Localized nasal dermatosis in a healthy male
Aarohi Shah, Kevin Gaddis, Brittney Schultz

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
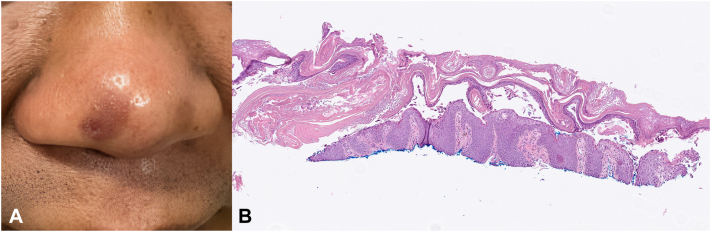 Figure 1
Figure 1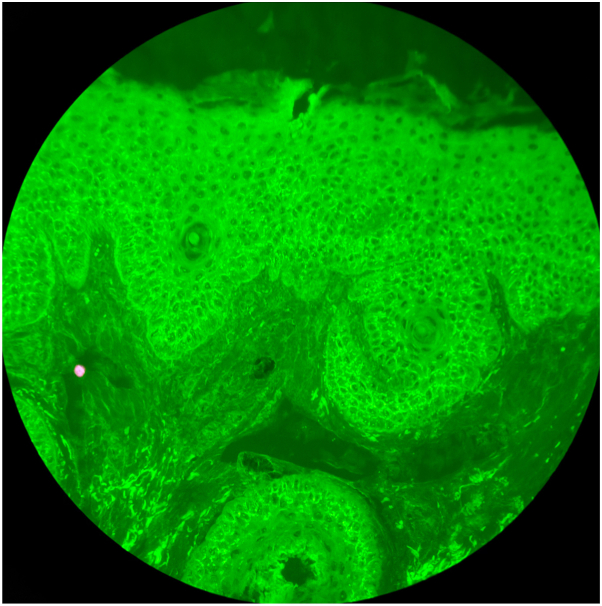 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Oral Health Pathology and Treatment · Genetic and rare skin diseases.
Case description
A 49-year-old male presented to the clinic with a 7 month history of pruritus on his nose. The patient was otherwise healthy and was on no medications. He had no similar eruption elsewhere. He had improvement but not resolution with ketoconazole cream and triamcinolone 0.025% cream. Physical examination revealed hyperpigmented macules with overlying scale on the nasolabial folds and nasal tip with 1 scaly papule (Fig 1, A). A biopsy specimen was obtained for histopathologic analysis (Fig 1, B).Fig 1A, Hyperpigmented patch on nose with erosion. B, Histopathology showing superficial acantholysis. Magnification and stain: hematoxylin and eosin, original magnification ×40.
Question: What is your diagnosis?
- **A.**Discoid lupus erythematosus
- **B.**Pemphigus foliaceus
- **C.**Facial discoid dermatosis
- **D.**Lupus pernio
- **E.**Sarcoidosis
Discussion
Histopathologic examination revealed superficial epidermal acantholysis. Direct immunofluorescence (DIF) revealed intercellular immunoglobulin (Ig) G and complement 3 (C3) in the lower epidermal keratinocytes (Fig 2). Indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA) or desmoglein (Dsg) 1 and 3 were within normal limits and antinuclear antibodies (ANAs) were negative. The patient showed improvement with tacrolimus 0.1% ointment.Fig 2. Direct immunofluorescence showing intercellular IgG deposition in lower epidermal keratinocytes. Magnification and stain: direct immunofluorescence—IgG, original magnification ×200.
Pemphigus foliaceus (PF) is an acquired autoimmune blistering disorder in which the immune system creates IgG antibodies that attack the intercellular adhesion glycoprotein Dsg 1, resulting in subcorneal blisters and acantholysis.1^,^2 Worldwide incidence and prevalence of PF is low. Localized PF is a rarely reported entity in the literature, with even fewer reported cases isolated to the nose.1, 2, 3 In current literature, cases of PF localized to the nose have remained confined, whereas others progressed beyond the nose.2^,^3 Localized pemphigus seems to favor seborrheic areas of the face, specifically the nose, though the reason is not completely clear.2^,^3 Previously reported cases have demonstrated various combinations of Dsg 1 and Dsg 3 antibodies, including negative Dsg 1 antibodies with positive Dsg 3 antibodies, as well as initially positive Dsg 1 antibodies with negative Dsg 3 antibodies later progressing to positive antibodies for both Dsg 3 and Dsg 1.2 It has been suggested that PF in sun-exposed areas may be attributed to the increased expression of Dsg 1 antigen in the face or increased exposure to ultraviolet light, as it may induce the binding of anti-Dsg 1 to the epidermis.2^,^3 Literature describing treatments of localized nasal PF includes variations of systemic corticosteroids, topical corticosteroids, calcineurin inhibitors, dapsone, and other immunosuppressive agents.3^,^4
Seronegativity in this case is suspected to be due to the localized nature of PF. Although ELISA and IIF are sensitive in detecting circulating anti-Dsg autoantibodies in widespread pemphigus foliaceus (PF), localized PF may involve antibody levels below detection thresholds or antibody sequestration within affected skin. Therefore, negative ELISA and IIF do not exclude PF, and biopsy with DIF becomes critical for diagnosis of localized PF. Interestingly, DIF in this patient showed intercellular IgG deposition confined to the lower half of the epidermis. In classic PF, staining is typically more prominent in the upper epidermis, correlating with Dsg 1 distribution.5 Further studies are needed to determine whether this staining pattern is distinct to localized presentations or reflects temporal disease evolution.
In conclusion, localized involvement of the nose is a rare presentation of pemphigus foliaceus. It seems to follow a more benign course and may be treated topically with topical corticosteroids or calcineurin inhibitors with escalation to systemic therapies if needed.2^,^4 Additional studies are needed to understand the pathogenesis of localized PF and what determines its progression to more extensive disease to provide optimal treatment.
Conflicts of interest
Brittney Schultz, MD: Argenx—Advisory Board (honoraria), AstraZeneca—Sub-investigator, UCB—Investigator, Regeneron/Sanofi—Advisory Board (honoraria).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1James K.A.Culton D.A.Diaz L.A.Diagnosis and clinical features of pemphigus foliaceus Dermatol Clin 293201140541210.1016/j.det.2011.03.01221605805 PMC 3108573 · doi ↗ · pubmed ↗
- 2Safadi M.G.Turowski M.Murray T.Zahner S.Aronson I.Pemphigus vulgaris and foliaceus localized to the nose: report of 2 cases JAAD Case Rep 15202112913210.1016/j.jdcr.2021.07.02634471665 PMC 8387825 · doi ↗ · pubmed ↗
- 3Kishibe M.Kinouchi M.Ishida-Yamamoto A.Koike K.Iizuka H.Pemphigus foliaceus localized to the nose Clin Exp Dermatol 285200356056210.1046/j.1365-2230.2003.01343.x 12950358 · doi ↗ · pubmed ↗
- 4Kunadia A.Moschella S.Mc Lemore J.Sami N.Localized pemphigus foliaceus: diverse presentations, treatment, and review of the literature Indian J Dermatol 681202312310.4103/ijd.ijd_324_22PMC 1016275637151255 · doi ↗ · pubmed ↗
- 5Lepe K.Yarrarapu S.N.S.Zito P.M.Pemphigus foliaceus Stat Pearls 2025 Stat Pearls Publishing 29763004 · pubmed ↗