Rare cutaneous coelomycete infection in an immunosuppressed patient: When morphology is not enough
Grace S. Saglimbeni, Maria Epino, A. Brian Mochon, Daniela C. Russi, Harper Price, Danielle Vargas de Stefano

Abstract
Click any figure to enlarge with its caption.
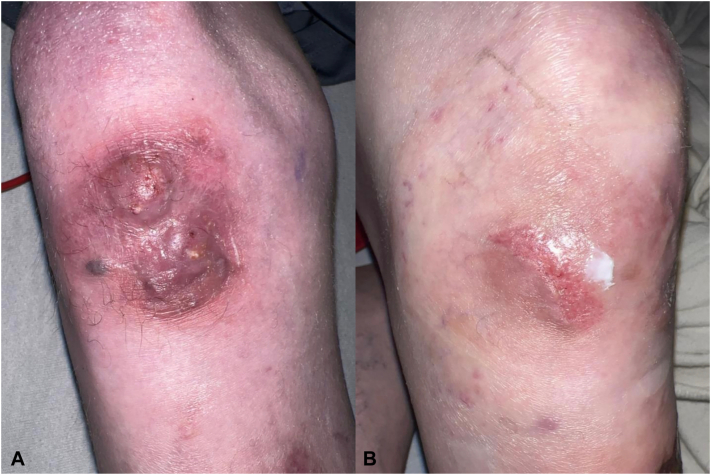 Figure 1
Figure 1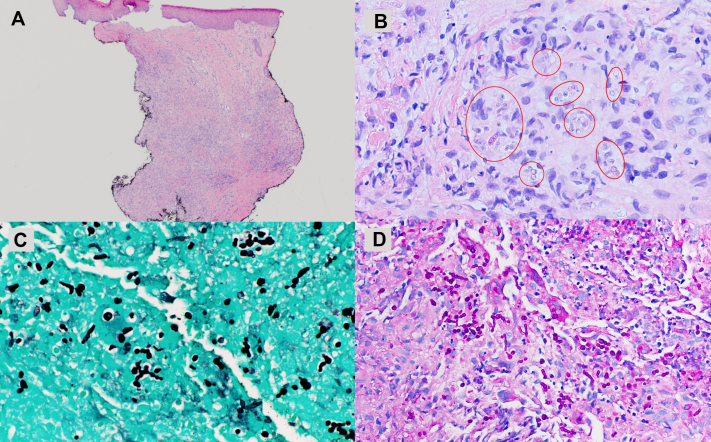 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Cancer and Skin Lesions
Introduction
Coelomycetes are an artificial taxonomic group of filamentous fungi defined by phenotypic rather than genetic characteristics, producing conidia within fruiting bodies.1 Once considered environmental saprophytes, several coelomycetes, including the dermatologic pathogen Neoscytalidium,2 are now recognized as rare opportunistic human pathogens.3^,^4 Within this group, Microsphaeropsis arundinis and Paraconiothyrium cyclothyrioides are distinct species that exhibit similar clinical and morphologic features, making species-level distinction challenging even with molecular diagnostic methods.2^,^5
Human infections with coelomycetous fungi typically result from traumatic implantation, such as minor abrasions or gardening injuries, with exposure to contaminated soil.4^,^5 Because of their saprophytic origin and nondistinct morphology, infections by M arundinis/P cyclothyrioides are frequently misdiagnosed,6^,^7 delaying appropriate antifungal therapy.
Given these diagnostic and therapeutic challenges, infections with M arundinis/P cyclothyrioides require high clinical suspicion in immunosuppressed patients with nonhealing wounds. This case underscores the need for improved fungal identification tools and targeted treatment protocols.
Case report
A 22-year-old man with hypoplastic left heart syndrome, postheart transplant (2017), Fontan-associated liver disease, and malnutrition from protein-losing enteropathy was admitted in July 2024 for protein-losing enteropathy management. Shortly after admission, he experienced right lower limb cellulitis, which he attributed to a superficial scrape sustained while playing soccer. Initially presumed bacterial, the infection was treated with intravenous vancomycin (500 mg every 6 hours for 10 days) and mupirocin ointment twice daily for 5 days. Despite this, symptoms worsened, with increased pain, marked erythema, and 3+ pitting edema of the lower portion of the leg.
The patient exhibited signs of shock, requiring intensive care. Blood cultures were negative. Although systemic symptoms stabilized with supportive care, the knee lesion progressed to a tender erythematous-violaceous plaque with erosion and intermittent purulent drainage (Fig 1, A).Fig 1**(A)** On initial evaluation, the patient presented with a 3 × 3 cm erythematous, violaceous, and nodular plaque on the right knee that exhibited intermittent purulent drainage. (B) Clinical appearance after 5 months of posaconazole treatment. The lesion regressed, with scar formation and no signs of active infection.
Infectious disease and dermatology consultations prompted wound culture and skin biopsy. Given the Arizona location, differential diagnoses included atypical mycobacteria, blastomycosis, sporotrichosis, cutaneous leishmaniasis, and other deep fungal infections. Culture morphology was consistent with a dematiaceous mold. Histologic examination revealed a flattened epidermis with underlying dermal scarring and acute and chronic granulomatous inflammation composed of histiocytic aggregates, lymphocytes, and neutrophils (Fig 2, A). Cluster of differentiation 1a immunostaining was negative for leishmaniasis, and acid-fast bacilli and Gram stains were negative for acid-fast bacilli and bacteria, respectively. Hematoxylin and eosin sections revealed abundant hyphae and budding yeasts lacking distinct morphologic features or pigmentation (Fig 2, B), prompting Grocott methenamine silver and periodic acid–Schiff stains, which confirmed the presence of fungal elements (Fig 2, C, D). Fontana–Masson was negative for pigment in tissue, supporting classification as hyalohyphomycosis.Fig 2**(A)** Punch biopsy of right knee shows diffuse inflammatory process sparing epidermis and papillary dermis (hematoxylin and eosin stain, 1.25×). (B) At medium power, note the presence of a mixed chronic granulomatous inflammatory infiltrate with histiocytes, lymphocytes, and neutrophils. Microorganisms, possibly fungal forms, are visible on hematoxylin and eosin and indicated by circles (hematoxylin and eosin stain, 10×). (C) Grocott methenamine silver stain and (D) periodic acid–Schiff stain both highlight numerous septate hyphae and budding yeast forms within the dermis (Grocott methenamine silver stain, 60× oil; periodic acid–Schiff stain, 60× oil).
The patient was started on intravenous liposomal amphotericin B (150 mg), but the lesion remained unchanged after several days. Matrix-assisted laser desorption/ionization time-of-flight on culture and 16S ribosomal DNA analysis with reflex next-generation sequencing on tissue identified coelomycetous fungi related to M arundinis or P cyclothyrioides. Following susceptibility testing, treatment was changed to oral posaconazole.
The lesion gradually regressed and showed marked improvement (Fig 1, B), with no fluctuance, drainage, induration, or new lesions. Prolonged antifungal therapy was advised.
Discussion
Cutaneous M arundinis/P cyclothyrioides infections are exceedingly rare and often misdiagnosed as bacterial cellulitis, squamous cell carcinoma, or other chronic dermatoses.3^,^5 Reported cases predominantly occur in immunocompromised patients, particularly those receiving corticosteroid therapy, solid organ transplant recipients, and patients with chronic illnesses such as diabetes and autoimmune diseases.1^,^4^,^5^,^7 Infections commonly follow traumatic implantation, with plaques and nodules appearing on the hands, legs, or feet.4^,^5 In our case, the lesion developed from a wound contaminated with soil. Initial misdiagnosis led to a prolonged course of ineffective antibiotic treatment, highlighting diagnostic challenges of rare fungal infections.
In reported cases of M arundinis/P cyclothyrioides infections, histopathologic findings often include granulomatous inflammation with multinucleated giant cells, epithelioid histiocytes, neutrophils, and lymphocytes in the dermis.1^,^6^,^8 Fungal cultures typically show mold growth within 1 to 3 weeks, with colonies that darken with age and produce chains of smaller yeast-like cells and septate hyphae with swollen segments and distinguishable flask-shaped conidiomata containing elongated conidia.5^,^9 Our case revealed a similar granulomatous inflammation, along with septate hyphae and budding yeast. Although coelomycetous fungi are typically classified as phaeohyphomycotic given their ability to pigment in both culture and tissue, our case demonstrated pigmentation only in culture, and Fontana–Masson staining was negative for melanin, confirming classification as hyalohyphomycosis.
Because of the nonspecific morphology of the fungal structures, definitive identification, as in prior reports, required advanced techniques.5^,^6^,^8^,^9 Sequencing and matrix-assisted laser desorption/ionization time-of-flight narrowed the organism to M arundinis or P cyclothyrioides, but close genetic similarity prevented species-level distinction; therefore, they are addressed collectively. Prior studies demonstrate that internal transcribed spacer sequencing alone is often insufficient to differentiate these species due to high sequence homology. Supplementary sequencing of β-tubulin or actin genes is typically required for definitive identification.10 However, this level of sequencing is rarely available in routine clinical laboratories. Given their similar antifungal susceptibilities and treatment responses, distinguishing between the 2 may be of limited clinical significance.
The complexities of M arundinis/P cyclothyrioides infections are further compounded by their variable antifungal susceptibility across antifungal agents. In our patient, no improvement was noted with amphotericin B, whereas clinical response was achieved following transition to posaconazole. Previous reports have shown that M arundinis/P cyclothyrioides are responsive to posaconazole and terbinafine, but more resistant to itraconazole and voriconazole.2^,^3^,^6^,^8^,^10 Prolonged antifungal therapy is recommended to prevent recurrence and achieve complete resolution.
Regarding additional laboratory testing, matrix-assisted laser desorption/ionization time-of-flight offers faster results but is limited to material obtained from fungal culture, which typically requires weeks to grow. In contrast, 16S ribosomal DNA analysis with reflex next-generation sequencing can be performed on culture material or paraffin-embedded biopsy tissue. Although its processing time is longer, tissue preparation for histopathology is significantly faster than fungal culture, resulting in comparable overall turnaround times. In our case, the 16S ribosomal DNA analysis with reflex next-generation sequencing results were received first.
Conclusion
This case underscores the importance of considering rare fungal pathogens, including M arundinis/P cyclothyrioides, in chronic, nonhealing wounds of immunosuppressed patients. Increased awareness and early fungal-specific diagnostics are crucial to improving outcomes and preventing misdiagnosis. Further studies on antifungal susceptibility and long-term management are warranted to optimize care for future patients facing similar infections.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asahina A.Kobayashi M.Nakano K.Deep cutaneous infection with Microsphaeropsis arundinis: report of two Japanese cases Acta Derm Venereol 957201585585710.2340/00015555-209125758776 · doi ↗ · pubmed ↗
- 2Valenzuela-Lopez N.Sutton D.A.Cano-Lira J.F.Coelomycetous fungi in the clinical setting: morphological convergence and cryptic diversity J Clin Microbiol 552201755256710.1128/JCM.02221-1627927918 PMC 5277526 · doi ↗ · pubmed ↗
- 3Hall M.R.Brumble L.M.Mayes M.A.Snow J.L.Keeling J.H.Cutaneous Microsphaeropsis arundinis infection initially interpreted as squamous cell carcinoma Int J Dermatol 5212013848610.1111/j.1365-4632.2010.04808.x 23278613 · doi ↗ · pubmed ↗
- 4Hamed A.Bosshardt Hughes O.Palavecino E.L.Jakharia N.Cutaneous infection caused by Paraconiothyrium cyclothyrioides in a renal transplant recipient Transpl Infect Dis 2342021 e 1362410.1111/tid.1362433884728 · doi ↗ · pubmed ↗
- 5Crawford S.J.Chen S.C.A.Halliday C.Rangan G.K.Gottlieb T.Reid A.B.Microsphaeropsis arundinis skin and soft tissue infection in renal transplant recipients: three case reports and a review of the literature Transpl Infect Dis 176201591592010.1111/tid.1246426437250 · doi ↗ · pubmed ↗
- 6Choi H.Kim C.J.Kim M.S.Shin B.S.Na C.H.A case of subcutaneous and intranasal phaeohyphomycosis caused by Microsphaeropsis arundinis in an immunocompromised patient misdiagnosed with mucormycosis Ann Dermatol 315201957157510.5021/ad.2019.31.5.57133911652 PMC 7992564 · doi ↗ · pubmed ↗
- 7Ferrándiz-Pulido C.Martin-Gomez M.T.Repiso T.Cutaneous infections by dematiaceous opportunistic fungi: diagnosis and management in 11 solid organ transplant recipients Mycoses 622201912112710.1111/myc.1285330230044 · doi ↗ · pubmed ↗
- 8Nguyen Y.Dodds T.Lowe P.Cutaneous Microsphaeropsis arundinis infection in renal transplant recipients-a report of 2 cases and review of the literature JAAD Case Rep 45201841541710.1016/j.jdcr.2017.11.01229984267 PMC 6031487 · doi ↗ · pubmed ↗