Socioeconomic disparities and dog rabies: a retrospective analysis of high-spatial-resolution surveillance data from a Latin American city
Sherrie Xie, Julianna Shinnick, Elvis W. Diaz, Edith Zegarra, Ynes Monroy, Sergio E. Recuenco, Ricardo Castillo-Neyra

TL;DR
This study finds that rabies in dogs is more common in poorer areas of a Peruvian city and suggests combining targeted and community-based surveillance to reduce disparities.
Contribution
The study provides empirical evidence linking socioeconomic disadvantage to higher dog rabies incidence within a single city using high-resolution surveillance data.
Findings
Rabies cases were concentrated in socioeconomically disadvantaged blocks (p < 0.001).
Sample positivity was positively associated with neighborhood disadvantage (p < 0.05).
Active surveillance reduced disparities in surveillance effort and sample positivity.
Abstract
Dog-mediated human rabies is intuitively linked to poverty, but few studies have formally investigated the relationship between local socioeconomic disadvantage and dog rabies incidence. We leveraged a unique, high-spatial-resolution surveillance database from the rabies-endemic city of Arequipa, Peru to probe the relationship between neighbourhood socioeconomic status (SES) and dog rabies risk in 2015–2022. Rabies cases and samples were assigned to the SES level of their block or locality of origin, respectively. We tested the hypothesis that lower SES is associated with increased case positivity and used a spatial statistical model to understand how sample positivity varied spatially. Rabies cases were concentrated in socioeconomically disadvantaged blocks (p < 0.001), and sample positivity had a significant and positive association with neighbourhood disadvantage (p < 0.05 for all…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
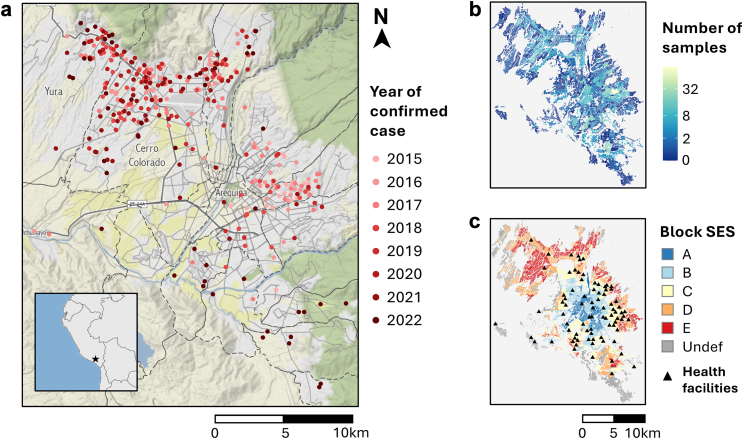 Figure 1
Figure 1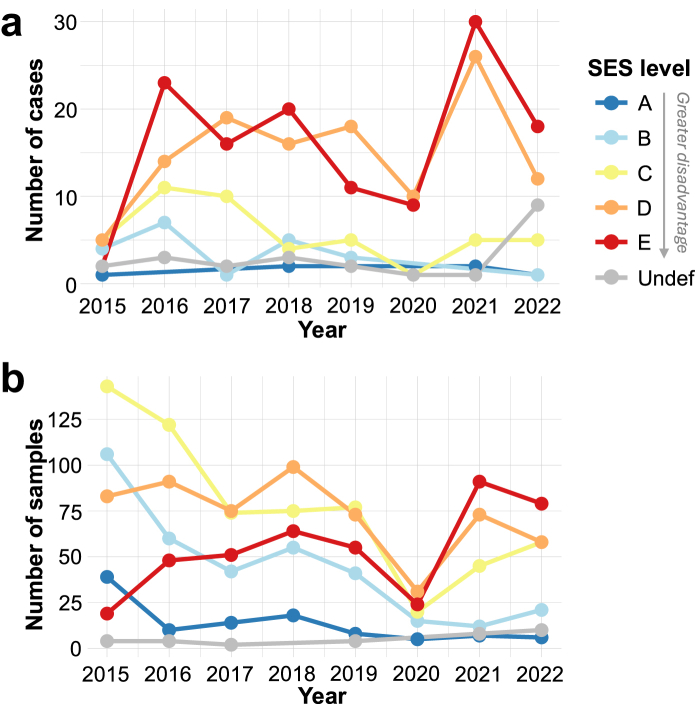 Figure 2
Figure 2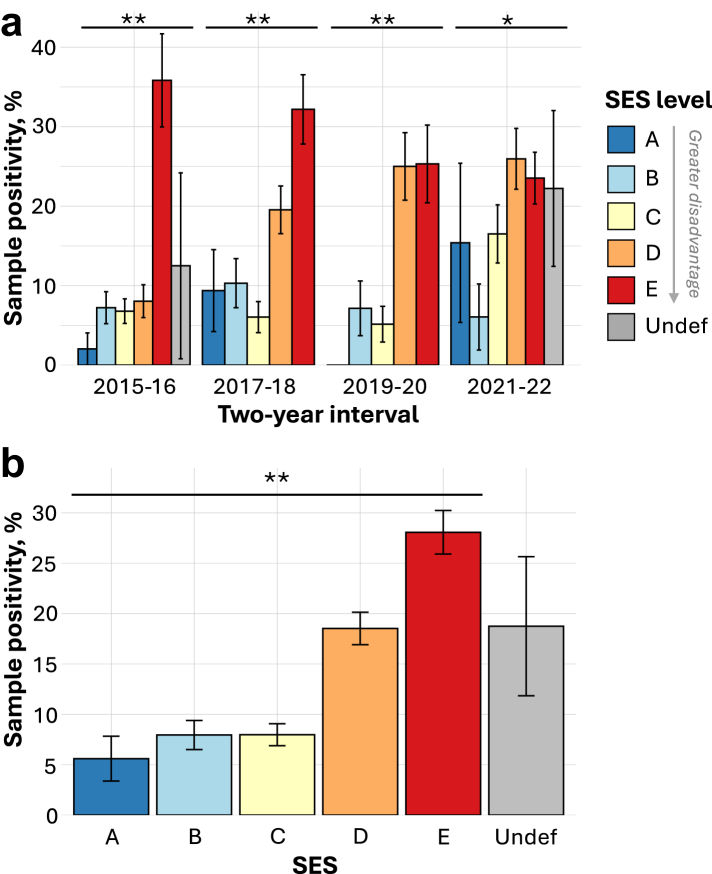 Figure 3
Figure 3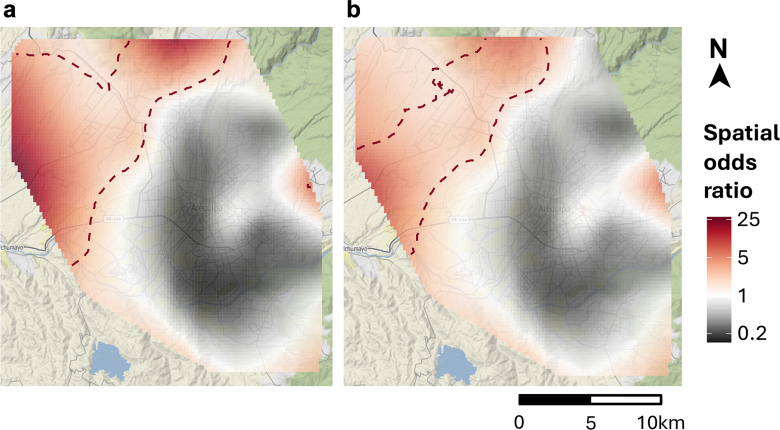 Figure 4
Figure 4- —10.13039/100000002National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRabies epidemiology and control · Geographies of human-animal interactions · Zoonotic diseases and public health
Research in contextEvidence before this studyAlthough dog-mediated human rabies is commonly linked to poverty, few studies have formally investigated the relationship between local socioeconomic disadvantage and dog-mediated rabies risk. We conducted a comprehensive search in PubMed, Web of Science, and Google Scholar for published studies evaluating the relationship between area-based socioeconomic status (SES) measures and dog rabies that were published before October 1, 2024. We used the search terms “rabies”, “dog rabies”, “socioeconomic status”, “poverty”, “spatial analysis”, and “spatiotemporal analysis”. Only two studies met the criterion of assessing the relationship between area SES and dog rabies. These studies yielded inconsistent results, with one finding a higher rate of dog rabies in poor areas and the other finding the opposite. These analyses, both conducted at the national scale, were limited by the use of coarse spatial data aggregated at the level of districts or municipalities and the sole reliance on case data at the exclusion of negative samples.Added value of this studyOur study leverages a unique high-spatial-resolution surveillance database from a dog rabies-endemic city to assess for trends between dog rabies incidence and neighborhood SES on a local scale (i.e., within a single city's limits). Additionally, we incorporated information from negative samples to infer differences in surveillance effort across space and socioeconomic divides. We found that the concentration of rabies cases and sample positivity rates were highest in socioeconomically disadvantaged neighborhoods. As sample positivity provides insight into both case incidence and surveillance effort, the disparity in this metric also suggests that surveillance effort has been insufficient in disadvantaged areas of the city. Stratifying samples by those collected via active surveillance vs. passive surveillance revealed that active surveillance reduced disparities in surveillance effort and sample positivity.Implications of all the available evidenceGlobal trends in rabies disparities are also evident on a local scale in urban centers. Disadvantaged neighborhoods are disproportionately affected by dog rabies and should be prioritized to reduce health inequities and support rabies elimination. Our findings also provide evidence for the use of targeted active surveillance to mitigate disparities arising from population-based passive surveillance systems. Reducing local inequities in dog rabies control will be essential for achieving WHO's goal of eliminating dog-mediated human rabies by 2030.
Introduction
Dog-mediated rabies is a neglected zoonotic disease that causes tens of thousands of human deaths annually.1^,^2 An acute encephalitis caused by a lyssavirus, rabies is 100% fatal once symptoms appear.3 It disproportionately affects low and middle-income countries (LMICs), which carry 99% of the global burden of the disease.2^,^4 The vast majority (99%) of human rabies cases are transmitted through dog bites, with most dog-mediated human rabies cases occurring in Southeast Asia and Sub-Saharan Africa.3^,^5 However, dog rabies remains endemic in parts of the Americas, including Haiti, Guatemala, Bolivia, and southern Peru where ongoing transmission of rabies virus in dog populations leads to regular spillover into humans.6, 7, 8
Dog-mediated human rabies mortality is commonly linked to poverty,9, 10, 11 partly due to limited access to rabies post-exposure prophylaxis (PEP) by under-resourced communities.10 At the cost of USD 65-108 per treatment, PEP has been unaffordable for health systems and communities in many LMICs,12 although recent investment from Gavi, the Vaccine Alliance, may help bridge this gap.13 Even if PEP is available to healthcare systems, it may be inaccessible to people who have experienced dog bites due to lack of availability at nearby health centers,14^,^15 lack of knowledge or misconceptions about PEP as a treatment option,16 or distance to health centers.17 Additionally, studies conducted in LMICs have found that individuals from low socioeconomic backgrounds are less knowledgeable about rabies and prevention practices, less likely to vaccinate their dogs against rabies, and less likely to seek medical care after a dog bite.18, 19, 20, 21, 22, 23, 24, 25, 26
In addition to disparities in healthcare access and knowledge of prevention practices, disparities in dog rabies incidence and surveillance may also drive the association between dog-mediated human rabies and poverty. However, studies investigating the relationship between area-level socioeconomic status (SES) and dog rabies incidence have yielded inconsistent results. A spatial analysis of dog rabies in Thailand revealed that more cases occurred in high-poverty areas.27 However, a study conducted with data from El Salvador contradicted these findings; the study's authors concluded that dog rabies risk was higher in the country's low-poverty zones.28 Limitations of both these prior studies include: (1) the use of case data only and a lack of negative samples to provide information about spatial variation in surveillance effort and (2) the use of relatively low-resolution spatial data (i.e., rabies incidence and SES aggregated at the level of districts or municipalities, each comprising an average 20,000–80,000 people).
Here, we leverage a unique high-spatial-resolution surveillance dataset from Arequipa, Peru to understand the relationship between neighbourhood SES and dog-mediated rabies risk. Dog rabies has become endemic in Arequipa a few years after the region was declared rabies free, a result of viral reintroduction into the local dog population that was first detected in 2015.29 Annual mass dog vaccination campaigns have been held since 2015 to combat the epidemic; however, reaching adequate herd immunity has remained a challenge (estimated coverage <70% in most areas) due to local resource constraints and various barriers to participation faced by dog owners.30, 31, 32, 33
There are a few features of the dog rabies epidemic in Arequipa that are distinct from those in other parts of the world. First, like in much of the Americas, rabies surveillance, outbreak response, dog vaccination, and dog bite case management are activities managed by the local Ministry of Health (MoH), a separate entity from government veterinary services that typically focus on livestock diseases. Additionally, because Arequipa is surrounded by desert with little wildlife to act as viral reservoirs, rabies transmission is sustained by the local dog population with rare spillover into cats and humans; there have been no rabies detected in livestock or wildlife to date.
There is marked socioeconomic inequality in Arequipa, as in many Latin American cities, and we aimed in the present study to determine how the risk posed by dog rabies differentially impacts residents across space and socioeconomic divides. To evaluate the presence of social and spatial inequality in dog rabies burden and surveillance, we test the hypothesis that positivity rates of samples submitted for dog rabies testing increase with low neighborhood SES (i.e., neighborhood disadvantage), map the geospatial distribution of sample positivity, and assess for the presence of positivity hotspots using spatial statistics.
Methods
Data sources
There is a passive surveillance system for dog rabies in Arequipa, Peru, in which dead or suspected dogs are reported by residents to the local MoH either by phone or in-person notification at health facilities (municipal hospitals, health centers, and health posts; Fig. 1). Following notification and typically (>90%) within two days of the report date, MoH personnel investigate and collect brain samples from suspected cases for testing by the direct fluorescent antibody test, which is performed using a standardized protocol for rabies diagnosis that is in accordance with WHO guidelines.34 Briefly, the brains of dead or euthanized dogs are removed and processed into tissue impressions that are fixed on a slide and stained with fluorescently labeled anti-rabies antibodies; then a fluorescence microscope is used to detect rabies viral antigens. Beginning in 2021, the Zoonotic Disease Research Center (a consortium between the University of Pennsylvania and Cayetano Heredia University) has supplemented the passive surveillance system with active surveillance, whereby field personnel search the city's dry water channels for dead dogs and submit samples from all recovered dogs for rabies testing using the protocol described above. Dry water channels are targeted by active surveillance because they are frequently utilized as an ecological corridor by the city's free-roaming dogs and have been previously associated with the locations of rabid dogs.29^,^35 Precise longitudinal and latitude coordinates are recorded for all confirmed cases, and the locality (subdistrict division containing 984 people on average) in which a reported dog was found is recorded for samples submitted for testing. We limited our analyses to dog samples collected between January 1, 2015 and December 31, 2022.Fig. 1Maps depicting the confirmed cases of canine rabies (a), surveillance effort by locality (b), and block-level socioeconomic status (c). Panel a shows the locations of confirmed cases of canine rabies as dots colored according to year. Case locations were slightly jittered to protect the privacy of positive households. District boundaries are indicated by dashed lines, and the districts of Yura and Cerro Colorado are labelled. The inset map in panel a shows the location of Arequipa in Peru. Panel b maps the number of samples submitted for laboratory testing for canine rabies in 2015–2022 for each locality of Arequipa, and the colour scale was log (x+1) transformed. Panel c depicts the geographic distribution of block-level socioeconomic status (SES) in Arequipa and the locations of health facilities (black triangles). Block-level SES is an ordinal variable, with group A comprising the most affluent blocks and group E comprising the most disadvantaged blocks. Blocks whose SES level was undefined (“Undef”) are colored gray. Note that the spatial extent of all three map panels is the same.
A large geospatial database of all households in Arequipa is maintained by the Zoonotic Disease Research Center that contains for each residential block either: (1) the coordinates of all houses on the block or (2) a block-level aggregate house count. The Peruvian National Institute of Statistics and Informatics (INEI for the acronym in Spanish) determines block-level SES through a national household economic survey that is further imputed using information from the national census using a small-area SES estimation method developed by the World Bank.36^,^37 Block-level SES is calculated based on average estimated household income and further stratified as an ordinal variable using the Dalenius-Hodges method, taking values A, B, C, D, E, or NA.36^,^38 A represents the highest (least disadvantaged) SES level and E represents the lowest (most disadvantaged) level. Blocks with insufficient data to determine SES are classified as NA; notably, NA assignment often occurs in newly developing, peri-urban areas where households are typically more materially disadvantaged than those in more established areas.39 To distinguish the NA classification from true missing data, we will refer to this level as undefined for the remainder of this manuscript.
Assigning SES levels to confirmed rabies cases and surveillance samples
Rabies cases were assigned SES levels by intersecting case coordinates with city block polygons and assigning cases to the SES level of the block they fell in. Case coordinates that fell outside of block polygons but within 50 m of a city block were assigned the SES level of their closest block. Fifty meters was chosen as the distance threshold as it represented the distance within which case coordinates could be clearly associated with a residential area. Case coordinates located more than 50 m from a city block were not assigned an SES level and were excluded from further analyses. Localities that contained a median of 13 blocks (interquartile range = 7–26), were assigned the median SES level of the blocks within them (after excluding blocks with undefined SES), except for localities in which the majority (>50%) of blocks had undefined SES, which were assigned the undefined SES level. All spatial data manipulations were performed in R using the sf package.40, 41, 42 Maps of confirmed case locations, locality-level sample counts, and block-level SES were generated using the ggmap R package.43
Evaluating the relationship between sample positivity and neighborhood SES
Sample positivity—which is calculated by dividing the number of confirmed cases for a group or location by the number of samples submitted for that group or location—served as the primary measure by which we evaluated dog rabies disparities, because it combines the burden posed by dog rabies incidence (via confirmed cases) and surveillance effort (via submitted samples). To test the hypothesis that sample positivity increased with neighborhood disadvantage, we performed two-sided Cochran–Armitage trend tests, which can be used to assess for the presence of a trend in the binomial proportions of an outcome variable (sample positivity) across the levels of an ordinal exposure variable (neighborhood SES).
To evaluate the consistency of trends over time, we applied the Cochran–Armitage test to samples stratified across two-year intervals: 2015–2016, 2017–2018, etc. Two-year intervals were chosen to capture any broad temporal changes without resulting in overly small cell sizes. We also applied the test across all years to assess for a global trend. We performed the tests by excluding samples assigned to the undefined SES level. As a sensitivity analysis, we also conducted the tests by re-assigning undefined samples to SES level E, as households located in these newly developing areas in the city periphery tend to be the most materially disadvantaged.39
We also tested for disparities in the total case count by comparing the counts of cases found in disadvantaged blocks (i.e., SES levels D or E) and less disadvantaged blocks (i.e., SES levels A, B, or C) to the counts of households within the city that fall within these same SES groups using a chi-squared test with one degree of freedom while excluding cases and households in the undefined SES level. We used a binary classification system (i.e., SES levels D/E vs. SES levels A/B/C) to assess disparities, as our aim was to determine whether cases tended to occur in disadvantaged vs. less disadvantaged areas and not whether the specific SES distribution of cases (number in SES levels A vs. B vs. C…) differed from that of households in the city. As a sensitivity analysis, we included cases and households in the undefined level, grouping them with SES levels D and E. All statistical analyses were performed in R version 4.2.1.40 The Cochran–Armitage trend tests were performed using the CochranArmitageTest function in the DescTools package, and chi-squared tests were performed using the chisq.test function in the base stats package.40^,^44
Assessing the impact of active surveillance on observed disparities
To understand how the supplemental active surveillance activities that began in 2021 impacted rabies disparities, we assessed the SES distributions of samples obtained via active vs. passive surveillance in 2021 and 2022 and tested for differences using chi-squared tests. We compared plots of the temporal trends in the number of cases and submitted samples by SES from the main results to similar plots that excluded samples obtained via active surveillance. We repeated our analysis of the trend between sample positivity and neighborhood SES but excluding samples obtained via active surveillance. We repeated the two-sided Cochran–Armitage test excluding active samples for the 2021–2022 period (the only period with active surveillance) as well as the entire study period and compared these results to the main results that were calculated using all (both active and passive) samples.
Spatial analysis of sample positivity
We used a generalized additive model (GAM) to determine how sample positivity varied spatially and assess for the presence of global spatial heterogeneity and local hotspots of sample positivity. Spatial analysis using GAM has been described previously,45^,^46 but in brief, the GAM was used to generate an odds ratio map of sample positivity across Arequipa. A global test was performed to test for overall spatial heterogeneity with an alpha of 0.05, and given a significant global test, a local test for significance was performed to identify areas (hotspots) with higher sample positivity using a one-sided alpha of 0.01. We considered both a crude GAM without covariate adjustment and a GAM that included adjustment for locality-level SES and distance between the locality centroid of the sample of origin and the nearest health facility. We used Moran's I to ensure there was not spatial autocorrelation in the model residuals of the crude and adjusted GAMs, using an alpha level of 0.05 to determine significance. Spatial GAM analyses were performed using R package MapGAM,40^,^47 and risk maps generated from model outputs were created using R package ggmap.43 Moran's I of the model residuals were calculated using the Moran.I function in R package ape.48
Multivariable logistic regression modeling of sample positivity
To assess the sensitivity of our findings to our analytical approach, we also instituted a statistical model to identify factors associated with sample positivity. We used a stepwise modeling approach and considered each factor sequentially, incorporating a factor into subsequent models only if it was significantly associated with sample positivity in prior models, as determined using an alpha level of 0.05. We constructed four logistic regression models to consider the effects of locality SES, distance to the nearest health facility, distance to dry water channels, and active (vs. passive) surveillance. Model 1 considered locality SES as the only explanatory variable; Model 2 considered distance to the nearest health facility and only included locality SES if it were significantly associated with sample positivity in Model 1; Model 3 considered distance to dry water channels and only included locality SES and health facility distance if they were significant predictors of sample positivity in Models 1 and 2 and so on. Distance metrics were treated as continuous variables, active surveillance was treated as a binary variable, and locality SES was treated as a categorical variable to avoid imposing a dose–response relationship between neighbourhood disadvantage and sample positivity.
Role of the funding source
Research reported in this publication was supported by NIH-National Institute of Allergy and Infectious Diseases grants K01AI139284 (R. Castillo-Neyra), R01AI168291 (R. Castillo-Neyra), and NIH-Fogarty International Center grant D43TW012741 (R. Castillo-Neyra, E.W. Díaz). The Centers for Disease Control and Prevention, through the Award 75D30120P08488, supported the active surveillance activities conducted in 2020. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Results
Rabies cases and samples
There were 347 confirmed cases of dog rabies in 2015–2022 (Fig. 1a). Of these 347 cases, only two cases (0.6%) were located >50 m from the closest city block and were thus excluded from further analyses. Of the remaining 345 cases, 203 (59%) were located inside a city block, while 142 (41%) fell within 0.1–46 m of the closest city block. Six (2%) were assigned to SES level A, 21 (6%) to level B, 46 (13%) to level C, 120 (35%) to level D, 129 (37%) to level E, and 23 (7%) to level undefined. Compared to the SES distribution of households in the city, cases were disproportionately concentrated in disadvantaged city blocks, i.e., SES levels D and E (p < 0.0001; Supplementary Figure S1 and Supplementary Table S1). These results were unchanged when undefined cases and households were included in the analysis grouped with SES levels D and E (p < 0.0001).
In the same eight-year span, there were 2568 samples submitted for laboratory testing of rabies virus in Arequipa. Of these, 2119 (83%) samples could be matched to a locality of origin; the 449 (17%) samples missing locality information were excluded from further analyses. All samples excluded due to missing locality information were negative. Of the 2119 samples that could be matched to a locality of origin, 107 (5%) originated from localities in the highest SES level (A), 352 (17%) were from localities in level B, 614 (29%) were from localities in level C, 583 (28%) were from localities in level D, 431 (20%) were from localities in level E, and 32 (2%) were from localities in the undefined SES level.
Temporal trends and sample positivity
During the initial years of the epidemic, rabies cases were typically detected just east of the city center; however, cases have increasingly extended into the northwestern and southern periphery in recent years (Fig. 1a). Surveillance effort has been spatially heterogeneous, with greater sample submission volumes in localities closer to the city center, particularly in the east and south (Fig. 1b). Health facilities in Arequipa are concentrated in the more affluent neighborhoods located in or near the city center (Fig. 1c). Although many recent cases have been detected in the disadvantaged peri-urban region of the northwest, sample volume has been relatively low in that area, which also has a reduced number of health facilities (Fig. 1a–c).
Since the second year of the epidemic (2016), there has been a clear and sustained disparity in the number of confirmed rabies cases in which annual case counts have been highest in the most disadvantaged areas (D and E; Fig. 2a). Surveillance effort–which was highest at the beginning of the epidemic and dipped in 2020 during the first year of the COVID-19 pandemic–shows a somewhat different temporal trend; annual sample counts were initially highest in localities with intermediate SES, but submissions from disadvantaged localities have made up a greater share of annual surveillance effort over time (Fig. 2b).Fig. 2Temporal trends in the number of confirmed cases (a) and submitted samples (b) by socioeconomic status. Lines are colored according to the socioeconomic (SES) level assigned to the case or sample of origin, where cases were assigned to SES at the block level, and samples were assigned to SES at the locality level. SES is an ordinal variable ranging A-E, with E denoting the most disadvantaged level.
Sample positivity increased with neighborhood deprivation, and this trend was highly significant across all periods considered (p < 0.0001 across all years and for each two-year interval except for 2021–2022, which had p = 0.024; Fig. 3). The inclusion of undefined blocks (reassigned to level E) did not change the significance of the association for all periods considered (p = 0.025 for 2021–22 and p < 0.0001 for all other periods). The period with the weakest trend between sample positivity and neighborhood SES (2021–2022) coincided with supplemental active surveillance activities. In the next section, we discuss how these activities may have impacted observed trends.Fig. 3Sample positivity by socioeconomic status (SES) level for canine rabies samples plotted for two-year intervals (a) and across all years (b). Bars are plotted with their margins of error and shaded according to the SES level associated with the sample of origin. SES is an ordinal variable ranging A-E, with E denoting the most disadvantaged level. There were <5 samples from undefined blocks in 2017–18 and 2019–20, and these bars were not plotted, as they had very large margins of error. The results of Cochran–Armitage trend tests for a positive association between sample positivity and neighborhood disadvantage (SES A → E) are indicated by asterisks: ∗∗ denotes p < 0.001 and ∗ denotes p < 0.05.
Impacts of active surveillance on SES disparities
Of the 2119 samples submitted for rabies testing, 153 were obtained via supplemental active surveillance in 2021–2022 (Supplementary Table S2). There were 146 and 169 passive samples submitted in 2021 and 2022, respectively, compared to 90 and 63 active samples submitted in those same years (Supplementary Table S2). Active surveillance targeted dry water channels, a strategy informed by eco-epidemiological data suggesting that these landscape features may act as a conduit for rabies transmission among the local dog population.29^,^35 While active surveillance was not intentionally aimed at socioeconomically disadvantaged areas, dry water channels are more concentrated in disadvantaged areas, and samples collected from active surveillance activities were more likely to be from disadvantaged localities (i.e., those assigned to SES levels D, E, or undefined) compared to samples submitted via passive surveillance (p = 0.017 and 0.009 for 2021 and 2022, respectively). While samples from disadvantaged localities accounted for 67% (98 out of 146) and 58% (98 out of 169) of passive samples in 2021 and 2022, respectively, they accounted for 81% (74 out of 90) and 78% (49 out of 63) of active samples during the same years (Supplementary Figure S2). Only a small number of positive samples were collected via active surveillance (5 positives out of 153 active samples compared to 105 of 315 passive samples), and the inclusion of actively collected samples had minimal impact on temporal trends in case numbers across SES levels (compare Fig. 2a to Supplementary Figure S3a). However, the inclusion of samples collected via active surveillance markedly increased the surveillance effort in the most disadvantaged neighborhoods (compare Fig. 2b to Supplementary Figure S3b).
Compared to all 468 samples submitted in 2021–2022 (both active and passive), the 315 passive samples submitted in this time period have more striking disparities in sample positivity (p < 0.0001 compared to p = 0.012 for all 2021–2022 samples; Supplementary Figure S4a). These trends were also apparent across all years: sample positivity in high and intermediate SES groups was unchanged when comparing all samples to passive samples only, but sample positivity was higher in low SES groups when active samples were excluded (compare Fig. 3b to Supplementary Figure S4b). These results indicate that active surveillance contributed a greater share of samples from disadvantaged localities compared to passive surveillance and reduced disparities in both surveillance effort and sample positivity.
Spatial analysis results
Spatial modeling using GAM revealed that sample positivity varied across Arequipa (global test p < 0.001; Fig. 4). Local one-sided significance tests, used to identify areas where the odds of samples testing positive were significantly higher than the overall mean, detected a hotspot of sample positivity in the northwest comprising Cerro Colorado and Yura districts (p < 0.01; Fig. 4). This area is marked by socioeconomic disadvantage and low access to health facilities (Fig. 1c). Adjusting for SES and distance from the locality centroid to the closest health facility reduced the intensity and size of the hotspot, though it persisted in the adjusted model (Fig. 4b). There was no evidence of spatial autocorrelation in the model residuals (p > 0.05 for both the crude and adjusted GAMs), which suggests that the GAMs appropriately captured the spatial variation in sample positivity for the study area (Supplementary Table S3).Fig. 4The spatial risk of sample positivity before (a) and after (b) covariate adjustment for neighbourhood socioeconomic status and distance to the nearest health facility. Raster cells are colored according to the spatial odds ratio of sample positivity, with red denoting areas of increased risk. Statistically significant hotspots (p < 0.01) of sample positivity are demarcated by red, dotted lines.
Factors associated with sample positivity
The results of the multivariable logistic regression models that evaluated the relationships between sample positivity and locality SES, distance to health centers, distance to water channels, and active (vs. passive) surveillance are shown in Supplementary Table S4. In all models, locality-level disadvantage was strongly and positively associated with sample positivity. For example, in the fully adjusted model (Model 4), samples collected in localities with SES levels C, D and E had 1.7 (CI95 0.8, 4.5), 3.7 (CI95 1.7, 9.8), and 5.7 (CI95 2.6, 15.1) greater odds of being positive compared to those collected in localities with SES level A. Distance to health facilities was another independent predictor of sample positivity, as samples collected further from health facilities were more likely to be positive. There was no association between sample positivity and distance to water channels (Supplementary Table S4).
Discussion
While dog-mediated rabies is commonly linked to poverty, few studies have investigated how dog rabies incidence varies with neighbourhood SES. Our analysis revealed clear socioeconomic disparities in dog rabies burden in Arequipa, Peru: confirmed cases and sample positivity rates were highest in disadvantaged neighborhoods. Additionally, our spatial analysis identified a sample positivity hotspot in the peri-urban region located northwest of the city center, which could be explained, in part, by the disadvantage and low access to health facilities in that area. As sample positivity provides insight into both case incidence and surveillance effort, the disparities in this metric also suggest that surveillance effort has been insufficient in disadvantaged areas of the city. Encouragingly, our results also indicate that spatially-targeted active surveillance can be combined with population-based passive surveillance to mitigate disparities in surveillance effort and sample positivity.
Our study adds to the evidence that the risk of dog-mediated rabies is disproportionately higher in the most disadvantaged areas of Arequipa. Previous studies of dog-mediated rabies risk in the city have found much higher rates of dog bites in the city's peri-urban areas.17 Once bitten, the percentage of people who received medical care, including PEP, in the city's wealthier urban areas was almost twice as high compared to those living in the city's peri-urban areas.17 Indeed, the first, and so far, only, documented human fatality due to rabies in the region occurred in Chiguata, a peri-urban area east of the city center.49 The low access and utilization of health services in disadvantaged peri-urban areas likely contributes to the underdetection of human cases. Studies assessing local knowledge, attitude, and practices towards rabies conducted in other LMICs have found socioeconomic disadvantage to be associated with less knowledge about rabies preventative practices and treatment,18, 19, 20, 21, 22, 23, 24, 25 a mechanism by which socioeconomic disadvantage may also act as a social determinant of human rabies in Arequipa and other highly unequal Latin American countries.
Canine rabies incidence is higher in Arequipa's disadvantaged neighborhoods due to several factors. Although vaccination coverage is similar across SES levels, peri-urban areas have more free-roaming dogs, which experience higher contact rates and population turnover, reducing effective vaccination coverage.50 The greater concentration of free-roaming dogs in peri-urban areas is partly due to inadequate waste management policies and budgets compared to urban areas, resulting in greater accumulations of solid waste, an important resource for free-roaming dogs.51 Arequipa's dry water channels have been shown to allow free-roaming dogs to travel long distances, increasing transmission potential.35 These water channels have more access points in the peri-urban areas compared to urban central areas. Additionally, peri-urban dogs are often bred as guard dogs, leading to more aggressive behaviour over time.30
The disparity in sample positivity and the lesser relative surveillance effort in disadvantaged areas can be explained by a variety of factors. First, the passive surveillance system requires that residents report dead or suspected dogs to nearby health facilities. However, disadvantaged, peri-urban parts of the city have relatively low access to health facilities, making reporting more challenging in these areas. In fact, the hot spot of sample positivity we detected was located in the city's northwestern peri-urban periphery. Our analysis also revealed that this same area has the lowest density of health facilities, and the adjusted spatial GAM model indicated that distance to health facilities could explain some of the increased positivity in that area. In previous work, distance to health facilities has been associated with other rabies outcomes, including decreased PEP uptake and greater number of deaths due to rabies.17^,^24^,^52 In addition to decreased health access, those living in peri-urban areas more frequently work in informal jobs that preclude them from going to health posts to report suspicious dogs. Our findings are in line with previous work suggesting evidence of under-reporting of dog bites in peri-urban areas (a related kind of surveillance).17 Finally, reporting of suspicious dogs requires that residents be informed about rabies, and knowledge of rabies may be lower in disadvantaged, peri-urban areas.
Currently, rabies surveillance, outbreak response, dog vaccination, and dog bite case management are activities managed by the local MoH in Arequipa. Veterinarians outside of the MoH (i.e., those working in municipal centers or private clinics) play a limited role in rabies control and surveillance. Private veterinarians occasionally report rabid dogs (only about 20 during the study period, making up a minority of total cases). Municipal veterinary services currently include deworming and health exams for local dogs, but their activities are rarely coordinated with the MoH and do not include responding to suspected cases. Coordinating rabies control and surveillance activities between the MoH and municipal and private veterinarians would strengthen the city's response to the ongoing epidemic.
Our study is subject to some limitations. First, our analyses utilized data from a predominantly passive surveillance system, which is subject to reporting bias, including differential reporting by SES (as health service access and knowledge of rabies is likely lower in disadvantaged areas). However, as explained below, including negative samples allowed us to account for differential surveillance effort. Other limitations include the 17.5% of samples that were excluded from our analysis due to missing locality information and the potential for SES misclassification resulting from changes in neighborhood environment (e.g., gentrification) during the study period. Additionally, the locations of negative samples were only available at the locality level, which may have resulted in some misclassification of sample SES. However, due to the high spatial correlation of block-level SES, there was good agreement between block- and locality-level SES (Cohen's k = 0.834), suggesting that misclassification was low. Finally, using locality centroids to represent the locations of negative samples in the spatial GAM analysis resulted in some inaccuracy in the control locations. However, localities are relatively small geographic units; there are 1317 localities in Arequipa and each contains a median of only 13 city blocks. Thus, the degree of spatial misclassification introduced by using centroids at this level of spatial aggregation likely had minimal impact on our results.
A key strength of our study is the inclusion of both positive and negative samples, allowing us to account for variation in surveillance effort across space and SES. Previous studies relying only on confirmed cases27^,^28 may misidentify high-risk areas, as high case counts often reflect greater surveillance effort. For example, a study in El Salvador reported higher dog rabies incidence in low-poverty areas, likely influenced by underreporting in high-poverty rural regions.28 By combining case incidence with sample positivity, we provide a more nuanced view of rabies disparities. Our finding that disadvantaged areas have both the highest case counts and sample positivity suggests true disparities may be even greater than case data alone indicate. Using high-spatial-resolution data enabled us to examine SES impacts within communities in a single city, unlike prior studies conducted on broader spatial scales.10^,^11^,^27^,^28
In conclusion, we found that global trends in rabies disparities were also evident on a local scale, which highlights a critical health equity issue in a Latin American city. Disadvantaged areas are disproportionately affected by dog rabies and should be prioritized to protect the most vulnerable. By identifying where resources are most needed, our analysis supports a shift from broad city-wide approaches, necessary in some contexts (i.e., city-wide mass dog vaccination), to more targeted surveillance and control strategies that use limited resources efficiently. In addition to reducing inequities, targeting resources to the highest-risk areas would support rabies elimination, as spatial heterogeneity in transmission risk can sustain an epidemic even when herd immunity thresholds have been reached.53^,^54 Importantly, our results advance the goals of One Health by integrating human, animal, and environmental health. By focusing on socioeconomic and geographic inequities, our study emphasizes the need for coordinated efforts across multiple sectors, including healthcare, veterinary services, urban planning, and local stakeholder engagement. Reducing inequities in dog rabies control will be essential for achieving the WHO's goal of eliminating dog-mediated human rabies by 2030.55
Contributors
SX contributed to the conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing the original manuscript, and editing the final manuscript. JS contributed to writing the original manuscript and reviewing and editing the final manuscript. ED, EZ, and YM contributed to the investigation and project administration. SR contributed to writing of the paper and reviewing the final manuscript. RCN contributed to the conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, and writing of the paper.
Data sharing statement
All code and non-sensitive data are available at https://github.com/RabiesLabPeru/ses_rabies.
Editor note
The Lancet Group takes a neutral position with respect to territorial claims in published maps and institutional affiliations.
Declaration of interests
We declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hampson K.Coudeville L.Lembo T.Estimating the global burden of endemic canine rabies P Lo S Negl Trop Dis 942015 e 000370910.1371/journal.pntd.0003709 PMC 440007025881058 · doi ↗ · pubmed ↗
- 2Gan H.Hou X.Wang Y.Global burden of rabies in 204 countries and territories, from 1990 to 2019: results from the global burden of disease study 2019 Int J Infect Dis 12620231361443634386610.1016/j.ijid.2022.10.046 · doi ↗ · pubmed ↗
- 3Scott T.P.Nel L.H.Lyssaviruses and the fatal encephalitic disease rabies Front Immunol 122021[cited 2024 Sept 4] Available from:https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2021.786953/full 10.3389/fimmu.2021.786953 PMC 867859234925368 · doi ↗ · pubmed ↗
- 4Bucher A.Dimov A.Fink G.Chitnis N.Bonfoh B.Zinsstag J.Benefit-cost analysis of coordinated strategies for control of rabies in Africa Nat Commun 141202353703767931410.1038/s 41467-023-41110-2PMC 10484917 · doi ↗ · pubmed ↗
- 5World Health Organization WHO fact sheet on rabies[cited 2024 Nov 13]. Available from:https://www.who.int/news-room/fact-sheets/detail/rabies
- 6Seetahal J.F.R.Vokaty A.Vigilato M.A.N.Rabies in the Caribbean: a situational analysis and historic review Trop Med Infect Dis 332018893027448510.3390/tropicalmed 3030089 PMC 6160905 · doi ↗ · pubmed ↗
- 7Meske M.Fanelli A.Rocha F.Evolution of Rabies in South America and Inter-Species Dynamics (2009–2018)Trop Med Infect Dis 622021983420782210.3390/tropicalmed 6020098 PMC 8293400 · doi ↗ · pubmed ↗
- 8Vigilato M.A.N.Clavijo A.Knobl T.Progress towards eliminating canine rabies: policies and perspectives from Latin America and the Caribbean Philos Trans R Soc Lond B Biol Sci 368162320132012014310.1098/rstb.2012.0143 PMC 372004123798691 · doi ↗ · pubmed ↗