Effect Modifiers of Graded Sensorimotor Retraining for Chronic Low Back Pain: A Secondary Analysis of the RESOLVE Randomized Trial
Martjie Venter, James H. McAuley, Harrison J. Hansford, Mia Ryan, Matthew K. Bagg, Benedict M. Wand, Aidan G. Cashin

TL;DR
This study examines whether certain factors influence the effectiveness of a treatment for chronic low back pain over time.
Contribution
The study identifies back perception as a potential modifier of treatment outcomes for chronic low back pain at long-term follow-up.
Findings
Back perception was a potential treatment effect modifier for pain intensity at 52 weeks.
Most baseline variables showed no strong evidence of modifying treatment effects.
Future research is needed to explore potential modifiers further.
Abstract
This secondary analysis of a randomized clinical trial assesses changes in pain intensity and disability level associated with 8 treatment effect modifiers among people with chronic low back pain. Which variables modify the effect of graded sensorimotor retraining on pain intensity and disability level at 18 weeks and 52 weeks of follow-up? In this secondary analysis of a randomized clinical trial involving 276 participants, there was limited evidence of treatment effect modification by the 8 baseline variables identified. Back perception was identified as a potential treatment effect modifier for pain intensity at the 52-week follow-up time point. These findings suggest that the benefits of graded sensorimotor retraining may be similar for all people with chronic low back pain, regardless of individual differences at baseline. Outcomes for people with low back pain (LBP) may be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Treatment effect modifier | Variable assessment | Supporting evidence | Rationale | Hypothesized direction |
|---|---|---|---|---|
| Psychoactive medication use | Dichotomous (yes, no)— | Beneciuk et al, | Psychoactive medication use affects CNS processing, which may influence a person’s capacity to engage with the intervention | No medication use > medication use |
| Pain intensity | Continuous (scale: 0-10)— | Gurung et al, | People with more severe pain likely have more pronounced sensorimotor disruption and maladaptive pain processing, providing greater potential for an improved response to treatment | Higher baseline pain intensity > lower baseline pain intensity |
| Disability level | Continuous— | Gurung et al, | People with more functional limitations may respond better to a treatment aimed at restoring movement confidence and control | Higher baseline disability level (ie, poorer physical function) > lower baseline disability level |
| Beliefs about back pain consequences | Continuous— | Cashin et al, | The intervention challenges maladaptive beliefs about the back pain consequences; therefore, those with negative beliefs about back pain consequences may respond better | Negative beliefs about back pain consequences > positive beliefs about back pain consequences |
| Kinesiophobia | Continuous— | Murillo et al, | The intervention progressively exposes individuals to feared movements, targeting movement-related fear; therefore, those with worse fear of movement may respond better | Higher kinesiophobia > lower kinesiophobia |
| Pain catastrophizing | Continuous— | Cashin et al, | Higher catastrophizing reflects stronger maladaptive pain cognitions, which the intervention targets; therefore, those with higher pain catastrophizing may respond better | Higher pain catastrophizing > lower levels of pain catastrophizing |
| Pain self-efficacy | Continuous— | Roseen et al, | Greater pain self-efficacy may facilitate better engagement with and adherence to the intervention; therefore, these people may respond better | Higher pain self-efficacy > lower pain self-efficacy |
| Back perception | Continuous— | Wand et al, | The intervention targets disrupted back perceptions; therefore, those with higher levels of body perception disturbances may respond better | Higher levels of body perception disturbance > lower levels of body perception disturbance |
| Characteristic | Participant group | |
|---|---|---|
| Treatment (n = 138) | Sham control (n = 138) | |
| Age, y | 44.7 (14.5) | 47.0 (14.1) |
| Sex, No. (%) | ||
| Female | 72 (52.2) | 66 (47.8) |
| Male | 66 (47.8) | 72 (52.2) |
| Educational level, No. (%) | ||
| University-level degree | 77 (55.8) | 77 (56.2) |
| Diploma | 19 (13.8) | 20 (14.6) |
| Vocational certificate | 17 (12.3) | 18 (13.1) |
| Year 12 | 18 (13.0) | 10 (7.3) |
| Year 10 | 7 (5.1) | 12 (8.8) |
| Duration of current episode of LBP, median (IQR), y | 5 (4-10) | 6 (3-11) |
| Work absence or reduction, No. (%) | 27 (19.6) | 26 (18.8) |
| Compensation claimed, No. (%) | 9 (6.5) | 17 (12.3) |
| Insomnia Severity Index | 13.5 (7.7) | 14.0 (7.5) |
| Depressive symptoms score | 4.6 (5.0) | 5.0 (4.9) |
| Potential treatment effect modifiers | ||
| Pain intensity | 5.6 (1.8) | 5.8 (1.8) |
| Disability level | 9.6 (5.4) | 10 (5.0) |
| Psychoactive medication use, No. (%) | 28 (20.3) | 36 (26.1) |
| Pain catastrophizing | 19.1 (12.7) | 21 (12.8) |
| Beliefs about back pain consequences | 26.2 (6.6) | 25.6 (6.4) |
| Kinesiophobia | 38.5 (7.6) | 38.4 (7.3) |
| Pain self-efficacy | 40.4 (13.7) | 38.7 (13.0) |
| Back perception score | 6.96 (5.0) | 7.91 (4.7) |
| Potential treatment effect modifier | Pain intensity | Disability level | ||||||
|---|---|---|---|---|---|---|---|---|
| 18-wk Follow-up | 52-wk Follow-up | 18-wk Follow-up | 52-wk Follow-up | |||||
| Interaction coefficient (95% CI) | Interaction coefficient (95% CI) | Interaction coefficient (95% CI) | Interaction coefficient (95% CI) | |||||
| Psychoactive medication use (yes/no) | 0.19 (−1.21 to 1.60) | .79 | −0.04 (−1.58 to 1.50) | .96 | 1.43 (−1.58 to 4.45) | .35 | 0.16 (−2.91 to 3.22) | .92 |
| Pain intensity (scale: 0-10) | −0.16 (−0.47 to 0.15) | .31 | −0.13 (−0.46 to 0.21) | .46 | −0.29 (−0.99 to 0.40) | .41 | −0.37 (−1.11 to 0.36) | .32 |
| Disability level (scale: 0-24) | 0.02 (−0.01 to 0.13) | .72 | 0.04 (−0.08 to 0.17) | .48 | −0.15 (−0.38 to 0.07) | .17 | 0.13 (−0.37 to 0.10) | .26 |
| Beliefs about back pain consequences (scale: 9-45) | −0.04 (−0.14 to 0.05) | .37 | −0.04 (−0.14 to 0.05) | .39 | 0.06 (−0.14 to 0.26) | .57 | 0.16 (−0.05 to 0.37) | .14 |
| Kinesiophobia (scale: 17-68) | 0.06 (−0.02 to 0.14) | .15 | 0.07 (−0.02 to 0.16) | .12 | −0.01 (−0.18 to 0.16) | .92 | −0.02 (−0.20 to 0.15) | .79 |
| Pain catastrophizing (scale: 0-52) | 0.02 (−0.03 to 0.06) | .51 | 0.01 (−0.04 to 0.06) | .69 | 0.01 (−0.01 to 0.12) | .85 | 0.00 (−0.10 to 0.10) | .93 |
| Pain self-efficacy (scale: 0-60) | 0.00 (−0.05 to 0.04) | .86 | 0.00 (−0.04 to 0.05) | .85 | 0.03 (−0.06 to 0.12) | .47 | 0.04 (−0.06 to 0.13) | .46 |
| Back perception (scale: 0-36) | 0.10 (−0.02 to 0.22) | .09 | 0.18 (0.05 to 0.32) | .007 | 0.22 (−0.04 to 0.48) | .10 | 0.27 (0.00 to 0.55) | .05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Pain Management and Treatment · Muscle activation and electromyography studies
Introduction
Low back pain (LBP) contributes the largest share of the disability burden worldwide.^1^ In 2020, LBP affected 619 million people globally,^1^ with one-third of this population likely to report chronic, ongoing pain and disability for more than 3 months after symptom onset.^2^ People with chronic LBP have a poor prognosis^3,4^ and account for a disproportionately large percentage of the burden associated with LBP due to ongoing treatment costs, loss of work productivity, and reduced quality of life.^5,6^
A top priority in LBP research is to identify effective and cost-effective treatments for subgroups of individuals who may have differential treatment responses.^7,8,9^ These subgroups comprise patients who share characteristics such as symptoms or prognostic factors.^10^ The targeted use of effective treatments for certain subgroups of people with chronic LBP has the potential to improve treatment outcomes. A new theoretically informed treatment for chronic LBP—graded sensorimotor retraining^11^—demonstrated clinically meaningful and sustained improvements in pain intensity and disability level when investigated in a sham- and attention-controlled randomized clinical trial.^12^ Although graded sensorimotor retraining was effective, it remains unclear whether certain baseline characteristics may modify the treatment effect (effect modification).
There is a need to investigate variables that modify the effect (also known as moderators) of graded sensorimotor retraining both to optimize the treatment and to facilitate its implementation in practice for people with chronic LBP.^13^ By identifying baseline characteristics associated with treatment response, the results may guide the refinement of the intervention to target less responsive groups and facilitate delivery in clinical settings to people more likely to benefit. Guidelines for treatment effect modification studies state that the hypothesized moderators should be prespecified based on sound theoretical support and relevant expert consultation.^14,15^ This study aimed to investigate potential treatment effect modifiers of graded sensorimotor retraining affecting pain intensity and disability level in the short and long terms for people with chronic LBP.
Methods
Study Design, Setting, and Participants
This post hoc secondary analysis was declared in a statistical analysis plan^16^ (Supplement 1) after completion of the RESOLVE trial, a 2-group parallel, sham-controlled randomized clinical trial conducted at a medical research institute in Sydney, Australia.^12^ We performed a moderation analysis using data from this trial. The trial protocol^17^ and statistical analysis plan^18^ outlining the methods were published previously, as were the main findings,^12^ mediation analysis,^19^ and qualitative analyses,^20,21^ providing detailed information on the trial design, procedures, and findings. The University of New South Wales Human Research Ethics Committee approved the trial. All participants provided written informed consent prior to trial enrollment.
Participants were recruited by direct referral from primary care clinicians and from the community through local and online advertisements. Eligible participants were adults between 18 and 70 years of age who reported chronic nonspecific LBP (lasting ≥12 consecutive weeks), with or without associated leg pain, that was rated a minimum of 3 out of 10 on an 11-point Numerical Rating Scale (NRS). Additionally, participants were required to speak fluent English, have internet access, and have a trusted person to assist them with the home components of the intervention. Participants were excluded if they had radicular pain; had LBP caused by a serious medical condition (infection, fracture, or malignant neoplasm); were pregnant or gave birth in the previous 6 months; had undergone spinal surgery in the past 12 months or were scheduled for major surgery in the upcoming 12 months; had an uncontrolled mental health condition that would prevent participation; and had any other contraindications to physical activity, transcranial direct current stimulation, cranial electrical stimulation, low-intensity laser therapy, or short-wave diathermy.
Participants were randomized between December 10, 2015, and July 25, 2019, and follow-up was completed by February 3, 2020. This secondary analysis was conducted from November 5, 2024, to May 27, 2025.
Randomization and Blinding
Participants were randomly allocated (1:1) through sealed, opaque, sequentially numbered envelopes to receive either graded sensorimotor retraining (treatment group) or the matched attention control and sham procedures (sham control group). Random allocation occurred immediately after baseline assessment when the clinician opened the next numbered envelope. The randomization sequence was generated using a computer-generated block randomization (random block size range, 2-10). Participants as well as the researchers collecting and analyzing outcome data were blinded to the group allocation. To maintain blinding, participants were informed that both interventions targeted the central nervous system and back function, and no trial information was publicly disclosed. The trial clinicians remained unblinded.
Interventions
Both treatment and control interventions consisted of 12 in-person sessions, each lasting 1 hour, that were delivered by trained study clinicians. Participants were required to complete a home treatment program approximately 5 times per week for 30 minutes. Detailed intervention descriptions can be found in the published trial findings^12^ and protocol.^17^
Graded Sensorimotor Retraining
Graded sensorimotor retraining is a rehabilitation package developed from the theoretical framework described in the fit-for-purpose model,^11^ which evolved from the maladaptive perceptions model.^22,23^ This intervention package integrates approaches (pain science education, premovement training, and graded movement and loading) that have a clinically meaningful effect on pain and disability.^24,25,26^ The first component of the package aims to help the person understand that it is safe and helpful to move. This educational component is delivered across the 12 sessions and focuses on contemporary pain science.^24^ The second component aims to refine neural representations of the back and the precision of sensorimotor processing so that the back feels safe to move. This aim is achieved through premovement training,^25^ which incorporates both tactile precision practice and mental rehearsal of movement through graded motor imagery as well as active exercises designed to improve proprioceptive precision. The third component aims to load the back to promote beneficial tissue adaptations and enable the individual to experience safety with movement of increasing complexity and load. This aim is achieved through precision-focused and feedback-enriched graded movement and loading until return to functional goals.^26,27^
Attention Control and Sham Procedures
Attention control and sham procedures involved discussion of the participant’s back pain experience without advice or education provided, sham laser therapy to the most painful area of the back, sham shortwave diathermy to the back, and sham transcranial direct current stimulation applied to the motor and prefrontal cortices on the contralateral side of the worst pain. Participants were provided with a sham cranial electrical device to use at home. The intervention was designed to control for time with an expert clinician, graded progression of treatment in the active intervention and expectation of a central nervous system–directed component of care (as outlined in the trial protocol and participant information sheet), and matching the active intervention’s home component.
Outcome Measures
The primary outcomes for this study were pain intensity (measured with the 11-point NRS, with a score range of 0 [indicating no pain] to 10 [indicating worst imaginable pain]) and disability level (measured with the 24-item Roland-Morris Disability Questionnaire [RMDQ], with a scale range of 0-24 [higher scores indicating greater levels of disability]) assessed at 18 weeks and 52 weeks after randomization. These outcomes were included because they represent distinct dimensions of LBP, align with established core outcome sets for LBP,^28^ and reflect the priorities identified by people with a lived experience.^29^
Potential Treatment Effect Modifiers
Prior to randomization, baseline characteristics were collected from participants using self-reported questionnaires. Eight potential treatment effect modifiers were selected—psychoactive medication use,^30,31,32,33,34^ pain intensity,^31,35,36,37^ disability level,^31,37,38,39^ beliefs about back pain consequences,^19,40^ kinesiophobia,^41^ pain catastrophizing,^19^ pain self-efficacy,^19,40,42^ and back perception^22^—that represent common clinical and psychosocial characteristics observed in populations with chronic LBP. These variables were selected based on prior evidence of moderation or their theoretical relevance to the graded sensorimotor retraining intervention. Table 1 describes the 8 potential treatment effect modifiers as well as the assessment method, supporting evidence, rationale, and hypothesized direction for each moderator variable. We selected these effect modifiers and specified their hypothesized direction in the statistical analysis plan prior to executing the moderation analysis.^10,15,16,43^
Statistical Analysis
Main Analysis
Baseline demographic and clinical characteristics were summarized using counts (percentages) for categorical variables and means (SDs) or medians (IQRs) for continuous variables. We conducted a formal moderation analysis using a test for statistical interaction.^14,43^ We used separate linear regression models at the 18-week and 52-week follow-up time points to evaluate a potential moderator variable against each outcome by incorporating a group-moderator interaction term in each model. We examined residual plots to assess linearity, normality, and homoscedasticity; leverage and influence plots to detect influential outliers; and scatterplots to check for collinearity. We identified no threat to the assumptions for each model. Each model was constructed using a term for outcome (pain intensity or disability level), group allocation, and potential moderator and an interaction term for group and moderator. We estimated the effect size and 95% CI and reported them alongside the P value for each group-moderator interaction. The moderation effect of the dichotomous moderator variable (ie, psychoactive medication use) was interpreted as the difference in intervention effect (treatment vs sham control) between participants who used and did not use medication. The moderation effect of the continuous moderator variables was interpreted as the difference in intervention effect (treatment vs sham control) for a single unit change in the moderator. We considered P < .20 as hypothesis generating and P < .05 as statistically significant, similar to previous studies investigating treatment effect modifiers.^30,31^ Statistical analyses were conducted from November 11 to December 6, 2024, using R, version 4.4.2 (R Project for Statistical Computing).^44^
Missing Data
We assessed the proportions and patterns of missing data for the moderator and outcome variables and performed multiple imputation by chained equations^45^ for 10 datasets using the mice package^46^ in R, version 4.4.2.^44^ The imputation model included baseline covariates (age, sex, back pain duration, other areas of pain, work absence, compensable status, educational level, depressive symptoms score, and Insomnia Severity Index), group allocation, outcome variables at the 18-week and 52-week follow-up time points, and all potential moderator variables. Estimates were pooled using Rubin rules,^47^ and all reported results were based on the pooled imputed estimates.
Results
Sample Characteristics
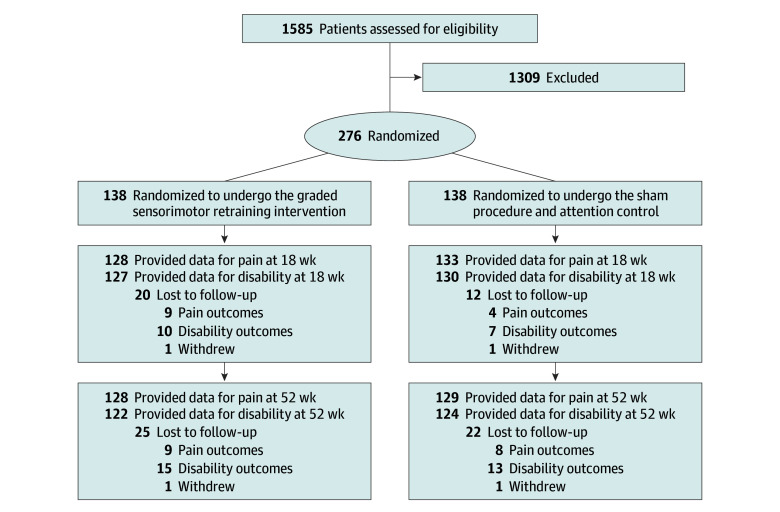
A total of 276 participants were enrolled in the RESOLVE trial, 138 of whom were randomized to the treatment group and 138 of whom were randomized to the sham control group. Figure shows the flow of trial participants.
RESOLVE Trial Participant Flowchart
Baseline characteristics for included participants are summarized in Table 2. The mean (SD) age was 46 (14.3) years; there were 138 females (50.0%) and 138 males (50.0%); and 154 participants (55.8%) had a university-level degree. At baseline, participants had moderate to high pain intensity scores (mean [SD] NRS score, 5.7 [1.8]) and moderate disability levels (mean [SD] RMDQ score, 9.8 [5.2]). There were no missing data for the moderator variables. Proportions of missing data for the outcome variables were 5.4% at 18 weeks and 6.9% at 52 weeks of follow-up for pain intensity and 6.9% at 18 weeks and 10.9% at 52 weeks of follow-up for disability level.
Treatment Effect Modifiers
Table 3 reports the effect size and statistical significance of the group-moderator interactions between each of the 8 investigated moderator variables and pain intensity and disability level at 18 weeks and 52 weeks of follow-up. There was no evidence that baseline psychoactive medication use, pain intensity, disability level, pain catastrophizing, and pain self-efficacy modified the effect of the intervention (graded sensorimotor retraining vs attention control and sham procedures) on pain intensity at the 18-week or 52-week follow-up time points. Similarly, there was no evidence that baseline psychoactive medication use, pain intensity, beliefs about back pain consequences, kinesiophobia, pain catastrophizing, and pain self-efficacy modified the effect of the intervention on disability level at 18 weeks after randomization. Baseline psychoactive medication use, pain intensity, disability level, kinesiophobia, pain catastrophizing, and pain self-efficacy also did not modify the intervention effect on disability level at 52 weeks after randomization.
The effect of the intervention on pain intensity was modified by back perception at 52 weeks of follow-up (β-coefficient = 0.18 [95% CI, 0.05-0.32]; P = .007) (Table 3). People with higher levels of disrupted back perception at baseline experienced less benefit from graded sensorimotor retraining at the 52-week follow-up time point.
Hypothesis-Generating Evidence for Treatment Modification
Hypothesis-generating evidence showed that higher levels of kinesiophobia may modify the effect of the intervention on pain intensity at the 18-week (β-coefficient = 0.06 [95% CI, −0.02 to 0.14]; P = .15) and 52-week (β-coefficient = 0.07 [95% CI, −0.02 to 0.16]; P = .12) follow-up time points; however, the 95% CIs included no moderating effect. Lower levels of disability at baseline may modify the effect of the intervention on disability level at 18 weeks (β-coefficient = −0.15 [95% CI, −0.38 to 0.07]; P = .17), and positive beliefs about back pain consequences may modify the effect of the intervention on disability level at 52 weeks of follow-up (β-coefficient = 0.16 [95% CI, −0.05 to 0.37]; P = .14); however, the 95% CIs included no moderating effect. Finally, higher levels of disrupted back perception may modify the effect of the intervention on pain intensity and disability level at the 18-week (β-coefficient = 0.10 [95% CI, −0.02 to 0.22; P = .09] and 0.22 [95% CI, −0.04 to 0.48; P = .10]) and disability level at the 52-week (β-coefficient = 0.27 [95% CI, 0.00-0.55]; P = .05) follow-up time points; however, the 95% CIs included no moderating effect.
Discussion
This exploratory secondary analysis of data from the RESOLVE trial sought subgroups of individuals who might respond differently to graded sensorimotor retraining compared with attention control and sham procedures. We found limited evidence of any prominent treatment effect modifiers. Participants presenting with chronic LBP and lower levels of disrupted back perceptions may benefit more from graded sensorimotor retraining in the long term. Our findings suggest the benefits of graded sensorimotor retraining are likely to be similar for people presenting with typical characteristics of chronic nonspecific LBP.
To our knowledge, back perception has not been investigated as a treatment effect modifier for people with chronic LBP. The development of graded sensorimotor retraining was informed by evidence that back perceptions may become disrupted following nociplastic changes associated with chronic LBP,^48^ which can contribute to and maintain pain,^22,49^ and that improvements in back perception are associated with reduced pain and disability.^25,50^ Counter to our hypothesis, people with less disrupted back perceptions experienced greater benefits with graded sensorimotor retraining. A reason for this finding may be that individuals with higher levels of body perception disturbance found it difficult to engage with the intervention effectively (particularly the premovement tasks) or that the ability of the intervention to affect back perception remains uncertain.^19^ This finding that back perception was a treatment effect modifier requires replication to determine whether the observed result was spurious or might instead reflect the measurement tool used (Fremantle Back Awareness Questionnaire^22^), which has not undergone adequate content validation; trial sample characteristics (eg, low levels of [ie, better] back perception); or a surrogate for another unmeasured factor (eg, emotional regulation), which may be more directly associated with the outcome of interest. An investigation of the role of back perceptions in other brain- and body-directed treatments^51,52^ for LBP may help guide the targeting of these interventions to relevant patient groups.
Lower disability levels, positive beliefs about back pain consequences, and higher levels of kinesiophobia at baseline were identified as possible treatment effect modifiers. We considered P < .20 as hypothesis-generating evidence of effect modification, identifying factors that may be worth investigating in future studies with larger sample sizes. Future trials should measure and continue to review the role of moderator variables as subgroups that may affect treatment responses. However, for this hypothesis-generating evidence (P < .20), the 95% CI included no moderation effect; therefore, these results need to be interpreted with caution.
This secondary analysis provided evidence to move the implementation of graded sensorimotor retraining from a research setting to clinical practice. The treatment appears to be suitable for people with chronic nonspecific LBP in primary care. Assessing the back perceptions of patients presenting with chronic LBP using validated tools (eg, Fremantle Back Awareness Questionnaire^22^) may be informative for identifying those who may not experience as great a benefit and for guiding treatment decisions. For example, clinicians should be mindful that people with high scores on the Fremantle Back Awareness Questionnaire may require extra support throughout the course of the intervention, beyond what is currently provided in the intervention. Extra support may include augmenting sensory feedback^53^ (eg, virtual reality or biofeedback), slowing task progression, or increasing premovement training before progressing to movement tasks. Back perception could also be considered in future trial design, particularly when making decisions about participant selection criteria,^54^ and for inclusion in future clinical prediction tools.^55^ Finally, future randomized clinical trials should be designed with larger sample sizes to statistically accommodate for and prospectively plan moderation analyses.
Strengths and Limitations
This study has several strengths. First, we used data from the RESOLVE trial, a high-quality sham-controlled randomized clinical trial with limited missing data.^12^ Second, we followed methodological guidelines for studies investigating treatment effect modifiers, including selecting a limited set of theory-informed variables prior to executing the analysis.^14,15^ Third, we evaluated all continuous treatment effect modifier variables in their continuous form, rather than dichotomizing them. Fourth, the baseline clinical and demographic characteristics of the study sample were comparable with those of patients with chronic LBP, suggesting that the results are generalizable.
This study also has some limitations. First, the RESOLVE trial was not powered for a moderation analysis, which is common in the effect modification literature.^14^ Second, the treatment effect modification on pain intensity and disability level, although statistically significant and clinically meaningful, was small and moderate, respectively,^56^ which may reduce the plausibility for finding significant moderators. Third, the sham control comparison may have limited our ability to detect treatment moderators, given that both groups likely engaged active mechanisms, masking subgroup differences. Fourth, we investigated a single variable at a time, which may affect the ability of findings to directly inform clinical decision-making because patients may have multiple varying characteristics.
Conclusions
This study found limited evidence of subgroups of people with chronic LBP who respond differently to graded sensorimotor retraining vs attention control and sham procedures. Similar benefits are likely for all people with chronic nonspecific LBP. Future clinical trials are needed to explore the treatment effect modifiers identified in this study and to assess their role in LBP management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferreira ML, de Luca K, Haile LM, ; GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e 316-e 329. doi:10.1016/S 2665-9913(23)00098-X 37273833 PMC 10234592 · doi ↗ · pubmed ↗
- 2Henschke N, Maher CG, Refshauge KM, . Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study. BMJ. 2008;337(7662):a 171. doi:10.1136/bmj.a 171 18614473 PMC 2483884 · doi ↗ · pubmed ↗
- 3da C Menezes Costa L, Maher CG, Hancock MJ, Mc Auley JH, Herbert RD, Costa LOP. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184(11):E 613-E 624. doi:10.1503/cmaj.111271 22586331 PMC 3414626 · doi ↗ · pubmed ↗
- 4Wallwork SB, Braithwaite FA, O’Keeffe M, . The clinical course of acute, subacute and persistent low back pain: a systematic review and meta-analysis. CMAJ. 2024;196(2):E 29-E 46. doi:10.1503/cmaj.230542 38253366 PMC 10805138 · doi ↗ · pubmed ↗
- 5Schofield D, Kelly S, Shrestha R, Callander E, Passey M, Percival R. The impact of back problems on retirement wealth. Pain. 2012;153(1):203-210. doi:10.1016/j.pain.2011.10.018 22192565 · doi ↗ · pubmed ↗
- 6Schofield D, Cunich MM, Shrestha RN, . The indirect costs of back problems (dorsopathies) in Australians aged 45 to 64 years from 2015 to 2030: results from a microsimulation model, Health&Wealth MOD 2030. Pain. 2016;157(12):2816-2825. doi:10.1097/j.pain.0000000000000715 27842049 · doi ↗ · pubmed ↗
- 7da Cunha Menezes Costa L, Koes BW, Pransky G, Borkan J, Maher CG, Smeets RJEM. Primary care research priorities in low back pain: an update. Spine (Phila Pa 1976). 2013;38(2):148-156. doi:10.1097/BRS.0b 013e 318267 a 92f 22781003 · doi ↗ · pubmed ↗
- 8Pransky G, Borkan JM, Young AE, Cherkin DC. Are we making progress?: the tenth international forum for primary care research on low back pain. Spine (Phila Pa 1976). 2011;36(19):1608-1614. doi:10.1097/BRS.0b 013e 3181 f 6114 e 21245787 · doi ↗ · pubmed ↗