Leukemia cutis with concomitant acrodermatitis chronica atrophicans and chronic B‐cell lymphocytic leukemia: complete clearance under doxycycline therapy
Sven‐Niklas Burmann, Thilo Gambichler, Jürgen C. Becker, Frank Oellig, Alexander Kreuter, Ulrich Peter Wehry

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1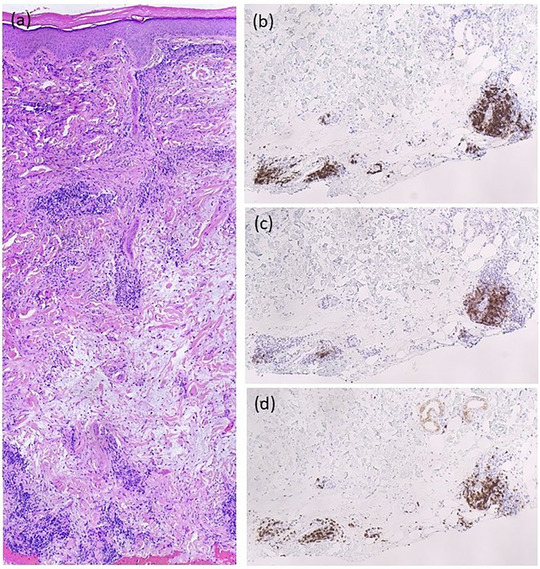 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Chronic Lymphocytic Leukemia Research · Inflammatory Myopathies and Dermatomyositis
Dear Editors,
Leukemia cutis (LC) is a rare cutaneous manifestation in hematologic malignancies. It arises from secondary infiltration of leukemic cells into the skin, although the pathomechanism is not yet fully understood.1, 2, 3, 4 In this case report, we describe a patient who was diagnosed with both LC as a manifestation of chronic lymphocytic leukemia (CLL) and acrodermatitis chronica atrophicans (ACA). The underlying CLL was identified only during dermatopathological analysis. Following oral doxycycline treatment for Lyme disease, complete regression of the LC was observed.
A 67‐year‐old man presented with asymptomatic, disseminated subcutaneous nodules that had been present for 6 months, progressively increasing in both number and size (Figure 1a). Additionally, around the same time, large, cushion‐like, livid plaques developed on the forearms and hands (Figure 1b). No relevant internal medical history was known, and the patient was not on any medication. Histopathological examination of a subcutaneous nodule from the trunk revealed superficial and deeper perivascular lymphocytic infiltration without plasma cells or epidermal involvement. Immunohistochemical expression of CD5, CD20, and CD23 suggested cutaneous infiltration of a B‐cell lymphoma, indicative of LC (Figure 2a–d). A subsequent punch biopsy of a livid plaque on the forearm revealed CD138‐positive plasma cells. Due to the clinical and histological appearance of ACA on the forearms and hands, PCR analysis was performed on both this biopsy and the LC, and both tested positive for Borrelia (B.) burgdorferi DNA. Furthermore, a positive IgG immunoblot (antigens: DbpA, Osp17, OspC, p21, p30, p39, p43, p84, and VlsE) and a positive Lyme disease serology (B. burgdorferi IgG/IgM EIA) confirmed the diagnosis of chronic Borrelia infection. Additional diagnostics revealed leukocytosis (96,000/µl; normal range: 4,400–11,000/µl) with markedly elevated B‐cell counts (53,320/µl; normal range: 100–500/µl). A subsequent bone marrow biopsy revealed infiltration by a low‐grade non‐Hodgkin lymphoma consistent with CLL. Mutation analysis revealed intermediate genetic risk (unmutated IGHV status, no del(17p) or TP53 mutation, no complex karyotype). Imaging revealed diffuse lymphadenopathy and splenomegaly.
In light of these findings, the diagnosis of LC in the context of CLL with accompanying ACA was established. As treatment for chronic Lyme disease with doxycycline had already been planned and there was no current indication for CLL‐specific therapy, oral doxycycline treatment was initiated. This resulted not only in a marked fading of the livid plaques (ACA lesions) on the forearms and hands, but also in a reduction of the subcutaneous nodules. For this reason, the doxycycline treatment was continued at a lower dose (100 mg once daily) for 3 months, leading to complete healing of all skin changes (Figure 1c,d). The patient has now been under oncological follow‐up for 2 years and is still free of skin manifestations. During this period, no specific therapy for CLL (watch‐and‐wait strategy) has been conducted, which confirms the successful treatment of LC with purely antibiotic monotherapy.
LC most commonly occurs in acute myeloid leukemia (AML) and is less frequently observed in patients with CLL. Its presence often indicates an advanced or particularly aggressive course of the underlying disease, as is frequently the case in AML. Overall, LC is a sign of extramedullary leukemia activity and indicates an advanced stage of disease.4 ACA is a frequently overlooked but serious complication of Lyme disease that requires early treatment. An association between Lyme disease and primary cutaneous B‐cell lymphomas, such as primary cutaneous marginal zone lymphoma, has been described in the literature. Similar to the present case, patients with B. burgdorferi‐associated primary cutaneous marginal zone lymphoma showed clinical resolution without recurrence after 3 weeks of oral tetracycline therapy.5, 6 In addition to Borrelia burgdorferi, other infections such as syphilis and herpesviruses have been described as triggers of similar skin manifestations. This underscores the importance of comprehensive infectious workup when LC is suspected.1, 2, 3 The clinical presentation of LC in the context of CLL is broad, ranging from nonspecific skin changes to aggressive, neoplastic skin infiltrates.7 Pseudolymphomatous infiltrates, typically presenting as dense B‐ and T‐cell infiltrates that can mimic hematologic malignancies, should be differentiated from this condition.8 The mechanisms underlying this association are not yet fully understood. In addition to inflammatory disruption of the blood–skin barrier, chronic antigenic stimulation of B‐cells by the pathogen – enhanced by Toll‐like receptor (TLR) activation, particularly via TLR9 – has been proposed. This activation leads to an increased clonal expansion of B cells.9 In fact, skin infiltrates of CLL can also be triggered by topical imiquimod therapy.10 Furthermore, Borrelia lipoproteins such as OspA and OspC can act as activators of TLR2, thereby releasing pro‐inflammatory cytokines such as TNF‐α, IL‐6, and IL‐1β. This can modify the tumor microenvironment accordingly.11 Drawing parallels to Helicobacter pylori‐associated MALT lymphomas, antibiotic therapy for eradicating the underlying infection could, as shown in our case, be a promising treatment option.12
Our case report illustrates the rare phenomenon of LC in the context of CLL and a B. burgdorferi infection. Early diagnosis and appropriate treatment of the underlying infection have a significant impact on the clinical course of the malignant disease.
CONFLICT OF INTEREST STATEMENT
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cerroni L , Höfler G , Bäck B , et al. Specific cutaneous infiltrates of B‐cell chronic lymphocytic leukemia (B‐CLL) at sites typical for Borrelia burgdorferi infection. J Cutan Pathol. 2002;29:142‐147.11972710 10.1034/j.1600-0560.2002.290303.x · doi ↗ · pubmed ↗
- 2Hofmann H , Margos G , Todorova A , et al. Case report of disseminated borrelial lymphocytoma with isolation of Borrelia burgdorferi sensu stricto in chronic lymphatic leukemia stage Binet A – an 11 year follow up. Front Med. 2024;11:1465630.10.3389/fmed.2024.1465630 PMC 1152765539493706 · doi ↗ · pubmed ↗
- 3Kash N , Fink‐Puches R , Cerroni L . Cutaneous Manifestations of B‐Cell Chronic Lymphocytic Leukemia Associated With Borrelia burgdorferi Infection Showing a Marginal Zone B‐Cell Lymphoma‐Like Infiltrate. Am J Dermatopathol. 2011;33:712‐715.21946761 10.1097/DAD.0b 013e 3181 fc 576f · doi ↗ · pubmed ↗
- 4Gambichler T , Herde M , Hoffmann K , et al. Poor prognosis of acute myeloid leukaemia associated with leukaemia cutis. J Eur Acad Dermatol Venereol. 2002;16:177‐178.12046831 10.1046/j.1468-3083.2002.00392_5.x · doi ↗ · pubmed ↗
- 5Gambichler T , Jridi R , Bernd H‐W , et al. Unusual Presentation of Acrodermatitis Chronica Atrophicans Resulting in Delay of Diagnosis and Inappropriate Treatment in Three Cases. Dermato. 2024;4:37‐45.
- 6Bertolotti A , Pham‐Ledard A , Petrot D , et al. Two cases of proliferation of monoclonal and monotypic lymphocytes and plasma cells corresponding to acrodermatitis chronica atrophicans. Ann Dermatol Venereol. 2014;141:452‐457.24951145 10.1016/j.annder.2014.04.117 · doi ↗ · pubmed ↗
- 7Aldapt MB , Yassin M . Leukemia Cutis as an Early Presentation or Relapsing Manifestation of CLL. Acta Biomed. 2021;92:e 2021192.33988158 10.23750/abm.v 92i 2.10763 PMC 8182576 · doi ↗ · pubmed ↗
- 8Kempf W , Kazakov DV , Hübscher E , Tinguely M . Cutaneous Borreliosis With a T‐Cell‐Rich Infiltrate and Simultaneous Involvement by B‐Cell Chronic Lymphocytic Leukemia With t(14;18)(q 32;q 21). Am J Dermatopathol. 2015;37:715‐718.25171429 10.1097/DAD.0000000000000216 · doi ↗ · pubmed ↗