A Randomized Controlled Trial Comparing Intrathecal 0.5% Hyperbaric Levobupivacaine and 0.75% Hyperbaric Ropivacaine for Elective Caesarean Section
Abhishek Chatterjee, Ayan Maity, Umesh K Singh, Deb Sanjay Nag, Zaid M Nafe

TL;DR
This study compares two spinal anesthetics for caesarean sections, finding each has distinct advantages in terms of block duration, recovery, and neonatal outcomes.
Contribution
The study provides a direct comparison of levobupivacaine and ropivacaine for spinal anesthesia in caesarean sections, highlighting their respective clinical benefits.
Findings
Levobupivacaine provides faster and longer-lasting sensory and motor block.
Ropivacaine offers better haemodynamic stability and quicker motor recovery.
Ropivacaine is associated with higher Apgar scores in newborns.
Abstract
Introduction: This randomized, double-blind, controlled trial compared intrathecal 0.5% hyperbaric levobupivacaine with 0.75% hyperbaric ropivacaine in parturients undergoing elective caesarean section to evaluate sensory and motor block profiles, haemodynamic stability, neonatal outcomes, and adverse effects. Methods: Sixty-six American Society of Anesthesiologists (ASA) physical status I or II parturients were randomized equally into a levobupivacaine group (Group L) and a ropivacaine group (Group R). Sensory block onset, peak level, regression, motor block onset, Bromage progression, and recovery were recorded using standardized protocols. Haemodynamic variables were measured at fixed intervals following spinal administration. Neonatal well-being was evaluated using Apgar scores at one and five minutes. Statistical analysis included the independent t-test, Mann-Whitney U test, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
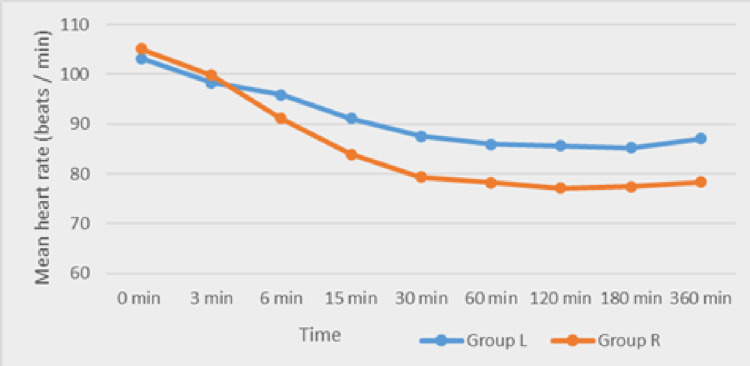 Figure 1
Figure 1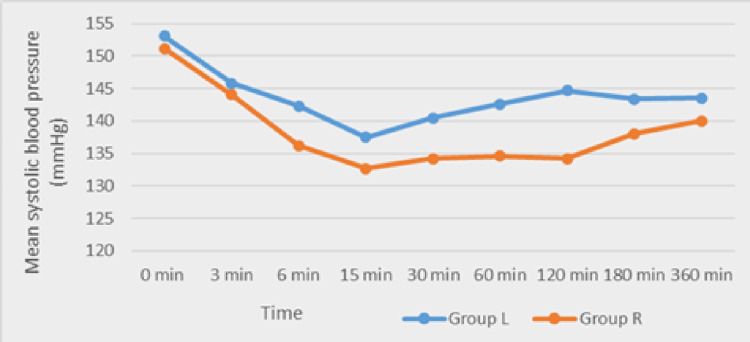 Figure 2
Figure 2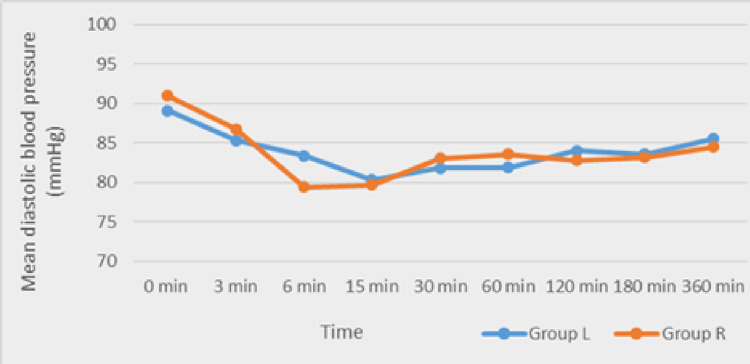 Figure 3
Figure 3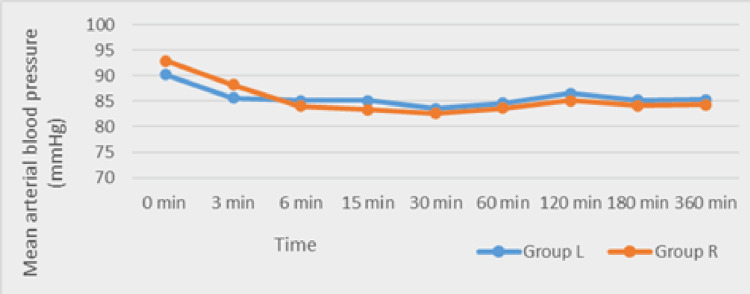 Figure 4
Figure 4| Sensory block characteristics | Group L (n=33) | Group R (n=33) | P-value |
| Time taken for the onset of sensory block (in min) | 3.6±0.72 | 4.2±1.0 | 0.002 |
| Time taken for the sensory block to reach T12 (in min) | 5.1±0.80 | 6.7±0.25 | 0.04 |
| Time taken to peak sensory block (in min) | 6.60±0.40 | 7.45±0.82 | 0.0005 |
| Time taken by sensory block to regress by 2 levels | 130.0±8.3 | 110.0±7.9 | 0.0001 |
| Mean duration of sensory block (in min) | 162.5±21.4 | 150.7±42.8 | 0.0002 |
| Motor block characteristics | Group L (n=33) | Group R (n=33) | P-value |
| Time taken for the onset of motor block (in min) | 5.4±0.72 | 6.3±0.80 | 0.003 |
| Time to reach Bromage score 3 (in min) | 6.9±0.75 | 8.2±0.70 | 0.02 |
| Time to regress to Bromage score 1 (in min) | 120±6.25 | 105±5.92 | 0.0005 |
| Mean duration of motor block (in min) | 148±26.40 | 132±28.75 | 0.0001 |
| Parameter | Group L (n=33) | Group R (n=33) | P-value |
| Mean time to first rescue analgesia (in min) | 188±5.12 | 172±6.03 | 0.0001 |
| Complications | Group L (n=33) | Group R (n=33) | P-value | Degree of freedom | Effect size |
| Hypotension | 8 (24.2%) | 4 (12.1%) | 0.18 | 1 | 0.16 |
| Bradycardia | 5 (15.2%) | 2 (6.1%) | 0.23 | 1 | 0.14 |
| Nausea | 6 (18.2%) | 3 (9.1%) | 0.28 | 1 | 0.13 |
| Vomiting | 4 (12.1%) | 2 (6.1%) | 0.39 | 1 | 0.1 |
| Shivering | 5 (15.2%) | 2 (6.1%) | 0.23 | 1 | 0.14 |
| Headache | 2 (6.1%) | 1 (3%) | 0.55 | 1 | 0.07 |
| Transient neurological symptoms (TNS) | 1 (3%) | 0 (0%) | 0.31 | 1 | 0.12 |
| Study | HR | SBP | DBP | MBP | SpO₂ |
| Present study | Group R lower from 15 min onwards (p<0.05) | Group R lower from 30 min onwards (p<0.05) | Similar except at 6 min (lower in Group R; p=0.007) | Comparable throughout | Stable and comparable |
| Bhalekar et al. [ | Not explicitly compared | Not detailed | Not detailed | Not mentioned | Not mentioned |
| Hazarika et al. [ | No significant difference | Significant at 5, 10, and 75 min | Significant at 5, 30, and 180 min | Not reported | Not reported |
| Sharma et al. [ | Ropivacaine showed a more stable HR | Smaller drop in Group R (more stable) | Less drop in Group R | Higher in Group R (p<0.05) | Stable and comparable |
| Study | Onset of sensory block (min) | Duration of sensory block (min) | Regression of sensory block by 2 levels (min) |
| Present study | Group L: 3.6±0.72; Group R: 4.2±1.0 | Group L: 162.5±21.4; Group R: 150.7±42.8 | Group L: 130.0±8.3; Group R: 110.0±7.9 |
| Bhalekar et al. [ | Not stated explicitly | Not explicitly reported | Not specified |
| Hazarika et al. [ | Group L: 7.03±1.61; Group R: 5.71±1.75 | Group L: 216.7±18.9; Group R: 193.7±14.1 | Group L: 99.4±15.0; Group R: 88.7±15.6 |
| Sharma et al. [ | Group L faster (exact not quoted) | Longer in Group L (statistically significant) | Group L slower (longer regression time) |
| Gautier et al. [ | Group L slightly slower (not detailed) | Not directly compared | Reported but not numerically detailed |
| Study | Onset of motor block (min) | Time to Bromage score 3 (min) | Duration of motor block (min) | Motor block regression to Bromage score 1 (min) |
| Present study | Group L: 5.4±0.72; Group R: 6.3±0.80 | Group L: 6.9±0.75; Group R: 8.2±0.70 | Group L: 148±26.4; Group R: 132±28.75 | Group L: 120±6.25; Group R: 105±5.92 |
| Bhalekar et al. [ | Not clearly stated | Not specified | Not detailed | Not stated |
| Hazarika et al. [ | Group L: 3.8±1.25; Group R: 2.54±1.03 | Group L: 8.37±2.90; Group R: 6.02±1.58 | Group L longer (exact values not stated) | Group R faster (exact not stated) |
| Sharma et al. [ | Faster in Group L (exact not quoted) | Faster in Group L | Group L longer (stat. sig.) | Group R faster (significant) |
| Gautier et al., Agarwal et al., Goyal et al. [ | Group L slower than ropivacaine (not detailed) | Ropivacaine shorter time (estimated) | Levobupivacaine shorter vs. bupivacaine | Not reported |
| Study | Hypotension | Bradycardia | Nausea/vomiting | Shivering | Headache |
| Present study | Group L: 24.2%; Group R: 12.1% (NS) | Group L: 15.2%; Group R: 6.1% (NS) | Nausea: L. 18.2%; R, 9.1%. Vomiting: L, 12.1%; R, 6.1% | Group L: 15.2%; Group R: 6.1% (NS) | Group L: 6.1%; Group R: 3% (NS) |
| Hazarika et al. [ | Group L: 2 pts; Group R: 3 pts (NS) | Group L: 0 pts; Group R: 1 pt | Nausea: L, 2 pts; R, 1 pt. Vomiting: not reported | Group L: 1 pt; Group R: 0 pts | Not reported |
| Sharma et al., Agarwal et al., Goyal et al. [ | Lower in Group R | Rare, not significantly different | Not discussed | Not reported | Not reported |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Pediatric Pain Management Techniques · Neonatal and fetal brain pathology
Introduction
Spinal anaesthesia remains the anaesthetic technique of choice for elective caesarean delivery due to its favourable safety profile, rapid onset, and ability to minimize fetal exposure to systemic drugs [1]. Over the past several decades, a range of local anaesthetic agents has been used for intrathecal administration, with hyperbaric bupivacaine traditionally regarded as the standard of care [2]. However, concerns related to cardiotoxicity and central nervous system toxicity associated with the racemic form of bupivacaine have led to the exploration of safer alternatives. Levobupivacaine, the pure S(-) enantiomer of bupivacaine, and ropivacaine, another S(-) enantiomer with lower lipid solubility, have emerged as two promising options for spinal anaesthesia [3,4]. Both agents offer improved cardiovascular safety profiles while providing effective sensory and motor blockade [5,6].
Although extensive literature exists on the comparative safety and efficacy of these agents in a variety of clinical settings, relatively fewer studies have directly compared equipotent intrathecal doses of hyperbaric levobupivacaine and hyperbaric ropivacaine in obstetric anaesthesia. The physiological changes of pregnancy, including increased sensitivity to local anaesthetics and altered haemodynamics, warrant focused investigation into the performance of these drugs in parturients. Understanding their differential effects on sensory block characteristics, motor blockade, maternal haemodynamic stability, and neonatal outcomes is essential for optimizing anaesthetic protocols and ensuring the safety of both mother and child.
The present randomized, double-blind, controlled trial was designed to address this gap by directly comparing 0.5% hyperbaric levobupivacaine with 0.75% hyperbaric ropivacaine in elective caesarean delivery. The primary outcomes included onset and duration of sensory and motor block, while the secondary outcomes encompassed haemodynamic profiles, neonatal Apgar scores, postoperative analgesia requirements, and incidence of complications. This investigation seeks to provide comprehensive clinical insights that may inform evidence-based selection of intrathecal agents in obstetric practice.
Materials and methods
This prospective, randomized, double-blind, controlled trial was conducted at Tata Main Hospital, Jamshedpur, India, over an eight-month period after obtaining approval from the institute's Institutional Ethics Committee (approval number: TMH/IEC/JAN/091/2023). The study was also registered at Clinical Trials Registry-India (CTRI) (ID: CTRI/2025/07/091610). Sixty-six American Society of Anesthesiologists (ASA) physical status I or II parturients aged 18 years or older and scheduled for elective lower-segment caesarean section under spinal anaesthesia were included. Exclusion criteria comprised patient refusal, contraindications to neuraxial anaesthesia, coagulopathy, infection at the injection site, hypersensitivity to amide local anaesthetics, and BMI ≥30 kg/m².
Participants were randomized into two groups of 33 each using a computer-generated sequence concealed in opaque envelopes. The levobupivacaine group (Group L) received 2.6 mL of 0.5% hyperbaric levobupivacaine, while the ropivacaine group (Group R) received 2.6 mL of 0.75% hyperbaric ropivacaine. All spinal injections were administered at the L3-L4 interspace with the patient in the sitting position using a 27G Quincke needle. Immediately after intrathecal injection, patients were positioned supine with left uterine displacement to prevent aortocaval compression.
Sensory block assessment was performed using alcohol-soaked pledgets [7], every two minutes for the first 10 minutes, followed by assessments at 15 and 20 minutes and subsequently at 30-minute intervals until regression to the L5 dermatome. Motor block was evaluated concurrently using the Modified Bromage Scale by the same observer to avoid inter-observer variation. Haemodynamic parameters, including heart rate, systolic blood pressure, diastolic blood pressure, mean arterial pressure, and oxygen saturation, were recorded at baseline and at regular intervals up to 360 minutes. Hypotension was defined as a reduction greater than 20% from baseline values. Neonatal outcome assessment included Apgar scoring at one and five minutes after birth [7].
Data were analyzed using IBM SPSS Statistics for Windows, Version 29.0 (Released 2019; IBM Corp., Armonk, New York, United States). Continuous variables were tested for normality and analyzed with the independent t-test or Mann-Whitney U test as appropriate. Categorical variables were compared using the chi-squared test. Statistical significance was set at p<0.05.
Results
The demographic variables of age, height, weight, and BMI were comparable between groups. Sensory block characteristics (Table 1) showed significantly faster onset in the levobupivacaine group, which also achieved peak sensory level earlier and demonstrated longer duration of block and slower regression by two dermatomal levels.
Motor block (Table 2) showed a similar pattern, with levobupivacaine producing faster onset, faster attainment of Bromage score 3, and prolonged duration, whereas ropivacaine enabled more rapid recovery. There were no significant differences between the groups when we compared surgical readiness and total duration of surgery.
Haemodynamic monitoring demonstrated that ropivacaine was associated with comparatively lower heart rate and systolic blood pressure from approximately 15 to 30 minutes onwards, though values remained clinically acceptable (Figures 1-2).
Comparison of the mean heart rate between Group L and Group R Group L: levobupivacaine group; Group R: ropivacaine group
Comparison of the mean systolic blood pressure between Group L and Group R Group L: levobupivacaine group; Group R: ropivacaine group
The mean diastolic blood pressure and mean arterial blood pressure (Figures 3-4) did not differ significantly between groups.
Comparison of the mean diastolic blood pressure between Group L and Group RGroup L: levobupivacaine group; Group R: ropivacaine group
Comparison of the mean arterial blood pressure between Group L and Group RGroup L: levobupivacaine group; Group R: ropivacaine group
Oxygen saturation values remained stable. Neonatal outcomes revealed statistically higher Apgar scores at one and five minutes in the ropivacaine group. However, all scores fell within normal limits, and no newborn required resuscitative intervention. The time required for first rescue analgesia was significantly longer in Group L as compared to Group R (Table 3).
Complications such as hypotension, bradycardia, nausea, vomiting, shivering, and headache occurred at similar frequencies in both groups, with no statistically significant differences (Table 4).
Discussion
This trial demonstrated clear differences between hyperbaric levobupivacaine and hyperbaric ropivacaine in spinal anaesthesia for caesarean delivery. Levobupivacaine exhibited a faster onset and longer duration of both sensory and motor block, consistent with its established pharmacological profile. These characteristics contribute to its suitability for longer surgical durations and extended postoperative analgesia. In contrast, ropivacaine's shorter duration and faster motor recovery align with its lower lipid solubility and reduced motor block intensity, making it advantageous in contexts where early mobilization is desirable.
The superior haemodynamic stability observed with ropivacaine in this study aligns with previous research with similar timelines (Table 5), indicating that its lower cardiotoxic potential contributes to more favourable cardiovascular patterns. Although levobupivacaine maintained stable haemodynamics overall, its association with slightly higher rates of hypotension and bradycardia, though not statistically significant, warrants consideration in high-risk patients. There was no significant difference between the two groups when we compared the amount of vasopressors required to correct hypotension.
Additionally, neonatal Apgar scores were significantly higher in the ropivacaine group, suggesting that ropivacaine may provide superior early neonatal outcomes, potentially due to improved maternal haemodynamic stability and reduced transplacental drug transfer.
The findings of this investigation are consistent with several prior studies (Tables 6-8) comparing these agents, reinforcing the relevance of drug selection based on clinical context. Levobupivacaine may be preferred when prolonged sensory or motor blockade is advantageous, whereas ropivacaine may be chosen to enhance maternal haemodynamic stability and neonatal well-being.
Limitations of the present study
This was a single-center study. A large sample size would have helped us in revealing potential rare complications of study drugs like neurotoxicity [14] and cardiovascular complications [15]. Also, we did not include emergency surgeries and pregnant patients with multiple comorbidities in the present study.
Conclusions
This randomized controlled trial demonstrates that 0.5% hyperbaric levobupivacaine provides a denser and more prolonged sensory and motor block than 0.75% hyperbaric ropivacaine in parturients undergoing elective caesarean section. Levobupivacaine offers extended analgesia and delayed need for rescue analgesics, while ropivacaine offers superior haemodynamic stability, quicker recovery from motor block, and more favourable neonatal Apgar scores. Both agents are effective and safe for spinal anaesthesia in caesarean delivery. Clinicians should base their choice on surgical requirements, patient characteristics, and the need for early postoperative mobilization or enhanced neonatal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anesthesia-related deaths during obstetric delivery in the United States, 1979-1990 Anesthesiology Hawkins JL Koonin LM Palmer SK Gibbs CP 277284861997905424510.1097/00000542-199702000-00002 · doi ↗ · pubmed ↗
- 2Cardiac arrest following regional anesthesia with etidocaine or bupivacaine Anesthesiology Albright GA 28528751197948488910.1097/00000542-197910000-00001 · doi ↗ · pubmed ↗
- 3A comparison of the cardiovascular effects of levobupivacaine and rac-bupivacaine following intravenous administration to healthy volunteers Br J Clin Pharmacol Bardsley H Gristwood R Baker H Watson N Nimmo W 245249461998976496510.1046/j.1365-2125.1998.00775.x PMC 1873676 · doi ↗ · pubmed ↗
- 4Levobupivacaine: a review of its pharmacology and use as a local anaesthetic Drugs Foster RH Markham A 5515795920001077683510.2165/00003495-200059030-00013 · doi ↗ · pubmed ↗
- 5Clinical profile of levobupivacaine in regional anesthesia: a systematic review J Anaesthesiol Clin Pharmacol Bajwa SJ Kaur J 5305392920132424999310.4103/0970-9185.119172 PMC 3819850 · doi ↗ · pubmed ↗
- 6Ropivacaine Br J Anaesth Mc Clure JH 300307761996877711510.1093/bja/76.2.300 · doi ↗ · pubmed ↗
- 7Efficacy of intrathecal 0.75% hyperbaric ropivacaine versus 0.5% hyperbaric bupivacaine for elective inguinal and perineal surgery: a randomised double-blinded clinical study J Clin Diagnostic Res Shah B Mahanta D 07192025
- 8A comparative study of intrathecal hyperbaric 0.5% levobupivacaine and hyperbaric 0.75% ropivacaine for lower segment caesarean section in pre-eclampsia parturients European J Cardiovasc Med Bhalekar A Hau R Singh AK Nayak AP Sachan S 355360142024 https://healthcare-bulletin.co.uk/article/a-comparative-study-of-intrathecal-hyperbaric-0-5-levobupivacaine-and-hyperbaric-0-75-ropivacaine-for-lower-segment-caesarean-section-in-pre-eclampsia-parturients-2446/