ADInstruments). Playback of the MAP data was used after the experiment for data analysis of blood pressure responses. A second PE catheter (Scientific Commodities, Inc., #BB31695-PE/5) was inserted into the femoral vein for testing of experimental catheter lock solution and gel formulations. After hemodynamic baseline values were observed, 0.1 mL of GSNO/HP-αCD-loaded lock solutions or gels was alternately placed into the venous catheter using a 1-mL syringe. After each lock solution/gel placement, the blood pressure response was recorded until a new stable baseline was reached. The catheter was flushed with a total of 0.5 mL of 5 units/mL heparin in Ringer's lactate solution before another solution or gel was tested. The rat was humanely euthanized with an anesthetic overdose at the end. The experiment was approved by the Virginia Commonwealth University (VCU) Institutional Animal Care and Use Committee (AD10003237).
Hemocompatibility and Cytotoxicity Tests
2.7
Blood Clotting Tests
2.7.1
Four groups (n = 3) of 1.5 mL microcentrifuge tubes were placed in a 37 °C dry bath. Tubes in the control group were filled with 0.4 mL of rat blood, and tubes of the other three groups were respectively filled with 0.4 mL of hydrogels: 6 w/v% silicate nanoplatelet hydrogel (served as positive control), 22 w/v% F127 hydrogel, and GSNO/HP-αCD-loaded F127 hydrogel. Then, 0.2 mL of rat blood was added to each tube. To restore coagulation activity in the sodium citrate (3.2 w/v%)-treated rat blood, 0.1 mL of 0.2 M CaCl_2_ was added to each mL of blood. The clot formation was monitored by leaning the tubes at 15-s intervals.
Surface Antifouling Tests
2.7.2
Sterile catheter tubes (2.5 cm, HelixMark 60-011-07) were divided into two groups and filled with 22 w/v% F127 hydrogels with or without GSNO/HP-αCD loading. Both ends of the tubes were sealed with sterile plastic rods. The sealed catheters were immersed in 3 mL of FBS in culture tubes and incubated at 37 °C with gentle shaking (100 rpm) for 24 h. After incubation, the tubes were gently dip-rinsed with PBS to remove loosely bound proteins and transferred to clean culture tubes containing 1.3 mL of washing solution (1 wt % SDS in PBS). The samples were shaken at 100 rpm and 37 °C for 2 h, followed by 10 min of sonication to detach and suspend the adsorbed proteins in the washing solution. The collected solution containing the detached proteins was then analyzed using the BCA assay (Pierce BCA Protein Assay Kit, Thermo Scientific) according to the manufacturer’s protocol, and the protein amount was quantified and expressed as μg/cm^2^ of tube outer surface area.
Hydrogel Solubility Tests
in Serum
2.7.3
0.1 mL of GSNO/HP-αCD-loaded 22 w/v% F127 hydrogel was transferred into the wells of a 24-well plate preheated on a 37 °C hot plate. Prewarmed serum at volumes of 0.5, 1.0, and 1.5 mL was then added to individual wells containing the hydrogel. The plate was gently agitated by hand, and the dissolution behavior of the hydrogel was visually monitored.
Hemolysis Tests
2.7.4
Rat blood was centrifuged at 1000 × g for 10 min to separate the red blood cells (RBCs). The supernatant was discarded, and the RBC pellet was resuspended in PBS to prepare a 10% (v/v) RBC suspension. The NO-releasing hydrogel was mixed with PBS and RBC suspension to reach 2-, 4-, 8-, 16-, and 32-fold dilutions. The final RBC concentration is 5% in these microcentrifuge tubes. PBS and deionized water were used as negative and positive controls, respectively. After 1h of incubation at 37 °C, the sample was centrifuged at 1,000 × g for 5 min, and the absorbance (540 nm) of the collected supernatant was measured by a microplate reader (Varioskan LUX Multimode Microplate Reader). Since GSNO has a pink color that absorbs at 540 nm, the absorbance value was corrected by subtracting the background absorbance of GSNO at the corresponding concentration in PBS (A hydrogel denotes the absorbance after the background correction). Hemolysis (%) was calculated using the following formula:
Cytotoxicity
Tests
2.7.5
L929 murine fibroblast cells were cultured in complete media (EMEM with 1% penicillin/streptomycin and 10% FBS) before being seeded in a 96-well plate at a concentration of 10^4^ cells per well for 24 h. Then, the culture medium was aspirated, and cells were exposed to the 10-, 20-, 40-, 80-, and 160-fold diluted NO-releasing hydrogel or EMEM. After 24 h incubation, cytotoxicity was assessed using a lactate dehydrogenase (LDH) leakage assay following the manufacturer’s protocol (CyQUANT LDH Cytotoxicity Assay C20301). Unexposed cells served as a negative control, and cells exposed to lysis buffer served as a positive control. Absorbance at 490 nm (reference 680 nm) was measured by Varioskan LUX Multimode Microplate Reader, and cytotoxicity was calculated relative to positive and negative controls.
Quantification of GSNO
Decomposition via UV–Vis Absorption Spectroscopy
2.8
GSNO/HP-αCD F127-based hydrogels were placed in 1.5 mL disposable polystyrene cuvettes with caps and stored at 37 °C in the absence of light. Absorbance at 545 nm was measured using a UV–vis spectrophotometer (Go Direct Fluorescence/UV–vis Spectrophotometer). If air bubbles were observed, the cuvettes were placed on ice to temporarily convert the hydrogel to its liquid state, allowing trapped air to be released before measurements. All measurements were performed in triplicate.
Measurement
of NO Release from the Catheter Locks
2.9
A chemiluminescence NO analyzer (ECO PHYSICS nCLD 66) was used to monitor NO diffusion from the outer surface of catheters. Medical-grade silicone catheters (HelixMark 60-011-07; 1.58 mm ID, 2.41 mm OD) were cut into 2.5 cm segments, filled with NO-releasing hydrogel formulations, and tightly sealed at both ends using plastic rod plugs. The sealed catheter segments were immersed in 4 mL of PBS at 37 °C in an amber glass sample cell. The NO analyzer was calibrated using N_2_ and NO gas of a known concentration. During measurements, N_2_ gas was continuously purged into the sample cell at a flow rate of 100 cm^3^/min to carry the released NO into the chemiluminescence detector. Between measurements, all samples were stored separately in 5 mL of PBS at 37 °C in the dark.
Antibacterial Tests
2.10
All three Staphylococcus species used in this study were maintained on LB agar plates and stored at 4 °C. For each experiment, fresh colonies cultured within 48 h were used to ensure viability and consistency. The bacterial inoculum was standardized using a 0.5 McFarland turbidity standard (approximately 1.5 × 10^8^ CFU/mL), and all working suspensions were prepared by diluting the 0.5 McFarland suspension in the appropriate culture medium by a factor of 10,000. All medical-grade silicone catheters (HelixMark 60-011-07), plastic rods, F127 stock solution, phosphate buffer, and other experimental apparatus were sterilized by autoclaving prior to use. The design of the in vitro models, including the selection of growth medium, bacterial inoculum, culture conditions, incubation times, and biofilm quantification protocol, was adapted from previously published methods. ?,?,?,?
Intraluminal Bacterial Migration Tests
2.10.1
Catheters were cut into 4.5 cm long segments. The bottom end of the tube was tightly sealed with a plastic rod. A solution or 22 w/v% F127 hydrogel containing 1% TSB is added into the tube, leaving ∼10 μL of space at the open end. Ten microliters of 10^4^-fold diluted McFarland bacterial suspension in 1% TSB was added to the open end to mimic hub contamination. Each tube was then placed vertically into a sterile culture tube containing sterile PBS at a level just below the open end to maintain a humid condition. After 24h-incubation at 37 °C, 10 μL of liquid or gel was collected from the top and bottom segments of the tube, respectively, for planktonic bacteria quantification. The sample from the top segment was taken after discarding the uppermost 10 μL medium. For biofilm quantification, each tube with the F127 hydrogel was cut in half. The hydrogel was carefully aspirated, and the catheter was gently rinsed with sterile PBS to remove loosely associated bacteria. Then, each segment of tube was transferred into a centrifuge tube containing 2 mL of sterile PBS and subjected to vigorous vortexing for 1 min to dislodge biofilm bacteria. Twenty μL of the resulting bacterial suspension was plated on LB agar plates for plate counting. The final results were expressed as colony-forming units per square centimeter of inner surface area of the tube (CFU/cm^2^).
Intraluminal
Biofilm Prevention Study
2.10.2
The protocol is similar to the biofilm quantification protocol detailed in 2.10.1. The catheter was filled with F127 hydrogel with or without GSNO/HP-αCD. After bacterial inoculation, all tubes were incubated at 37 °C for 3 days before biofilm quantification for the bottom segments.
Extraluminal Biofilm
Prevention Study
2.10.3
Catheter tubes (2.5 cm) were filled with F127 hydrogel or NO-releasing F127 hydrogel and sealed at both ends by plastic rods. The sealed catheters were immersed in 2 mL of 1% TSB containing the 10^4^-diluted 0.5 McFarland bacterial suspension. The bacterial culture medium is refreshed every 24 h. After 72 h, the tubes were retrieved for biofilm quantification on the external catheter surface, which followed the same procedure described above.
Biofilm Eradication Study
2.10.4
To evaluate the biofilm eradication capability of the NO-releasing hydrogel, biofilm of Staphylococcus strains was first established on the catheter. For the intraluminal surface, 2.5 cm tubes were sealed at one end and filled with a bacterial suspension in TSB (∼10^4^ CFU/mL). For the extraluminal surface, 2.5 cm catheter segments sealed at both ends were fully immersed in 2 mL of the same bacterial suspension. All samples were incubated at 37 °C for 24 h to allow for the formation of biofilms on the internal or external surface. For the intraluminal biofilm eradication study, the bacterial culture medium was removed from the tube and the lumen was filled with F127 hydrogel with or without GSNO/HP-αCD. For the extraluminal biofilm eradication study, one end of the tube was unplugged to allow the addition of the F127 hydrogel with or without GSNO/HP-αCD. Then the tubes were transferred into sterile PBS. All tubes were further incubated at 37 °C for an additional 24 h before tube segments were processed for biofilm quantification as described above.
Statistical Analysis
2.10.5
All antibacterial tests were triplicated. Data were presented as mean ± SD. Statistical analysis was performed using the Student’s t test. A p-value <0.05 was considered statistically significant.
Results and Discussion
3
Formulation of NO-Releasing Hydrogels as Catheter
Locks
3.1
A wide range of NO-releasing hydrogels has been developed using natural polymers such as chitosan, alginate, gelatin, and hyaluronic acid, as well as synthetic polymers including polyethylene glycol, polypropylene glycol, poly(acrylic acid), poly(vinyl alcohol) (PVA), and peptide amphiphiles. ?−? ? ? ? ? NO donors, including S-nitrosothiols, N-diazeniumdiolates, metal nitrosyl complexes, organic nitrates, and nitrite, are incorporated into these polymeric systems either through physical blending or chemical attachment to impart NO release capabilities. However, a majority of previous studies on NO-releasing hydrogels have focused on topical applications such as wound healing, treatment of skin infections, and enhancement of dermal blood flow. These applications impose markedly different requirements from those of catheter locks, particularly in terms of mechanical property, hemocompatibility, and NO release characteristics. For example, a key and unique requirement of a hydrogel-based catheter lock is that it must be easily injected into and withdrawn from a CVC without obstruction. F127 is an ideal candidate for this application due to its thermosensitive and thixotropic properties. ?,? F127 is a triblock copolymer with a poly(ethylene oxide)–poly(propylene oxide)–poly(ethylene oxide) (PEO–PPO–PEO) structure. The FDA has approved its use for oral, ophthalmic, and topical medicinal applications. At low temperatures, F127 remains in its liquid state due to the high solubility of its PEO and PPO segments in water. As temperature increases, hydrophobic interactions among PPO chains become dominant, triggering self-assembly of copolymers into micelles. When the F127 concentration in the system is above the critical gelation concentration, these micelles organize into a structured network, resulting in a sol-to-gel transition. This phase transition is reversible. The micelle network disassembles upon cooling, allowing the hydrogel to return to its liquid state. The de Oliveira group pioneered NO-releasing hydrogels using pure F127 as well as F127 mixed with polymers such as poly(acrylic acid) and PVA. ?−? ? F127-based hydrogels and films have been investigated for applications in wound healing and dermal vasodilation. ?−? ? ? ? ? ? Herein, we focus on the development of injectable and withdrawable F127 gels that are hemocompatible, minimize drug leakage, and release desirable levels of NO. Our gel formulations leverage supramolecular chemistry? to achieve properties that make them well-suited as antimicrobial and antithrombotic locks for intravascular catheters.
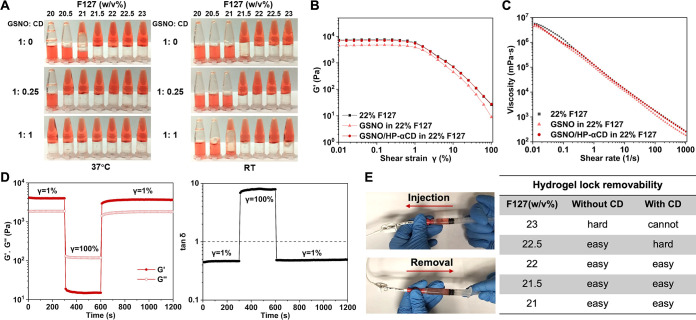
Although F127 is well-known to form thermoresponsive gels, the addition of a drug could perturb the gelation process. To determine the optimal NO-releasing F127 hydrogel formulation, the GSNO stock solution is blended with various F127 formulations in an ice bath, and a tube inversion test is performed after the solutions are incubated at room temperature (RT) and 37 °C for 5 min. As shown in FigureA, in the presence of 0.1 M GSNO, at least 21.5 w/v% F127 is needed to form a hydrogel, even though the gelation of pure F127 only requires a concentration of 17 w/v%.? Previously, we found that αCD and its derivatives can modulate NO release from GSNO solutions by forming GSNO/CD complexes.? Herein, HP-αCD is added to the GSNO stock solution before they are mixed with the F127 solution. With an equimolar amount of HP-αCD and GSNO, the required F127 concentration for hydrogel formation at 37 °C dropped to 20 w/v%. The CD-enhanced gelation presumably occurs because free αCD molecules (those not complexed with GSNO) can thread onto the flanking PEO segments of F127, forming PEO/αCD complexes in the solution state. ?,? As the temperature increases, the formation of microcrystalline PEO/αCD complexes ?,? further enhances the sol-to-gel transition in addition to the original micelle-based gelation mechanism. Dynamic shear rheometer testing demonstrated the same effect of GSNO and CD (FigureB and Figure S2). Although GSNO weakens the gel structure, as indicated by a reduction in storage modulus (G′, FigureB) and an increase in loss factor (tanδ, Table S1), the addition of an equimolar amount of HP-αCD compensated for this GSNO effect, recovering the gel integrity.
Physical characterization, rheological analysis, and functional screening of F127 hydrogels loaded with 0.1 M GSNO. (A) Tube inversion tests after incubating various F127 formulations at RT or 37 °C for 5 min. (B) Storage modulus (G′) as a function of the strain amplitude at a frequency of 10 rad/s at 37 °C. (C) Shear thinning property at 37 °C. (D) Thixotropic property of 22 w/v% F127 containing 0.1 M GSNO and 0.1 M HP-αCD at 37 °C. (E) Injectability and removability of the gel evaluated in a central venous catheter.
The shear-thinning behavior of F127-based hydrogels arises from the reversible disruption of micellar structures under shear. This property allows the material to flow under applied force and is therefore essential to the injectability and removability of the catheter lock. As is shown in FigureC, incorporation of GSNO and HP-αCD did not compromise the overall shear-thinning property. FigureD shows the thixotropic behavior of the F127 gel loaded with GSNO and HP-αCD in a three-step shear test. The shear strain (γ) is successively switched every 300 s from a low amplitude of 1% to a high amplitude value of 100% and again to 1%. Upon application of a transient 100% shear strain, the gel exhibits liquid-like behavior, as indicated by an increase in tan δ to values greater than 1, and rapidly returns to its original state once the shear is removed (FigureD and Figure S3). This shear-thinning and self-healing behavior suggests that the gel lock is both injectable and withdrawable under shear stress, while capable of reverting to a stable gel state after the cessation of mechanical force. We confirmed this injectability and removability using a commercial CVC with its indwelling portion placed in a 37 °C water bath. To illustrate the process, representative videos are provided as Supporting Information (Videos S1–S4). All examined hydrogels can be easily infused into the catheter from a plastic syringe. Hydrogels made of 22.5 w/v% F127 or less in the absence of HP-αCD and made of 22 w/v% F127 or less in the presence of HP-αCD allow obstruction-free aspiration (FigureE). At higher F127 concentrations, the resistance noticeably increases during withdrawal. In particular, the 23 w/v% F127 + HP-αCD formulation could not be aspirated from the catheter.
Spillage
of Solution- and Gel-Based Catheter Locks
3.2
The drug leakage from the lock solution to the bloodstream partially arises due to the laminar flow profile of Newtonian fluids within the catheter, where fluid at the center moves faster than at the periphery (FigureA). Moreover, when a lock solution is instilled to displace the saline flush, the absence of a physical barrier between the lock solution and the saline leads to immediate and inevitable mixing of liquids and, consequently, drug loss to the bloodstream. Experimental and theoretical models indicate that up to 25% of the lock solution can enter circulation upon instilling a volume equal to the catheter’s internal volume, with spillage beginning as early as 50% of lumen filling. ?,?,?,? The speed of manual injection has minimal to no effect on the extent of instillation spillage.? Unlike low-viscosity aqueous solutions, the hydrogel exhibits piston-like behavior during injection due to higher viscosity even under the shear stress and is also less prone to mixing with saline. As a result, chemical spillage out of the catheter is significantly reduced when a gel instead of a solution is being injected as a lock (FigureA). Beyond instillation, additional loss can occur via gravitational sinking and concentration gradient–driven diffusion, particularly for dense or drug-rich lock formulations. ?,? Clinical evidence corroborates such inevitable drug loss with reported systemic adverse effects, including heparin-induced thrombocytopenia, citrate-induced hypocalcemia, ethanol-related neurological symptoms, and gentamicin-associated ototoxicity. ?,?,?,? This fundamental limitation of the liquid lock is expected to be mitigated by switching to a hydrogel-based lock. The hydrogel does not easily sink into the blood and the gel network constrains drug molecules, thereby reducing gradual loss of the drug into the bloodstream after instillation.
*In vitro evaluation of the leakage of the liquid- and gel-based catheter locks. (A) Schematic illustration and a photo showing the flow behavior of liquid and gel locks injected into catheters prefilled with a flush solution (saline). The lock contains a red dye to aid visualization. Quantification of GSNO leakage (B) during instillation (n = 5) and (C) 1 h after instillation (n = 3) for liquid lock versus 22 w/v% F127 hydrogel lock under horizontal and vertical catheter orientations. All formulations contain 0.1 M GSNO and 0.1 M HP-αCD. ***p < 0.001. (D) Photos showing the blood backflow toward the liquid lock instead of the hydrogel lock. (E) GSNO leakage from the hydrogel lock over 6 h under horizontal and vertical catheter orientations (n = 3). (F) GSNO leakage during horizontal instillation of different lock formulations (0.1 M GSNO in 22 w/v% F127 gel, 0.1 M GSNO in 23 w/v% F127 gel, and 0.1 M GSNO/0.1 M HP-αCD in 22 w/v% F127 gel; n = 5). The red arrow indicates the approximate interface between the lock and the prefilled saline. **p < 0.01; **p < 0.001.
To evaluate this hypothesis, we conducted in vitro tests to comprehensively evaluate the leakage of solutions and gels as the catheter locks, incorporating both horizontal and vertical orientations to simulate different clinical scenarios based on patient positioning. The National Kidney Foundation Kidney Disease Outcomes Quality Initiative clinical practice guidelines recommend that CVC tips should be placed in the mid-to-deep right atrium to reduce the risk of catheter malfunction.? When the CVC tip is positioned in the right atrium and surrounded by flowing blood, the gravitational influence on the lock varies depending on whether the patient is in a reclined or upright position during lock instillation. Subsequent patient movements when the catheter is not in use also influence lock leakage over time. The catheter orientation significantly affects the extent of leakage for the solution-based lock formulation. When pushing the prefilled saline with the GSNO/HP-αCD lock solution at a volume equal to that of the catheter lumen, horizontal infusion results in 10.6 ± 0.8% leakage, whereas vertical infusion doubles the leakage (FigureB). In contrast, only less than 4% of GSNO is spilled during the instillation of the hydrogel regardless of the orientation (FigureB). When a catheter filled with the GSNO/HP-αCD solution is suspended vertically with the tip immersed in PBS, nearly 50% of the loaded drug leaked within just 1 h (FigureC). Positioning the catheter horizontally reduced such postinstillation leakage to 10.3 ± 1.2% (FigureC). Similarly, blood backflow is observed when the catheter tip is vertically immersed in blood due to the exchange of the GSNO/HP-αCD solution with blood (FigureD). This phenomenon is primarily attributed to the high density of the GSNO/HP-αCD solution (∼1.166 g/mL). In contrast to the liquid lock, the GSNO/HP-αCD-loaded F127 hydrogel as the lock effectively mitigates these issues, as no blood backflow is observed under the same experimental conditions (FigureD) and no more than 6% GSNO leaks 1 h past the instillation (FigureC). Even after 6 h, only less than 8% of GSNO diffuses away from the gel lock (FigureE), indicating that the hydrogel network effectively retains the loaded drug. Notably, the GSNO-loaded 23 w/v% F127 hydrogel without HP-αCD suffers from significantly more leakage than that in 22 w/v% F127 with HP-αCD (FigureF), even though their viscoelastic properties are similar (Figures S2 and S3). Pure F127 hydrogel is known for its relatively high tendency to dissolve in aqueous solutions.? The formation of supramolecular HP-αCD/PEO domains presumably reduces the gel dissolution in the prefilled saline during the instillation, thereby minimizing spillage. Based on these findings, 22 w/v% F127 hydrogel containing 0.1 M GSNO and 0.1 M HP-αCD was selected for all subsequent studies.
To further prove the reduced spillage of the gel-based catheter lock relative to conventional solution-based lock, we leverage the potent vasodilatory properties of NO as a physiological indicator of intravascular leakage.? The buffer and F127 hydrogel containing GSNO/HP-αCD were alternately instilled into the same rat, with each formulation administered three times. As shown in Figure, each instillation of the solution elicits a rapid and significant decrease in MAP, indicating immediate systemic exposure to NO due to the GSNO spillage. In contrast, no such hemodynamic response is observed following administration of the hydrogel-based formulation, suggesting minimal leakage into circulation.
In vivo assessment of GSNO spillage from the solution-based or hydrogel-based catheter lock using a rat model. The vertical gray lines indicate when the lock is injected. The transient mean arterial pressure (MAP) drop is caused by NO released from the spilled GSNO during instillation. The subsequent recovery of MAP is attributed to the short half-life of NO in circulation and the compensatory baroreceptor reflex.
Hemocompatibility
and Cytotoxicity of the NO-Releasing Gel Lock
3.3
Considering that the lock at the CVC tip is in direct contact with blood, hemocompatibility of the lock medium is a critical safety requirement: the catheter lock should not induce clot formation at the gel-blood interface; the hydrogel should be dissolvable if accidentally introduced into the bloodstream; the lock should not cause significant hemolysis. In our initial efforts to devise hydrogel-based catheter locks, we screened multiple hydrogel candidates, such as those based on synthetic silicate nanoplatelets and PVA. While silicate nanoplatelet-based hydrogel demonstrated excellent shear-thinning behavior, it shows a strong proclivity to induce blood clot formation at the hydrogel–blood interface. In vitro clotting assays show that blood in contact with 6 wt % silicate nanoplatelet hydrogel (FigureA, PC, positive control) clots within 3 min, significantly faster than the control group (FigureA, C, blood only), which clots after 6 min. This procoagulant effect is attributed to electrostatic interactions between the charged nanoplatelet surfaces and the blood components.? Similar clotting behavior has been observed with other clay-based materials, such as kaolin. Moreover, the gelation property of silicate nanoplatelets is substantially impaired with the addition of GSNO, presumably due to the ionic nature of GSNO. As a result, this group of inorganic hydrogels was excluded from further consideration as the catheter lock. In contrast, the F127 hydrogel does not induce clotting earlier than the control (FigureA, F127). More interestingly, no clot adhesion was observed on the surface of the NO-releasing F127 hydrogel over the course of the 6 min assay (FigureA, NO). This aligns with the well-known anticoagulant role of NO because it inhibits platelet aggregation and adhesion. ?−? ? ? ? In addition, NO release also reduces nonspecific protein adsorption on the outer surface of the catheter after serum exposure (Figure S4). Although this study does not focus on a comprehensive evaluation of the anticoagulant and antifouling functions of NO, the NO-releasing hydrogel is expected to exhibit both antimicrobial and antithrombotic properties to mitigate two major complications of CVC, namely infection and thrombosis. This dual-acting property is a highly unique advantage of NO over other drugs used in catheter locks.
Hemocompatibility of the NO-releasing hydrogel lock. (A) Blood clotting tests at 37 °C. C: control (blood only); PC: positive control (6 wt % silicate nanoplatelet gel); F127: 22 w/v% F127 gel; NO: 0.1 M GSNO/0.1 M HP-αCD in 22 w/v% F127 gel. (B) Hemolysis tests of 22 w/v% F127 gel containing 0.1 M GSNO and 0.1 M HP-αCD (n = 3). (C) Cytotoxicity tests of the same hydrogel (n = 3). (D) Photos showing dissolution of the GSNO-HP-αCD-loaded F127 hydrogel in serum.
Hemolysis assays reveal that the GSNO/HP-αCD hydrogel does not lyse red blood cells when diluted 8-fold or more (FigureB). The hydrogel shows no detectable cytotoxicity when diluted 80-fold or more (FigureC). Given the small volume of the catheter lumen (up to 3 mL) relative to the total human blood volume (∼5 L) and the limited leakage of the catheter lock, the hydrogel is unlikely to pose hemolytic or cytotoxic risk. Another important consideration is whether the hydrogel lock can dissolve in blood in case it inadvertently enters the circulation, as insoluble materials may pose a risk of vascular blockage. During our material screening process, hydrogels based on PVA were excluded because even small debris of these hydrogels cannot get dissolved in serum at physiological temperature. In contrast, the F127 hydrogel can be dissolved in serum within 1 min of mild physical agitation (FigureD). Given the continuous flow of blood, the F127 hydrogel formulation will not cause any blood vessel blockage.
NO Release
Profiles of the Hydrogel-Based Catheter Locks
3.4
GSNO is a naturally occurring NO donor that spontaneously decomposes at body temperature to release NO and generate glutathione disulfide (GSSG).? To investigate the NO release kinetics, the decomposition of GSNO with or without HP-αCD in the F127 hydrogel at 37 °C is monitored based on the characteristic UV–vis absorption of GSNO (FigureA). In the absence of HP-αCD, approximately 73% of GSNO decomposes within the first 24 h. In agreement with our previous observations in solution-based systems,? the addition of HP-αCD slows down the GSNO degradation due to the formation of host–guest complexes. When an equimolar amount of HP-αCD is added, the GSNO concentration after 24 h of incubation at 37 °C is nearly doubled compared to the hydrogel without HP-αCD. Furthermore, the lifetime of GSNO is extended from 3 to 5 days due to the presence of HP-αCD.
NO release property of the GSNO-loaded F127 hydrogel. (A) Decomposition of GSNO at 37 °C in 22 w/v% F127 hydrogel with or without equimolar HP-αCD. (B) NO flux measured from the outer surface of sealed catheters filled with GSNO-loaded F127 gels with and without HP-αCD. All experiments were performed in triplicate.
Another distinct advantage of using NO as the antimicrobial agent is that NO can permeate through the polymeric wall of the catheter and thus protect both the intraluminal and extraluminal environments. FigureB shows the NO release from sealed catheter segments filled with GSNO-loaded hydrogel formulations with and without HP-αCD. In the absence of HP-αCD, the initial NO flux exceeds 23 × 10^–10^ mol min^–1^ cm^–2^. Inclusion of HP-αCD suppresses this undesirable initial burst release to approximately 16 × 10^–10^ mol min^–1^ cm^–2^. During the subsequent tests over 3 days, the NO flux from the HP-αCD-containing hydrogel remains consistently higher than that of the CD-free hydrogel. The NO release longevity in the viscous gel is similar to that in the corresponding solution.? Since catheter locks are typically refreshed every 48 to 72 h for CVCs used for hemodialysis,? the NO release profile of the hydrogel lock aligns well with these lock replacement intervals. In real clinical applications, the dry powder of the NO donor and a preformulated gelable solution can be stored separately. A two-compartment device containing a hydrogel compartment and a separate compartment for the dry solid may be designed. At the time of use, the separation barrier can be removed so the NO donor is mixed into the gelable solution.
Antibacterial
Properties of the NO-Releasing Catheter Lock
3.5
Reduction of Microbial
Migration by the Hydrogel-Based Catheter Lock
3.5.1
The prevention and treatment of CRBSIs remain a significant clinical challenge for patients undergoing hemodialysis via a CVC. Approximately 70% of dialysis-related bloodstream infections occur in patients using catheters.? Staphylococcus species are the leading pathogens that cause CRBSIs, with Staphylococcus aureus (S. aureus) accounting for 21–43% of cases, and methicillin-resistant S. aureus (MRSA) reported in 12–38% of cases. ?,? The primary source of catheter infection is closely linked to the duration of catheter use. In short-term cases (<10 days), infections typically originate from cutaneous organisms colonizing the external surface of the catheter, whereas in long-term use (>10 days), infection is more often due to intraluminal spread from the catheter hub (FigureA). ?,?
*NO-releasing gel locks reduce bacterial growth. (A) Schematic illustration of potential routes of bacterial contamination on intravascular catheters. (B) Comparison of S. aureus migration in catheters filled with a liquid or hydrogel medium. (C) 3-day biofilm tests on the intraluminal surface of the catheter filled with a NO-releasing F127 hydrogel and a control hydrogel. The limit of detection is 102 CFU/cm2. (D) 3-day biofilm tests on the extraluminal surface of the catheter. The percent reduction is indicated on each graph. All experiments were performed in triplicate. *p < 0.05; **p < 0.01; **p < 0.001.
While the liquid lock allows bacteria to move freely, the hydrogel lock provides a much more rigid physical matrix that slows down bacterial migration from the catheter hub to the distal end of the catheter. An in vitro bacterial migration model illustrated in FigureB was used to evaluate the effectiveness of the F127 hydrogel in impeding bacterial movement along the catheter. Ten microliters of S. aureus suspension is gently added to the opening of a catheter tube filled with a solution or a hydrogel to mimic hub contamination. After 1-day incubation at 37 °C, the planktonic bacteria in the top half and the bottom half of the catheter lock are quantified. As shown in FigureB, for liquid-filled catheters, S. aureus accumulates in the bottom segment because of facile diffusion and sedimentation. In contrast, the planktonic bacteria are much less in the bottom part of the catheter lock when the lock is a gel, indicating that the hydrogel-based lock as a rigid medium reduces bacterial mobility. However, F127 hydrogel alone cannot completely block bacterial migration over time without being combined with antimicrobial agents. The continuous growth of bacterial biofilm along the inner surface of the catheter will ultimately lead to infection. We confirmed that significant bacterial biofilms are formed throughout the catheter over the period of 3 days (Figure S5), necessitating the use of an antibacterial drug in the catheter lock.
Prevention
of Intraluminal Biofilm Formation by the NO-Releasing Gel Lock
3.5.2
For patients with long-term catheter use and a history of CRBSIs, clinical practice guidelines recommend the use of highly concentrated antibiotic lock solutions, typically 100 to 1,000 times higher than the minimal inhibitory concentration (MIC).? However, as discussed above, leakage of such high-concentration antibiotics into the bloodstream is inevitable, raising concerns about systemic side effects and the promotion of antibiotic resistance. NO is a highly reactive free radical with potent antimicrobial properties. ?−? ? ? It quickly reacts with oxygen and superoxide from the microbiological environment to produce reactive oxygen and nitrogen species, which place oxidative and nitrosative stress on microbes. ?,? Unlike traditional antibiotics that typically act through a single mechanism, NO exhibits multifaceted antimicrobial activities, ranging from enzyme deactivation and lipid peroxidation, to membrane disruption and direct damage to microbial DNA and DNA repair systems. ?,?,? These broad and overlapping mechanisms make NO a potent, broad-spectrum antimicrobial agent. We compared the viable bacterial biofilm attached to the bottom catheter segment when the catheter is filled with the F127 hydrogel with and without GSNO/HP-αCD. Three Staphylococcus strains, commonly implicated in CRBSIs, were tested as representative pathogens. After 3 days of incubation, although the drug-free hydrogel lock allows for significant growth of bacteria, no viable bacteria can be detected from the catheter segments filled with the NO-releasing hydrogel, across all three strains (FigureC). Similarly, the inhibitory effect was observed against representative Gram-negative species, including E. coli, P. aeruginosa, and K. pneumoniae (Figure S6). The substantial reduction in biofilm formation demonstrates that the NO-releasing hydrogel lock is highly effective in preventing intraluminal bacterial colonization.
Reduction of Extraluminal Biofilm Formation
by the NO-Releasing Gel Lock
3.5.3
While the majority of CRBSIs originate from hub contamination, a significant portion of CRBSIs are associated with bacterial colonization on the extraluminal surface. ?,? These extraluminal infections typically result from improper handling during catheter implant or from patient skin flora entering the body through the insertion site.? Therefore, preventing bacterial colonization along the outer surface of the catheter is also important for comprehensive infection control. Traditional antibacterial agents in lock solutions are confined within the catheter lumen due to their negligible diffusivity in the catheter wall. Therefore, they cannot target bacteria colonizing the external surface of the catheter. In contrast, NO is a tiny gaseous molecule capable of diffusing through polymeric catheter materials, offering a unique advantage in addressing extraluminal infections. This nondirect-contact antimicrobial protection provided by NO-releasing locks has been previously reported by the Brisbois Group, the Schoenfisch group, and our group. ?,?,? To evaluate the effectiveness of the NO-releasing gel lock in preventing extraluminal infections, catheter segments filled with hydrogel are sealed at both ends and incubated with the three representative Staphylococcus strains. On the third day, the biofilm formed on the outer surface of the catheter is quantified. As shown in FigureD, 1-to 2-log reductions in biofilm are obtained on NO-releasing catheters compared to the control catheters. Specifically, S. aureus, MRSA, and S. epidermidis exhibit a 91.0%, 99.4%, and 98.9% reduction, respectively, confirming antibacterial protection on the extraluminal catheter surface provided by the NO generated from the hydrogel and diffused across the polymeric catheter wall.
Treatment of Catheter
Infection by the NO-releasing Gel Lock
3.5.4
If a CVC is already contaminated, antibiotic lock therapy may be employed to eradicate established biofilms that form on the internal surface of the catheter. ?,? However, antibiotics often possess limited effectiveness against established biofilms, largely due to the extracellular polymeric substances (EPS) that impede drug penetration into the biofilm.? In contrast, NO is capable of diffusing through the EPS matrix, disrupting the biofilm structure and exposing the bacteria.? We evaluated the biofilm eradication efficacy of the NO-releasing hydrogel lock. Catheter segments are sealed at one end, inoculated with three types of bacterial cultures, respectively, and incubated for 24 h to allow biofilm formation on the intraluminal surface. After incubation, the bacterial culture medium is removed, and the catheter lumen is filled with the hydrogel with or without GSNO/HP-αCD, followed by an additional 24-h incubation. After the 1-day treatment, reduced biofilm growth is observed across all three tested strains (FigureA). The S. epidermidis biofilm shows the most dramatic response to NO, with viable cell counts reduced by ∼2 orders of magnitude. The biofilm biomass of S. aureus and MRSA decreases to 16.5% and 5% of the untreated controls, respectively.
*NO-releasing hydrogel lock eradicates established bacterial biofilms on (A) inner and (B) outer catheter surfaces. Established biofilms are treated with the F127 hydrogel lock containing 0.1 M GSNO and 0.1 M HP-αCD for 24 h. The percent reduction is indicated on each graph. All experiments were performed in triplicate.*p < 0.05; **p < 0.01; **p < 0.001.
As discussed previously, current antibiotic lock therapies are ineffective against infections occurring on the outer surface of catheters because organic molecules cannot readily diffuse across the catheter wall. To assess whether our NO-releasing hydrogel lock could disperse and kill bacteria on the outer surface of the catheter, the hydrogel is added to the catheter segment that has established bacterial biofilms on the external surface. Both ends of the catheter segment are sealed so NO can only reach the outer surface via the catheter wall. Remarkably, despite the biofilms being located on the opposite side of the catheter wall, the NO-releasing hydrogel is still able to substantially reduce mature biofilm (FigureB). Following the 24-h treatment, there is at least a 90% reduction in biofilm biomass compared to controls for all three bacterial strains. These results underscore the highly unique efficacy of NO as a diffusive small-molecule drug in preventing and treating catheter-associated infections.
Conclusions
4
Catheter locks based on liquid formulations often spill into the bloodstream during instillation due to the parabolic flow pattern and subsequently mix with blood owing to the absence of a defined interface. When the lock solution contains drugs such as antimicrobial and anticoagulant agents, this spillage can lead to systemic toxicity and reduced therapeutic efficacy. In contrast, the use of a hemocompatible thixotropic hydrogel as a catheter lock significantly minimizes spillage and mixing by 2–5 folds, thereby slowing drug loss. When combined with GSNO, the hydrogel effectively inhibits bacterial growth by 1–3 orders of magnitude through sustained NO release. Future work may explore alternative hydrogel systems to fine-tune thixotropic properties, viscosity, stability, and NO release kinetics. Additional functions of NO-releasing hydrogel locks, such as inhibition of platelet aggregation and modulation of inflammatory responses, will also be systematically examined in future studies. Beyond central venous catheters, this hydrogel lock concept may also be extended to other types of catheters, such as peritoneal dialysis catheters and biliary drainage catheters.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kehagias E.Galanakis N.Tsetis D.Central Venous Catheters: Which, When and How British Journal of Radiology 20239611512022089410.1259/bjr.2022089437191031 PMC 10607393 · doi ↗ · pubmed ↗
- 2Wang Y.Sun X.Reevaluation of Lock Solutions for Central Venous Catheters in Hemodialysis: A Narrative Review Renal Failure 20224411502151810.1080/0886022 X.2022.2118068 · doi ↗
- 3Beathard, G. Malfunction of chronic hemodialysis catheters - Up To Date. 2025. https://www.uptodate.com/contents/malfunction-of-chronic-hemodialysis-catheters.
- 4CDC. Surveillance Summary of Bloodstream Infections in Outpatient Hemodialysis Facilities National Healthcare Safety Network, 2014–2019. 2014. https://www.cdc.gov/dialysis-safety/media/pdfs/BSI-NHSN-2014 to 2019-508.pdf.
- 5Harron K.Mok Q.Hughes D.Muller-Pebody B.Parslow R.Ramnarayan P.Gilbert R.Steyerberg E. W.Generalisability and Cost-Impact of Antibiotic-Impregnated Central Venous Catheters for Reducing Risk of Bloodstream Infection in Paediatric Intensive Care Units in England P Lo S One 201611 e 015134810.1371/journal.pone.015134826999045 PMC 4801221 · doi ↗ · pubmed ↗
- 6CDC. Background Information: Strategies for Prevention of Catheter-Related Infections in Adult and Pediatric Patients. 2011. https://www.cdc.gov/infection-control/hcp/intravascular-catheter-related-infection/prevention-strategies.
- 7Sousa C.Henriques M.Oliveira R.Mini-Review: Antimicrobial Central Venous Catheters – Recent Advances and Strategies Biofouling 201127660962010.1080/08927014.2011.59326121718230 · doi ↗ · pubmed ↗
- 8Kim E. Y.Saunders P.Yousefzadeh N.Usefulness of Anti-Infective Lock Solutions for Catheter-Related Bloodstream Infections Mount Sinai Journal of Medicine 201077554955810.1002/msj.2021320960556 · doi ↗ · pubmed ↗