RapidArc dynamic versus RapidArc: A multi anatomical‐site dosimetric evaluation
Aram Rostami, Carole Naim, Renilmon Pottanplackal Sukumaran, Mohammad Usman, Abbass Yousef Mkanna, Alla Fuad Al‐Sabahi, Ahamed Basith, Shelton Chuck, Mojtaba Barzegar, Bevan Orville Peltier, Bassim Aklan, Samaneh Baradaran, Satheesh Prasad Paloor, Rabih Wafiq Hammoud

TL;DR
This study compares two radiation therapy techniques, RapidArc and RapidArc Dynamic, showing that the newer method provides better protection for healthy organs without reducing treatment effectiveness.
Contribution
The study introduces and validates RapidArc Dynamic as a next-generation VMAT technique with improved organ-sparing capabilities.
Findings
RAD achieved significant OAR sparing in breast, prostate, lung SBRT, and head and neck cases.
RAD maintained equivalent target coverage compared to RA across all anatomical sites.
RAD improved dose conformity and reduced doses to critical organs like the heart, rectum, and spinal cord.
Abstract
RapidArc (RA) has advanced VMAT delivery; however, challenges remain in achieving optimal organ‐at‐risk (OAR) sparing in complex cases. RapidArc Dynamic (RAD), a next‐generation Volumetric Modulation Arc Therapy (VMAT) technique, incorporates dynamic collimator rotation, embedded static fields, and a faster optimizer to enhance dose modulation. This study compares dosimetric outcomes between conventional RA and RAD across four anatomical sites. A retrospective analysis was conducted on 40 patients (10 each for breast, lung SBRT, prostate, and head and neck cancers). Each case was initially treated with RA and subsequently replanned using RAD in Eclipse v18.1. Plans were evaluated using dose–volume histograms (DVH), and paired t‐tests assessed differences in target coverage and OAR sparing (p < 0.05). RAD maintained equivalent target coverage compared to RA across all sites.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
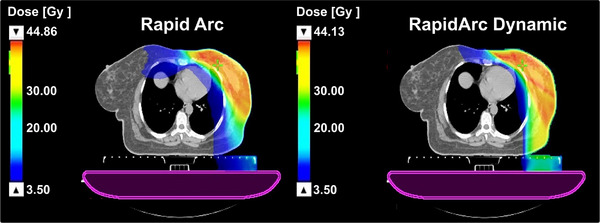 FIGURE 1
FIGURE 1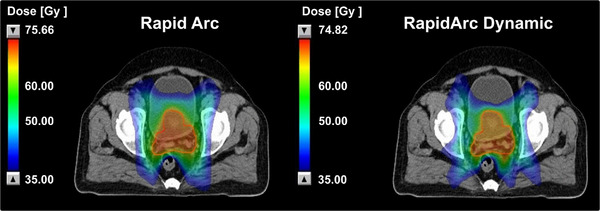 FIGURE 2
FIGURE 2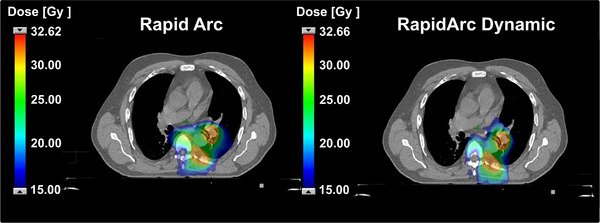 FIGURE 3
FIGURE 3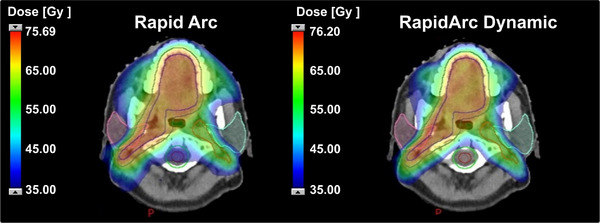 FIGURE 4
FIGURE 4| Parameter | Breast (RAD) | Breast (RA) | Head & Neck (RAD) | Head & Neck (RA) | Prostate (RAD) | Prostate (RA) |
|---|---|---|---|---|---|---|
| Arc span |
305–175 (Left Breast) 55–185 (Right Breast) |
2 Arcs (305–175 and reverse) 2 Arcs (55–185 and reverse) | 1 Full Arc | 2 Full Arcs | 2 Full Arcs | 2 Full Arcs |
| Static fields |
305, 330, 122, 175 (Left) 55, 30, 206, 237 (Right) | N/A | 4 Static Fields per arc | N/A |
2 Static Fields (Arc 1) 2 Static Fields (Arc 2) | N/A |
| Collimator | Optimized | Static | Optimized | Static | Optimized | Static |
| Static and arc weighting | Balanced | N/A | (−1) Arc | N/A | (−1) Arc | N/A |
| Total monitor units (MU) | 912 | 731 | 820 | 710 | 1042 | 910 |
| Estimated planning time | 160 min | 205 min | 150 min | 155 min | 135 min | 142 min |
| Dose calculation algorithm | Acuros XB (V.18.1) | Acuros XB (V.18.1) | Acuros XB (V.18.1) | Acuros XB (V.18.1) | Acuros XB (V.18.1) | Acuros XB (V.18.1) |
| Optimization algorithm | Photon Optimizer (V18.1) |
Photon Optimizer (V18.1) | Photon Optimizer (V18.1) | Photon Optimizer (V18.1) | Photon Optimizer (V18.1) | Photon Optimizer (V18.1) |
| OARs | Dose constraint | Left breast with IMN and SCF | Right breast with IMN and SCF | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RAD (Average) |
RA (Average) | Difference (%) | RAD (Average) |
RA (Average) | Difference (%) | RAD (Average) |
RA (Average) | Difference (%) | ||
| Heart | V23 Gy (%) | 0.14 | 0.17 | −16.48 | 0.14 | 0.18 | −12.50 | 0.139 | 0.173 | −19.47 |
| Heart | Dmean (Gy) | 2.668 | 3.518 | −24.17 | 1.940 | 2.681 | −26.51 | 2.319 | 3.099 | −25.18 |
| Breast contralateral | Dmean (Gy) | 2.048 | 2.752 | −25.58 | 2.176 | 2.721 | −20.02 | 2.112 | 2.736 | −22.82 |
| Lung ipsilateral | Dmean (Gy) | 10.056 | 10.597 | −5.11 | 9.328 | 10.09 | −7.61 | 9.692 | 10.347 | −6.33 |
| Lung ipsilateral | V18 Gy (%) | 21.12 | 21.32 | −1.0 | 18.82 | 20.10 | −6.37 | 19.97 | 20.71 | −3.57 |
| Lung ipsilateral | V5 Gy (%) | 50.36 | 57.96 | −13.11 | 48.8 | 52.24 | −8.5 | 49.08 | 55.10 | −10.93 |
| Lung contralateral | Dmean (Gy) | 2.088 | 2.587 | −19.29 | 1.652 | 1.912 | −13.58 | 1.870 | 2.249 | −16.86 |
| Spinal cord | Dmax (Gy) | 10.80 | 15.39 | −29.85 | 11.322 | 16.40 | −30.98 | 11.062 | 15.901 | −30.43 |
| Humeral head | Dmax (Gy) | 19.44 | 21.10 | −7.76 | 20.769 | 24.334 | −18.02 | 20.107 | 23.218 | −13.4 |
| OPTV | V95 (%) | 96.82 | 96.58 | 0.25 | 98.56 | 97.94 | 0.63 | 97.69 | 97.26 | 0.44 |
| OPTV | V105 (%) | 10.08 | 7.76 | 29.90 | 10.36 | 10.28 | 0.78 | 10.22 | 9.02 | 13.3 |
| PTV‐SC | V95 (%) | 98.54 | 98.12 | 0.43 | 98.22 | 98.22 | 0.0 | 98.38 | 98.17 | 0.21 |
| PTV‐SC | V105 (%) | 1.73 | 2.06 | −16.52 | 2.24 | 1.99 | 15.2 | 1.483 | 2.03 | −26.9 |
| Endpoint | RAD (Average) | RA (Average) | Δ (%) |
Raw
|
Bonferroni Corrected
| Significant ( | Significant after correction ( |
|---|---|---|---|---|---|---|---|
| Heart Dmean (Gy) | 2.319 | 3.099 | −25.18 | 0.008 | 0.024 | Yes | No |
| Ipsilateral lung V20 Gy (%) | 19.970 | 20.710 | −3.57 | 0.480 | 1.000 | No | No |
| Spinal cord Dmax (Gy) | 11.062 | 15.901 | −30.43 | 0.001 | 0.003 | Yes | Yes |
| Endpoint (Exploratory) | RAD (Average) | RA (Average) | Δ (%) | Raw p‐value | Interpretation |
|---|---|---|---|---|---|
| Heart V23 Gy (%) | 0.139 | 0.173 | −19.47 | 0.390 | No clear difference |
| Contralateral Breast Dmean (Gy) | 2.112 | 2.736 | −22.82 | 0.009 | Directionally favors RAD |
| Ipsilateral Lung Dmean (Gy) | 9.692 | 10.347 | −6.33 | 0.098 | No clear difference |
| Ipsilateral Lung V5 Gy (%) | 49.080 | 55.100 | −10.93 | 0.008 | Directionally favors RAD |
| Contralateral Lung Dmean (Gy) | 1.870 | 2.249 | −16.86 | 0.009 | Directionally favors RAD |
| Humeral Head Dmax (Gy) | 20.107 | 23.218 | −13.40 | 0.230 | No clear difference |
| OPTV V95 (%) | 97.690 | 97.260 | 0.44 | 0.270 | No clear difference |
| OPTV V105 (%) | 10.220 | 9.020 | 13.30 | 0.630 | No clear difference |
| PTV‐SC V95 (%) | 98.380 | 98.170 | 0.21 | 0.250 | No clear difference |
| PTV‐SC V105 (%) | 1.483 | 2.030 | −26.90 | 0.980 | No clear difference |
| Endpoint | Category | RAD (Average) | RA (Average) |
Δ (%) | Raw p‐value | Bonferroni Corrected p‐value (×3) | Significant (α = 0.05) |
Significant After Correction (α = 0.05/3 = 0.0167) | Interpretation |
|---|---|---|---|---|---|---|---|---|---|
| Rectum V45 Gy (%) | Primary | 21.6 | 26.08 | −17.0 | 0.005 | 0.015 | Yes | Yes | Significant reduction with RAD |
| Rectum V55 Gy (%) | Primary | 12.7 | 14.19 | −10.4 | 0.008 | 0.024 | Yes | Trend (> 0.0167) | Reduction trend |
| Bladder V55 Gy (%) | Primary | 12.8 | 14.65 | −12.6 | 0.008 | 0.024 | Yes | Trend (> 0.0167) | Reduction trend |
| Rectum V60 Gy (%) | Exploratory | 8.8 | 10.19 | −13.7 | 0.070 | – | No | – | No difference |
| Rectum D10 cc (Gy) | Exploratory | 50.89 | 54.18 | −6.1 | 0.040 | – | Yes | – | Directionally favors RAD |
| Rectum Dmax (Gy) | Exploratory | 68.09 | 68.62 | −0.8 | 0.180 | – | No | – | No difference |
| Bladder V65 Gy (%) | Exploratory | 7.4 | 8.11 | −8.4 | 0.090 | – | No | – | No difference |
| Bladder Dmax (Gy) | Exploratory | 70.50 | 69.62 | +1.3 | 0.140 | – | No | – | No difference |
| Femoral Head L Dmean (Gy) | Exploratory | 9.46 | 15.95 | −40.7 | 0.002 | – | Yes | – | Favors RAD |
| Femoral Head L Dmax (Gy) | Exploratory | 39.46 | 42.29 | −6.7 | 0.025 | – | Yes | – | Favors RAD |
| Femoral Head R Dmean (Gy) | Exploratory | 9.16 | 15.11 | −41.2 | 0.001 | – | Yes | – | Favors RAD |
| Femoral Head R Dmax (Gy) | Exploratory | 35.49 | 39.54 | −10.2 | 0.043 | – | Yes | – | Favors RAD |
| Bone Marrow V10 Gy (%) | Exploratory | 54.2 | 60.0 | −10.3 | 0.006 | – | Yes | – | Favors RAD |
| Bone Marrow V20 Gy (%) | Exploratory | 41.9 | 45.41 | −7.8 | 0.009 | – | Yes | – | Favors RAD |
| Bone Marrow V40 Gy (%) | Exploratory | 12.1 | 12.2 | −0.5 | 0.9 | – | No | – | No difference |
| Peritoneum V45 Gy (cc) | Exploratory | 83.8 | 91.32 | −8.2 | 0.008 | – | Yes | – | Favors RAD |
| PTV 5040 V95 (%) | Exploratory | 97.9 | 98.81 | −1.0 | 0.120 | – | No | – | Equivalent coverage |
| PTV 6000 V95 (%) | Exploratory | 98.9 | 98.16 | +0.8 | 0.120 | – | No | – | Equivalent coverage |
| PTV 6500 V95 (%) | Exploratory | 99.2 | 97.12 | +2.2 | 0.180 | – | No | – | Equivalent coverage |
| PTV 7000 V95 (%) | Exploratory | 97.9 | 98.22 | −0.4 | 0.290 | – | No | – | Equivalent coverage |
| Endpoint | Category | RAD (Average) |
RA (Average) | Δ (%) |
Raw p‐value |
Bonferroni corrected p‐value(×2) | Significant (α = 0.05) | Significant After Correction (α = 0.05/2 = 0.025) | Interpretation |
|---|---|---|---|---|---|---|---|---|---|
| Conformity Index (CI) | Primary | 0.84 | 0.77 | 8.3 | 0.008 | 0.016 | Yes | Yes | Improved conformity with RAD |
| Spinal Cord Dmax (Gy) | Primary | 9.470 | 13.493 | −29.8 | 0.004 | 0.008 | Yes | Yes | Significant reduction with RAD |
| PTV V95 (%) | Exploratory | 94.2 | 93.8 | 3.1 | 0.81 | – | No | – | Equivalent coverage |
| PTV V98 (%) | Exploratory | 85.8 | 82.5 | 3.8 | 0.075 | – | No | – | Comparable |
| Heart Dmean (Gy) | Exploratory | 1.150 | 2.10 | −45.2 | 0.001 | – | Yes | – | Favors RAD |
| Lung Dmean (Gy) | Exploratory | 4.130 | 5.680 | −27.3 | 0.040 | – | Yes | – | Favors RAD |
| Lung V5 Gy (%) | Exploratory | 22.8 | 27.1 | −15.1 | 0.035 | – | Yes | – | Favors RAD |
| Lung V10 Gy (%) | Exploratory | 15.9 | 19.3 | −17.6 | 0.033 | – | Yes | – | Favors RAD |
| Lung V20 Gy (%) | Exploratory | 7.8 | 9.2 | −15.2 | 0.034 | – | Yes | – | Favors RAD |
| Endpoint | Category | RAD (Average) | RA (Average) | Δ (%) |
Raw p‐value |
Bonferroni Corrected p‐value (×3) | Significant (α = 0.05) |
Significant After Correction (α = 0.05/3 = 0.0167) | Interpretation |
|---|---|---|---|---|---|---|---|---|---|
| Parotid Left Dmean (Gy) | Primary | 24.3 | 26.1 | −9.7 | 0.010 | 0.030 | Yes | Trend (> 0.0167) | Reduction trend |
| Parotid Right Dmean (Gy) | Primary | 23.6 | 26.9 | −14.2 | 0.010 | 0.030 | Yes | Trend (> 0.0167) | Reduction trend |
| Spinal Cord PRV Dmax (Gy) | Primary | 40.5 | 42.0 | −8.6 | 0.020 | 0.060 | Yes | No | Slight reduction |
| Mucosal Constrictors Dmean (Gy) | Exploratory | 39.5 | 42.7 | −9.2 | 0.010 | – | Yes | – | Favors RAD |
| Lips Dmean (Gy) | Exploratory | 20.3 | 26.1 | −23.4 | 0.010 | – | Yes | – | Significant reduction |
| Larynx Dmean (Gy) | Exploratory | 42.6 | 45.9 | −8.2 | 0.020 | – | Yes | – | Favors RAD |
| Esophagus Dmean (Gy) | Exploratory | 22.5 | 27.1 | −18.2 | 0.010 | – | Yes | – | Favors RAD |
| Oral Cavity Dmean (Gy) | Exploratory | 38.6 | 47.2 | −15.1 | 0.010 | – | Yes | – | Favors RAD |
| Brainstem PRV Dmax (Gy) | Exploratory | 57.5 | 60.0 | −4.6 | 0.020 | – | Yes | – | Reduced Dmax |
| Optic Nerves PRV Dmax (Gy) | Exploratory | 51.0 | 51.3 | −0.6 | 0.800 | – | No | – | No difference |
| Optic Chiasm PRV Dmax (Gy) | Exploratory | 52.5 | 54.5 | −5.6 | 0.040 | – | Yes | – | Trend toward reduction |
| Cochlea Left Dmean (Gy) | Exploratory | 33.6 | 39.4 | −14.9 | 0.010 | – | Yes | – | Favors RAD |
| Cochlea Right Dmean (Gy) | Exploratory | 34.5 | 40.4 | −14.8 | 0.010 | – | Yes | – | Favors RAD |
| Lens Left Dmax (Gy) | Exploratory | 7.6 | 9.4 | −20.0 | 0.010 | – | Yes | – | Significant reduction |
| Lens Right Dmax (Gy) | Exploratory | 7.5 | 9.1 | −18.5 | 0.010 | – | Yes | – | Significant reduction |
| Eye Left Dmax (Gy) | Exploratory | 40.5 | 42.5 | −4.7 | >0.05 | – | No | – | No difference |
| Eye Right Dmax (Gy) | Exploratory | 39.5 | 41.4 | −4.6 | >0.05 | – | No | – | No difference |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Breast Cancer Treatment Studies · Radiation Therapy and Dosimetry
INTRODUCTION
1
Volumetric modulated arc therapy (VMAT) has transformed the field of radiation oncology by enabling precise and efficient delivery of radiation doses. Unlike traditional static‐beam intensity‐modulated radiotherapy (IMRT), VMAT delivers radiation continuously as the machine's gantry rotates around the patient, allowing for highly conformal treatment in a shorter time.1 One of the earliest and most widely used VMAT techniques is RapidArc (developed by Varian Medical Systems, Palo Alto, CA), which coordinates changes in multileaf collimator (MLC) positions, gantry speed, and dose rate to shape the dose dynamically during treatment.2 However, in complex clinical situations—such as head and neck tumors or breast cancers with nodal involvement, conventional RapidArc (RA) may struggle to maintain sharp dose gradients or adequately limit low‐dose exposure to surrounding healthy tissues.2, 3 To address these limitations, RapidArc Dynamic (RAD) was introduced as part of newer software (Eclipse v18.1) and LINAC control system upgrades (TrueBeam v4.1+). RAD represents a significant evolution of the original RapidArc technique. Unlike conventional RA, which relies solely on dynamic arcs, RAD integrates multiple advanced delivery strategies within a single plan, including: directional control of IMRT and efficiency of VMAT delivery in a single treatment field, ability to strategically pause the gantry during an arc rotation for enhanced modulation at optimal beam angles and dynamically adjust collimator rotation to improve dose conformity and organ‐at‐risk sparing during delivery.4
In addition to these mechanical enhancements, RAD also features a new, faster optimization algorithm, which reduces planning time while maintaining dosimetric quality. RAD introduces another practical improvement—auto skin flash tools that help ensure adequate coverage of superficial targets, particularly in breast cases. Moreover, the new Photon Optimizer (PO) used in RAD planning offers an additional level of flexibility: within the optimization window, the user can control the relative weighting between static fields and arc components. This includes options such as balanced mode, arc‐dominant, or static field‐dominant settings, allowing further customization of plan modulation based on clinical objectives.4
This hybrid planning and delivery approach using dynamic collimator during arc offers enhanced flexibility in dose modulation and is particularly beneficial for treating anatomically complex or irregular targets—such as concave planning target volumes (PTVs) or tumors located near critical serial organs‐at‐risk (OARs), including the optic nerves and spinal cord.4 Preliminary hypotheses and vendor‐reported data suggest that RAD may provide improved OAR sparing, sharper dose fall‐off, and enhanced PTV coverage and conformity. However, multi‐anatomical‐site dosimetric comparisons remain limited.4
We hypothesized that RAD's added capabilities—particularly dynamic collimator rotation, incorporation of static fields during arc delivery, and built‐in skin flash for breast planning—could result in superior PTV coverage and OAR sparing compared to conventional RA, especially in anatomically complex cases. To evaluate this hypothesis, we conducted a retrospective dosimetric study in which newly generated RAD plans were compared against the clinically delivered RA plans across four anatomical treatment sites (Breast, Lung SBRT, Prostate, and Head & Neck). A systematic dose–volume histogram (DVH)‐based analysis was performed, and paired t‐tests were used to determine the statistical significance of dosimetric differences between the two planning approaches.
MATERIALS AND METHODS
2
Study design and patient selection
2.1
Following institutional review board approval, this retrospective multi‐anatomical‐site dosimetric study was conducted to compare radiation treatment plans generated using RA and RAD techniques. A total of 40 patients were included across four anatomical sites: Breast cancer (with internal mammary node involvement): 10 patients (5 left‐sided, 5 right‐sided), Lung SBRT: 10 patients, Prostate cancer (with nodal involvement): 10 patients and Head and Neck cancer (with nodal involvement): 10 patients.
For HN cases, treatment plans incorporated simultaneous integrated boost (SIB) over 33 fractions, covering three target volumes: high‐risk (70 Gy), medium‐risk (60 Gy), and low‐risk (54 Gy). For OARs, standard institutional dose thresholds were applied uniformly rather than linking constraints to specific SIB dose levels (70/60/54 Gy). Identical constraints and weightings were applied for both RA and RAD optimizations. These constraints were pre‐specified during optimization and applied consistently across all cases. For prostate cases, plans were delivered over 28 fractions, incorporating two or three target levels: a high‐risk volume (70 Gy) covering the prostate and seminal vesicles, a nodal volume (50.4 Gy), and, when indicated, PSMA PET‐positive bone metastases (64.4 Gy). For breast cases, treatments were planned over 15 fractions, including coverage of the supraclavicular and internal mammary node (IMN) PTVs as part of the target volume. This retrospective analysis was conducted using fully anonymized treatment planning data, with no impact on patient care.
Each patient case was initially planned using the RA technique and subsequently replanned using the RAD technique, enabling direct intra‐patient dosimetric comparisons.
Technology and software
2.2
RAD treatment planning was performed using the Eclipse Treatment Planning System (TPS) v18.1 (Varian Medical Systems, Palo Alto, CA), which features RAD capabilities, including dynamic collimator rotation and embedded static beam segments. For all RAD plans, the STAMP weighting parameter was set to −1 (‘Arc’ weighting) on the optimization window of RAD (−2: Arc Dominant, −1: Arc, 0: Balanced, +1: Static, +2: Static Dominant), indicating an arc‐leaning modulation preference during optimization. All static field angles were user‐specific and selected by the planner, based on the principle of choosing gantry angles that provided maximum geometrical view of the target and minimum geometrical view of adjacent critical OARs. All RA plans, originally generated in Eclipse v16.1, were re‐optimized and recalculated in Eclipse v18.1 to ensure consistency with RAD planning for comparative analysis. All dose calculations for RA and RAD were performed using the Acuros XB (AXB) version 18.1 algorithm with heterogeneity correction enabled, employing a calculation grid size of 2.5 mm for all sites, except for Lung SBRT cases, where a finer 1.25 mm grid size was used to improve dose calculation accuracy in small, high‐gradient regions. For all Lung SBRT cases, motion management was performed using 4DCT simulation to account for respiratory motion, and internal target volumes (ITVs) were delineated accordingly. The same CT datasets were used for both RA and RAD planning across all anatomical sites to ensure consistency and minimize setup‐related differences. Treatment delivery was simulated on Varian TrueBeam LINACs (v4.1) equipped with millennium multileaf collimators.
Planning techniques and geometry
2.3
RA plans utilized conventional VMAT delivery with static collimator angles and no static beam segments during arc delivery.
For both RA and RAD plans, maximum MLC leaf speed was restricted to 2.5 cm/s, and jaw tracking was enabled with a maximum jaw speed of 2.5 cm/s. The maximum field width was limited to 15 cm in the X‐direction to respect MLC leaf span constraints. For RAD plans, dynamic collimator rotation was permitted with a maximum rotation speed of 9°/s.
RAD plans incorporated advanced features, including: dynamic collimator rotation during beam‐on, embedded static fields within arcs, enhanced PO algorithm for faster and more effective optimization and automatic skin flash generation for breast cases. Plan geometry details by site are summarized in Table 1.
Plan evaluation metrics
2.4
For both RA and RAD plans, identical optimization objectives and OAR dose constraints were applied, with the same relative weighting factors in the Photon Optimizer. This ensured that observed differences reflected the planning technique rather than differences in optimization priorities
Each plan was done and reviewed by a multidisciplinary team consisting of two senior medical physicists per anatomical site. Evaluation was based on dose volume histogram comparison.
Following plan generation for both RA and RAD, we conducted a paired t‐test (significance: p < 0.05) to compare the target Coverage (the percentage of the target volume receiving 95% of the prescribed dose V95%), OAR Doses (the dose delivered to each OAR, aiming to identify potential reductions in dose exposure) and conformity index (CI) using Paddick formula 5 for SBRT cases. Primary endpoints per site were pre‐specified based on clinical relevance. P‐values for these were adjusted using Holm–Bonferroni; all other comparisons were considered exploratory.
RESULTS
3
Breast
3.1
A comparative analysis of RAD and RA plans for breast cases demonstrated that both techniques achieved comparable dose coverage of the target volumes, with no statistically significant differences in optimized planning target Volume (OPTV) V95 or V105 and supraclavicular planning target volume (PTV‐SC) coverage (see Table 2).
When considering pre‐specified primary endpoints, RAD yielded a significant reduction in the maximum spinal‐cord dose after Bonferroni correction (p = 0.003 < 0.0167). The mean heart dose was also reduced by approximately 25%, with a corrected p = 0.024, representing a strong trend toward significance, while the ipsilateral lung V20 did not differ significantly between techniques (p = 0.48), see Table 3.
Across exploratory endpoints, RAD consistently demonstrated favorable dosimetric trends. Notably, mean doses to the contralateral breast and contralateral lung were reduced by ∼23% and ∼17%, respectively (p = 0.009 for both), and the ipsilateral lung V5 Gy decreased by ∼11% (p = 0.008). These reductions reflect lower low‐dose exposure in RAD plans, particularly in the thoracic region adjacent to the heart and lungs. No statistically meaningful differences were observed for the humeral head, ipsilateral lung V18 Gy, or target‐volume hotspot parameters (OPTV V105%), see Table 4.
Collectively, these results confirm that while target coverage remains equivalent, RAD provides clinically relevant improvements in OAR sparing—especially in lowering spinal‐cord and cardiac exposures—with consistent directional benefits for other thoracic structures. Figure 1 illustrates a representative comparison of the 3.5 Gy isodose distribution between RA and RAD plans for a left‐sided breast case, highlighting improved conformity and reduced low‐dose spillage with RAD.
Comparison of the 3.5 Gy isodose distribution between RapidArc and RapidArc dynamic plans for a left breast case.
Prostate
3.2
The comparison between RAD and RA plans for prostate cancer demonstrated that both techniques achieved comparable target coverage across all PTVs, with no statistically significant differences in V95% for PTV5040, PTV6000, PTV6500, and PTV7000 (p > 0.05; Table 5).
For the pre‐specified primary endpoints, RAD plans achieved a statistically significant reduction in rectal V45 Gy (p = 0.005; Bonferroni‐corrected p = 0.015 < 0.0167). Rectum V55 Gy and Bladder V55 Gy also decreased by ≈10%–13%, showing trends toward significance after correction (corrected p = 0.024), see Table 5.
Across exploratory endpoints, RAD showed consistent dosimetric advantages. Rectum D10 cc decreased by ≈6% (p = 0.040), and although V60 Gy reduction did not reach statistical significance (p = 0.07), the direction favored RAD. Significant sparing was observed for both left and right femoral heads, with >40% reductions in mean dose and ≈7%–10% reductions in maximum dose (p < 0.05). Bone‐marrow sparing was also superior, with statistically significant decreases in V10 Gy (p = 0.006) and V20 Gy (p = 0.009), while V40 Gy remained comparable between techniques. The peritoneal V45 Gy was reduced by ≈8% (p = 0.008), further supporting improved normal‐tissue sparing with RAD, see Table 5.
Overall, RAD maintained equivalent PTV coverage while achieving clinically meaningful reductions in rectal, bladder, femoral‐head, bone‐marrow, and peritoneal doses. These findings indicate lower normal‐tissue doses with RAD for the evaluated structures without compromising target conformity or dose homogeneity. Figure 2 illustrates a representative 35 Gy (50% of prescription) isodose comparison between RA and RAD plans for a typical prostate case.
Comparison of the 35 Gy (50% of prescription) isodose distribution between RapidArc and RapidArc dynamic plans for a prostate case.
Lung SBRT
3.3
The comparison between RapidArc Dynamic (RAD) and conventional RapidArc (RA) plans for lung SBRT demonstrated that both techniques achieved comparable target coverage, with no statistically significant differences in PTV V95% (p = 0.81) or V98% (p = 0.075; Table 6). Although V98% was slightly higher in RAD plans, this difference did not reach statistical significance.
For the primary endpoints, RAD plans achieved a significantly improved Conformity Index (CI) according to the Paddick formula5 (p = 0.008; Bonferroni‐corrected p = 0.016 < 0.025), confirming superior dose conformity around the target. Similarly, the maximum dose to the spinal cord was significantly reduced with RAD (p = 0.004; Bonferroni‐corrected p = 0.008), indicating effective spinal‐cord sparing after multiple‐comparison adjustment, see Table 6.
Across exploratory endpoints, RAD also showed consistent normal‐tissue sparing. The mean heart dose was markedly lower in RAD plans (1.15 Gy vs. 2.10 Gy; p = 0.001), and the mean lung dose was reduced by approximately 27% (p = 0.040). Significant decreases were also observed in Lung V5 Gy, V10 Gy, and V20 Gy (p = 0.035, 0.033, and 0.034, respectively), demonstrating reduced low‐ and intermediate‐dose spillage to healthy lung tissue, see Table 6.
Overall, RAD planning provided enhanced conformity and superior OAR sparing while maintaining equivalent PTV coverage in lung SBRT. For the ten analyzed cases, treatments were prescribed per institutional protocols, ranging from 24 Gy in three fractions to 40 Gy in 5 fractions, depending on tumor size and proximity to critical structures. Figure 3 illustrates a representative lung SBRT case, where the RAD plan showed improved conformity and reduced heart and lung dose spillage compared with the conventional RA plan.
Comparison of 50% of prescription isodose distribution between conventional RapidArc and RapidArc dynamic plans for a lung SBRT.
Head and neck
3.4
The comparison between RapidArc dynamic (RAD) and conventional RapidArc (RA) plans for head‐and‐neck cases demonstrated similar target coverage across all planning target volumes (PTVs), with no statistically significant differences observed (p > 0.05; Table 7).
For the primary endpoints, the mean dose to the left and right parotid glands was reduced by 9.7% and 14.2%, respectively, in RAD compared to RA plans (p = 0.010 for both). After Bonferroni correction (m = 3; adjusted α = 0.0167), both parameters remained trending toward significance, indicating a consistent improvement in parotid sparing. The maximum dose to the spinal cord PRV decreased by 8.6% (p = 0.020), demonstrating a meaningful though non‐significant reduction after correction, see Table 7.
Across exploratory endpoints, RAD plans consistently provided improved sparing of critical structures. The mean dose to the mucosal constrictors was reduced by 9.2% (p = 0.010), and the mean lip dose decreased by 23.4% (p = 0.010). Further reductions were observed for the larynx (−8.2%, p = 0.020), esophagus (−18.2%, p = 0.010), and oral cavity (−15.1%, p = 0.010). The maximum doses to the brainstem and spinal cord PRVs were lower by 4.6% and 8.6%, respectively (both p ≈ 0.02).
No significant differences were detected for the optic nerves (p > 0.05), while the optic chiasm PRV showed a trend toward reduction (−5.6%, p = 0.040). The mean cochlear doses were substantially reduced by 14.9% on the left and 14.8% on the right (p = 0.010), and the lens maximum doses decreased by 20.0% and 18.5% on the left and right sides, respectively (p = 0.010), see Table 7.
Overall, RAD planning achieved improved sparing of multiple organs‐at‐risk while maintaining equivalent PTV coverage in head‐and‐neck cases. The most notable reductions were observed for the parotid glands, lips, cochleae, esophagus, oral cavity, larynx and lenses; although parotids and spinal cord dose reductions were clinically meaningful, they did not reach statistical significance after Bonferroni correction and should be interpreted as trends. Figure 4 illustrates the 35 Gy (50% prescription) isodose distribution comparison between RA and RAD plans for a representative head‐and‐neck case, demonstrating reduced low‐dose spillage and improved OAR sparing with the RAD technique.
Comparison of the 35 Gy (50% of prescription) isodose distribution between conventional RapidArc and RapidArc dynamic plans for a head and neck case.
DISCUSSION
4
This dosimetric study demonstrates that RapidArc Dynamic (RAD) achieves superior treatment plan quality compared to conventional RapidArc (RA) across breast, prostate, lung SBRT, and head and neck cancer cases. RAD consistently enhanced organ‐at‐risk (OAR) sparing and dose conformity while maintaining equivalent target coverage, underscoring its potential to advance precision in volumetric modulated arc therapy (VMAT).
For breast cancer, RAD significantly reduced mean doses to the heart, contralateral breast, and contralateral lung, alongside lower ipsilateral lung V5 Gy exposure. These improvements are clinically critical, as minimizing low‐dose spillage to healthy tissues is associated with reduced risks of cardiopulmonary complications and secondary malignancies in breast radiotherapy.6, 7 The integration of auto skin flash tools in RAD further ensured robust superficial target coverage, addressing setup uncertainties without manual bolus adjustments a practical advantage for complex breast geometries and at the same time reduced planning time.
In prostate cases, RAD improved rectal and bladder sparing compared to RA, along with enhanced sparing of femoral heads and bone marrow. Such dosimetric gains align with modern goals of minimizing genitourinary (GU) and gastrointestinal (GI) toxicities,8, 9 which directly impact long‐term patient quality of life. The ability to strategically embed static fields within arcs likely contributed to these outcomes by refining dose modulation near critical structures.
For lung SBRT, RAD's superior conformity indices and reduced spinal cord, heart, and lung doses highlight its suitability for high‐precision treatments requiring steep dose gradients. The dynamic collimator rotation and embedded static beams in RAD enabled sharper dose fall‐off, critical for preserving central structures while delivering ablative doses to tumors.10, 11 These technical enhancements may translate to safer dose escalation in challenging SBRT cases.
In head and neck cancer, RAD improved sparing of multiple head‐and‐neck OARs—key predictors of functional outcomes such as salivary function, swallowing, and hearing preservation.12, 13, 14 The ability to pause gantry rotation for optimal beam modulation likely facilitated these improvements, demonstrating RAD's adaptability in anatomically complex regions.
The dosimetric advantages of RAD stem from its advanced delivery features: dynamic collimator adjustments, embedded static fields, and a faster Photon Optimizer algorithm. These innovations allow finer control over dose distributions, particularly for concave targets or tumors near serial OARs. However, these benefits came with increased monitor units (MUs) (e.g., 912 vs. 731 MUs for breast cases). The higher MU count is primarily attributed to the integration of static IMRT fields within arcs, which inherently require additional beam modulation. While a portion of these MUs are blocked by the multileaf collimator (MLC) during delivery—similar to sliding window IMRT techniques—and do not directly contribute to patient dose, the higher MU count observed in RAD plans could theoretically contribute to increased secondary leakage and scatter radiation. However, we did not quantify integral dose or out‐of‐field dose in this study, and therefore this possibility remains speculative. Future work should explicitly assess these parameters to clarify the clinical relevance.
Another practical consideration is planning time. In this study, planning times for RAD were moderately shorter than for RA; however, it is important to note that our clinical team had extensive prior experience with RA and was relatively new to the RAD planning platform. With increasing familiarity and optimization of planning workflows, it is anticipated that RAD planning times could be further reduced.
Despite promising dosimetric outcomes, the clinical relevance of these findings—specifically, whether they translate to reduced toxicities—requires validation through long‐term follow‐up and prospective trials. Additionally, the planning time and complexity associated with RAD warrant further evaluation to optimize workflow integration fully.
This study has several limitations. First, its retrospective nature means that the conventional RA plans were created in clinical settings, while the RAD plans were created specifically for this comparison. This could potentially introduce bias, although we attempted to minimize this by using identical clinical objectives and constraints.
Second, while we demonstrated dosimetric improvements with RAD, these do not necessarily translate directly to clinical benefit. Long‐term follow‐up studies will be necessary to confirm whether the dosimetric advantages result in reduced toxicity rates or improved quality of life.
Third, we did not perform a cost‐effectiveness analysis of implementing RAD, which would require consideration of software/hardware upgrade costs, potential workflow efficiencies, and the monetary value of potential toxicity reductions.
Fourth limitation of this study is that plan verification was not performed. As our center was among the limited sites worldwide participating in the RAD evaluation phase organized by Varian Medical Systems, we only had access to the planning license, while delivery and verification would have required a separate machine license that was not available. Future investigations should incorporate patient‐specific quality assurance and delivery verification to comprehensively evaluate the clinical feasibility of RAD.
Finally, our study focused on specific anatomical sites and may not be generalizable to all clinical scenarios. Additional research is needed to evaluate RAD's performance in other treatment sites and special techniques such as stereotactic radiosurgery or total body irradiation.
CONCLUSION
5
In conclusion, this study was designed to compare conventional RapidArc (RA) and RapidArc Dynamic (RAD) across four anatomical sites (breast, prostate, lung SBRT, and head and neck) using identical optimization objectives and dose calculation settings. We found that RAD consistently maintained equivalent target coverage while improving dose conformity and providing superior sparing of critical organs at risk—such as the heart and contralateral lung in breast cancer, rectum and bladder in prostate cancer, spinal cord and heart in lung SBRT, and parotid glands and mucosal structures in head and neck cases. Although RAD plans required higher monitor units, planning efficiency was modestly improved. Taken together, these results demonstrate that RAD represents a meaningful advancement in VMAT delivery, particularly for anatomically complex and high‐precision treatments. Future work should validate these dosimetric advantages in prospective clinical studies and explore the integration of RAD into adaptive radiotherapy workflows.
AUTHOR CONTRIBUTIONS
Aram Rostami: Co‐authored sections, directed all content, proofing all content, contributed in planning part and analysis, and contributed to writing the manuscript. Carole Naim: Contributed in planning part and writing the manuscript. Renilmon Pottanplackal Sukumaran: Co‐authored sections, contributed in planning part and writing the manuscript. Muhammad Usman: Contributed planning part and proofing all content. Abbass Yousef Mkanna: Contributed planning part and proofing all content. Alla Fuad Al Sabahi: Contributed planning part and proofing all content. Ahamed Basith: Contributed planning part and proofing all content. Shelton Chuck: Contributed planning part and proofing all content. Mojtaba Barzegar: Statistical Analyzes and created figures. Bevan Orville Peltier: Contributed Planning part. Bassim Aklan: Creating all Figures and proofing all content Samaneh Baradaran: Statistical Analyzes and proofing all content. Satheesh Prasad Paloor: Co‐authored sections, proofing all content. Rabih Wafiq Hammoud: Co‐authored sections, directed all content, and co‐developed proofing all content.
CONFLICT OF INTEREST STATEMENT
The authors declare that this study was conducted independently without any involvement from the vendor. The vendor had no access to patient data, treatment plans, analysis workflows, or the manuscript at any stage. No financial or material support was provided by the vendor for this project. All research activities, data interpretation, and manuscript preparation were carried out solely by the authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Otto K , Volumetric modulated arc therapy: i MRT in a single gantry arc. Med Phys. 2008;35(1):310–317. doi:10.1118/1.2818738 18293586 10.1118/1.2818738 · doi ↗ · pubmed ↗
- 2Nicolini G , Vanetti E , Clivio A , Cozzi L , Fogliata A . Evaluation of a Rapid Arc plan optimization strategy for complex cases. Radiat Oncol. 2008;3:42. doi:10.1186/1748‐717X‐3‐42 19087250
- 3Li G , Zhang Y , Jiang X , Song X , Wang B , Gao Y , et al. Dosimetric comparison of VMAT with Rapid Arc and helical tomotherapy for nasopharyngeal carcinoma. Radiat Oncol. 2013;8:145. doi:10.1186/1748‐717X‐8‐145 23773560
- 4Varian Medical Systems . Photon and Electron Algorithms Reference Guide: Eclipse Treatment Planning System. Palo Alto, CA: Varian Medical Systems; 2024.
- 5Paddick I . A simple scoring ratio to index the conformity of radiosurgical treatment plans. J Neurosurg. 2000;93(Suppl 3):219–222. doi:10.3171/jns.2000.93.supplement 11143252 10.3171/jns.2000.93.supplement · doi ↗ · pubmed ↗
- 6Darby SC , Ewertz M , Mc Gale P , et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987‐998. doi:10.1056/NEJ Moa 1209825 23484825 10.1056/NEJ Moa 1209825 · doi ↗ · pubmed ↗
- 7Taylor C , Kirby AM . Cardiac side‐effects from breast cancer radiotherapy. Clin Oncol (R Coll Radiol). 2015;27(11):621–629. doi:10.1016/j.clon.2015.06.007 26133462 10.1016/j.clon.2015.06.007 · doi ↗ · pubmed ↗
- 8Michalski JM , Yan Y , Watkins‐Bruner D , et al. Preliminary toxicity analysis of 3‐dimensional conformal radiation therapy versus intensity‐modulated radiation therapy on the high‐dose arm of the Radiation Therapy Oncology Group 0126 prostate cancer trial. Int J Radiat Oncol Biol Phys. 2013;87(5):932‐938. doi:10.1016/j.ijrobp.2013.08.013 24113055 10.1016/j.ijrobp.2013.07.041PMC 3840044 · doi ↗ · pubmed ↗