Sézary syndrome presenting as vitiligo-like leukoderma with response and repigmentation to mogamulizumab and extracorporeal photopheresis
Elizabeth Anderson, Jordyn Puccio, Eric Mou, Brian Swick, Vincent Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
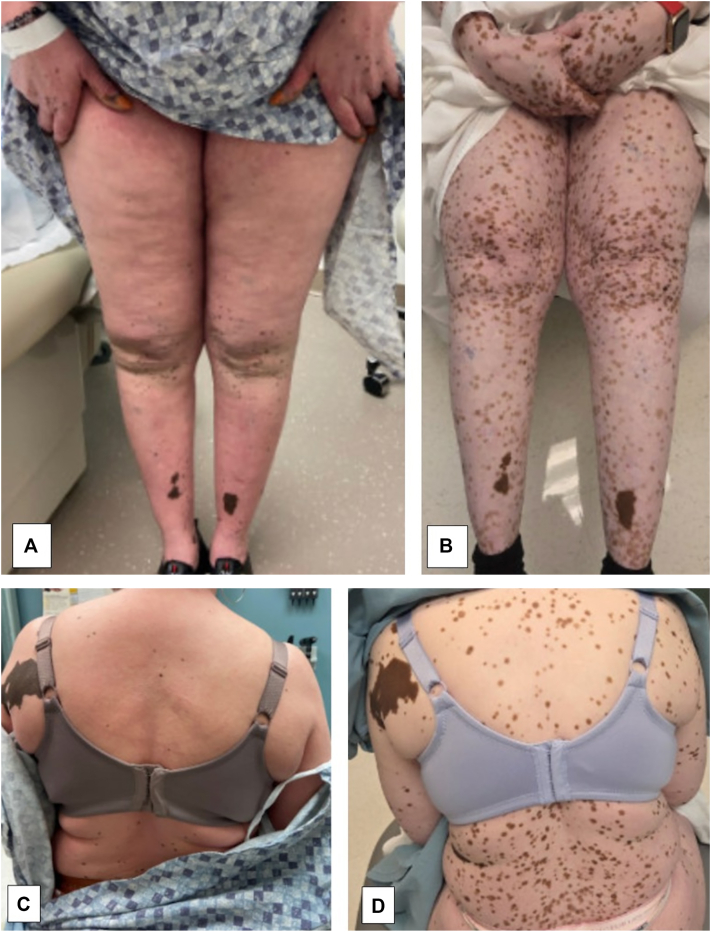 Figure 1
Figure 1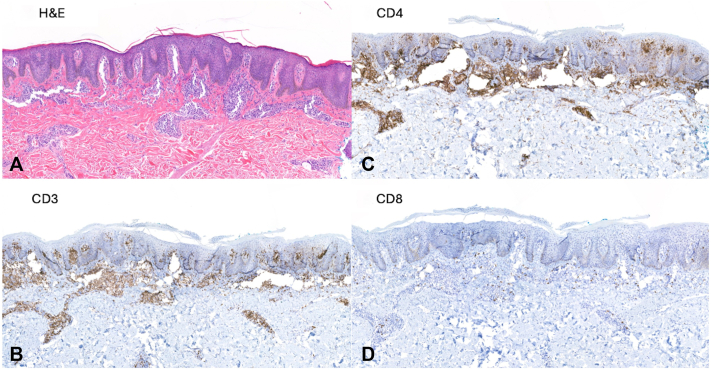 Figure 2
Figure 2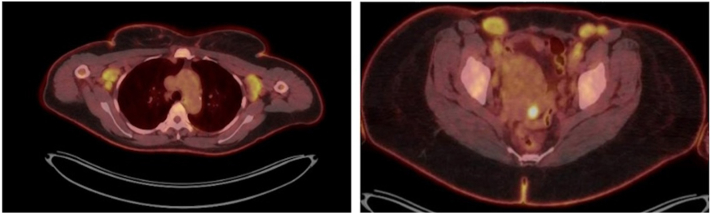 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsmelanin and skin pigmentation · Cutaneous lymphoproliferative disorders research · Chronic Lymphocytic Leukemia Research
Introduction
Cutaneous T-cell lymphomas (CTCLs) are extranodal non-Hodgkin lymphomas localized to the skin.1 Mycosis fungoides and Sezary syndrome (SS) are the most common types of CTCL, accounting for approximately two-thirds of all diagnosed cases of CTCL annually.2 Sezary syndrome, characterized by systemic dissemination of leukemic cells, classically presents as generalized erythroderma with lymphadenopathy but is notorious for its protean cutaneous manifestations.1^,^2 Diagnosis can be challenging, requiring the integration of clinical presentation, histopathology, immunopathology, and molecular evaluation for T-cell clonality.1 Treatment is stage-dependent and spans the spectrum of skin-directed to systemic therapies, the latter including retinoids, interferon, chemotherapy, and histone deacetylase inhibitors, as well as newer agents such as mogamulizumab (monoclonal antibody targeting C-C chemokine receptor 4 [CCR4]) and brentuximab vedotin (anti-CD30 monoclonal antibody-drug conjugate).2, 3, 4 CTCL-associated vitiligo-like leukoderma is a particularly rare manifestation, for which the optimal treatment regimen is unclear (Table I).5, 6, 7, 8, 9 Herein, we describe a patient with a striking example of this presentation, its associated challenges in diagnosis, and an excellent response to extracorporeal photopheresis (ECP) with mogamulizumab.Table IA summary of the reported cases of vitiligo-like leukoderma in setting of CTCLFirst author (y)Age, sexClinical descriptionClinical diagnosis, stageTreatmentOutcomeAlcalay, 1987562, MaleErythroderma, lymphadenopathy, muscle wasting, depigmentationSezary syndromeTopical and systemic steroids, chlorambucilStable diseaseBouloc, 2000683, FemaleErythroderma, pruritus, poikiloderma, lymphadenopathy, depigmented patchesSezary syndromeTopical and systemic steroids, topical mechlorethamine, systemic chlorambucilPartial response65, FemaleErythroderma, pruritus, lymphadenopathy, depigmented patchesSezary syndromeTopical and systemic steroids, topical mechlorethamine, retinoids, PUVA, interferon-alfa2, methotrexate, chlorambucil, cytopheresis, total-body electron beam therapy.Partial response65, MaleErythroderma, depigmented patchesErythrodermic MFTopical and systemic steroids, topical mechlorethamine, PUVA, chlorambucil, methotrexateComplete response63, MalePsoriasiform plaques progressed to erythroderma, pruritus, lymphadenopathy, depigmented patchesErythrodermic MFTopical mechlorethamineComplete responseMacheiner, 2003750, MaleErythroderma, pruritus, lymphadenopathy, splenomegaly, symmetric polyarthritisSezary syndromeTopical and systemic steroids, PUVA, localized radiation, vinblastine, cyclophosphamide, chlorambucil, ECPProgression of diseaseKnol, 2005871, FemaleErythroderma, pruritus, depigmented patchesSezary syndromeInterferon-alfa2 + PUVA, acitretinStable diseaseMirza, 2024462, MaleErythroderma, hyperkeratosis of feet, lymphadenopathy, depigmentation with leukotrichiaSezary syndromeT4 N3 B1 M0MogamulizumabPartial responseAnderson, (current patient)57, FemaleErythroderma, pruritus, lymphadenopathy, depigmented patchesSezary SyndromeT4 N3 B1 M0ECPMogamulizumabPartial responseCTCL, Cutaneous T-cell lymphoma; ECP, extracorporeal photopheresis; MF, mycosis fungoides; PUVA, psoralen + UVA phototherapy.
Case presentation
A 57-year-old Caribbean-American female presented with presumed vitiligo. She was referred to dermatology for rash, pruritus, and hypopigmentation, which developed following COVID-19 vaccination. The hypopigmentation began on the face and hands and subsequently spread diffusely, affecting over 80% of the body surface area, with some retention of perifollicular pigmentation (Fig 1). Additionally, a complete blood count demonstrated an absolute lymphocytosis initially felt to be reactive. Several initial skin biopsies showed postinflammatory hypopigmentation with spongiotic and psoriasiform dermatitis. She was treated with topical steroids, phototherapy, and methotrexate for presumed severe atopic dermatitis and concomitant vitiligo but witnessed no clinical improvement.Fig 1. Pigmentation (A and C) while being treated with methotrexate and (B and D) while being treated with ECP and mogamulizumab. ECP, Extracorporeal photopheresis.
Given her minimal response to treatment, further evaluation of her lymphocytosis was undertaken. Laboratory evaluation revealed white blood count 14.2 k/mm3 (normal range: 3.7- 10.5) with absolute lymphocyte count of 7652 cells/mm3 (normal range: 875-3300), lactate dehydrogenase 439 U/L (normal range: 135-214), and human T-lymphotropic virus-type 1 and 2 antibody negative. Peripheral blood flow cytometry identified a monoclonal lymphoid population of CD4+, CD3+, CD5+, CD7 partial positive, and CD26 mostly negative cells, and T-cell gene rearrangement studies by polymerase chain reaction were positive, consistent with SS. The clonal population measured 4960 cells/mm3, qualifying as B2 staging. Subsequent cutaneous biopsies showed psoriasiform dermatitis with a monoclonal CD4-positive epidermotropic lymphoid proliferation (Fig 2). SOX10 immunohistochemical staining was absent within the epidermis, consistent with vitiligo in the background of CTCL. Positron emission tomography/computed tomography (PET/CT) imaging demonstrated multiple fluorodeoxyglucose (radioactive sugar tracer used in PET scans) (FDG)-avid enlarged axillary (largest: left axillary node 4.7 × 2.3 cm, standardized uptake value max 5.3) and inguinal lymph nodes (largest: right inguinal node 3.4 × 2.3 cm, standardized uptake value max 5.3) (Fig 3). A follow-up lymph node biopsy of the right inguinal node showed architectural effacement by a monoclonal CD4+, CD7-lymphoid proliferation, consistent with lymphomatous involvement. T-cell gene rearrangement studies on skin, blood, and lymph node all showed matching monoclonal peaks, overall consistent with a diagnosis of SS, stage IVA_2_ (T4N3bM0B2b).Fig 2. Skin biopsy from left shoulder depigmented patch, showing (A) psoriasiform epidermal hyperplasia with associated epidermotropic atypical lymphocytic infiltrate [H&E; 86×], comprised by (B) predominant T-lymphocytes [CD3; 73×], the majority of which are shown to represent (C) CD4-positive helper T-cells [CD4; 69×] with admixed (D) minority CD8-positive cytotoxic/suppressor T-cells [CD8; 79×].Fig 3. Initial whole-body positron emission tomography/computed tomography showing multiple fluorodeoxyglucose-avid enlarged bilateral axillary (left) and inguinal (right) lymph nodes, suggestive of lymphomatous involvement. The dominant right inguinal lymph node, measuring 3.4 × 2.3 cm, was subsequently biopsied, showing florid lymphomatous involvement (N3).
She began monthly ECP treatments and mogamulizumab. After 3 cycles of therapy, there was improvement in the degree of erythroderma and pruritus, and her skin began slowly repigmenting. Interval peripheral blood flow cytometry showed complete resolution of her clonal lymphocytosis. Interim PET/CT showed decreasing size of her axillary and inguinal lymph nodes, with no new nodal growth. After completing 6 cycles of ECP + mogamulizumab, her pruritus remained resolved, as did her peripheral blood lymphocytosis. PET/CT showed quiescence of cutaneous disease but persistent FDG-avid bilateral axillary and inguinal lymphadenopathy. An axillary lymph node was rebiopsied, showing reactive lymphoid hyperplasia, consistent with dermatopathic lymphadenopathy. To date, she has continued combination therapy for over 1 year with an ongoing excellent response.
Discussion
Although CTCL can manifest within a spectrum of pigmentation morphologies, few cases of CTCL presenting as vitiligo have been reported in the literature, as reviewed in Table I.5, 6, 7, 8, 9 These cases demonstrate the heterogeneity in both clinical presentation and applied therapies to patients with vitiligo-like leukoderma and highlight the absence of a consensus approach to this striking phenomenon.
Whether the initial depigmentation represents a true manifestation of early SS or authentic vitiligo as a precursor paraneoplastic epiphenomenon is challenging to definitively discern. Several mechanisms have been proposed to explain this immune-mediated depigmentation; vitiligo in the setting of CTCL is thought to result from destruction of epidermal melanocytes by tumoral lymphocytes, reactive T lymphocytes, or T-cell-activated B-cell-mediated autoantibodies.7 It has been hypothesized that since both CTCL and vitiligo involve abnormal immune activity, the dysfunctional T-cell activity in CTCL may predispose patients to melanocyte destruction.7^,^9 For example, patients with CTCL and vitiligo have been found to harbor subpopulations of CD8+ T cells reactive to MART-1 in their lesional tissue.9 The leading hypothesis proposes that malignant or reactive T-cells directly attack melanocytes after infiltrating the skin through pathways that normally recruit T-cells, utilizing cutaneous lymphocyte antigen and chemokine receptors such as CCR4.5^,^9^,^10
Our case and an additional case presented by Mirza et al showed benefit in repigmentation of leukodermic patches with the use of mogamulizumab, as seen in Fig 1.5 Mogamulizumab is a monoclonal antibody targeting CCR4, which is present on T-cells and consistently expressed by Sézary cells.3 Targeting CCR4 leads to antibody-dependent cellular cytotoxicity.3 In both cases, leukodermic patches were present prior to the initiation of treatment with mogamulizumab and improved after treatment.5 This suggests that mogamulizumab may treat both the cutaneous lymphoma and the vitiligo-like leukoderma. Of note, mogamulizumab has been associated with the onset of vitiligo after treatment initiation.10 While the pathogenesis is not entirely established, it is currently hypothesized that the loss of Treg cells leads to decreased immune tolerance and subsequently increased autoimmunity.10 Given our suggestion that mogamulizumab may be beneficial in improving dyspigmentation, more research is required to understand the interactions between mogamulizumab, the immune system, and melanocytes.
In conclusion, CTCL-induced vitiligo is rare and poorly understood. It is important for dermatologists to be aware of the various presentations of CTCL, including vitiligo, to limit delay in diagnosis. Further research is needed to better understand the mechanisms underlying the concomitant diagnoses of CTCL and associated vitiligo-like leukoderma and to optimize management of both the cutaneous lymphoma and skin dyspigmentation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Olsen E.A.Whittaker S.Willemze R.Primary cutaneous lymphoma: recommendations for clinical trial design and staging update from the ISCL, USCLC, and EORTC Blood 1405202241943710.1182/blood.202101205734758074 PMC 9353153 · doi ↗ · pubmed ↗
- 2Kim Y.H.Bagot M.Pinter-Brown L.MAVORIC Investigators Mogamulizumab versus vorinostat in previously treated cutaneous T-cell lymphoma (MAVORIC): an international, open-label, randomised, controlled phase 3 trial Lancet Oncol 19920181192120410.1016/S 1470-2045(18)30379-6Erratum in: Lancet Oncol. 2018 Nov;19(11):e 581. https://doi.org/10.1016/S 1470-2045(18)30772-130100375 · doi ↗ · pubmed ↗
- 3Prince H.M.Kim Y.H.Horwitz S.M.ALCANZA study group ALCANZA study group. Brentuximab vedotin or physician's choice in CD 30-positive cutaneous T-cell lymphoma (ALCANZA): an international, open-label, randomised, phase 3, multicentre trial Lancet 39010094201755556610.1016/S 0140-6736(17)31266-728600132 · doi ↗ · pubmed ↗
- 4Mirza F.N.Olszewski A.J.Pelcovits A.R.Di Marco C.Firoz E.F.Sézary syndrome associated vitiligo-like leukoderma in type V skin: report of a case and review of the literature JAAD Case Rep 48202410310710.1016/j.jdcr.2024.04.00938813064 PMC 11134528 · doi ↗ · pubmed ↗
- 5Alcalay J.David M.Shohat B.Sandbank M.Generalized vitiligo following Sézary syndrome Br J Dermatol 11661987851855362034510.1111/j.1365-2133.1987.tb 04904.x · doi ↗ · pubmed ↗
- 6Bouloc A.Grange F.Delfau Larue M.H.Leucoderma associated with flares of erythrodermic cutaneous T-cell lymphomas: four cases. The French Study Group of Cutaneous Lymphomas Br J Dermatol 143420008328361106946610.1046/j.1365-2133.2000.03851.x · doi ↗ · pubmed ↗
- 7Macheiner W.Jantschitsch C.Graninger W.Sézary syndrome and seronegative polyarthritis: treatment with extracorporeal photochemotherapy J Am Acad Dermatol 482200322022610.1067/mjd.2003.1112582392 · doi ↗ · pubmed ↗
- 8Knol A.C.Quéreux G.Marques-Briand S.Pathogenetic mechanisms of vitiligo in a patient with Sézary syndrome Br J Dermatol 15362005120712121630766010.1111/j.1365-2133.2005.06877.x · doi ↗ · pubmed ↗