Atrial Fibrillation/Flutter in Transthyretin Cardiac Amyloidosis: Prevalence, Incidence, Clinical Predictors, and Effect of Tafamidis
Nicholas Chan, Yevgeniy Brailovsky, Sergio Teruya, Alfonsina Mirabal, Ariel Y. Weinsaft, Jeffeny De Los Santos, Samantha Guadalupe, Massiel Jimenez, Stephen Helmke, Margaret Cuomo, Dia Smiley, Angelo Biviano, Jose Dizon, Elaine Wan, Hirad Yarmohammadi, Mathew S. Maurer

TL;DR
This study finds that over half of patients with a specific heart condition have atrial fibrillation, which is linked to disease severity and a drug called tafamidis may help prevent it.
Contribution
The study identifies new predictors of atrial fibrillation in transthyretin cardiac amyloidosis and evaluates the protective effect of tafamidis.
Findings
Atrial fibrillation was present in 58% of patients with transthyretin cardiac amyloidosis at baseline.
Higher Columbia score and left atrial volume index were associated with prevalent atrial fibrillation.
Tafamidis and hereditary amyloid transthyretin were protective against new-onset atrial fibrillation.
Abstract
Atrial fibrillation/flutter (AF) is common in transthyretin cardiac amyloidosis (ATTR-CA). The CHARGE-AF score has not been validated in ATTR-CA. The Columbia staging system is prognostic for survival, but its utility in predicting incident AF is unknown. The authors aim to determine the predictors of prevalence and incidence of AF and the effect of tafamidis. This is a retrospective cohort study of 419 patients with ATTR-CA. AF was ascertained from review of electrocardiograms, extended rhythm, device interrogations, and charted history. Binary logistic regression assessed for factors associated with prevalent AF. Cox regression time-to-event analysis assessed for factors associated with incident AF. AF was present in 58% (n = 244) of ATTR-CA at baseline. On multivariable logistic regression, higher Columbia score (OR: 1.48; 95% CI: 1.25-1.75) and higher left atrial volume index…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
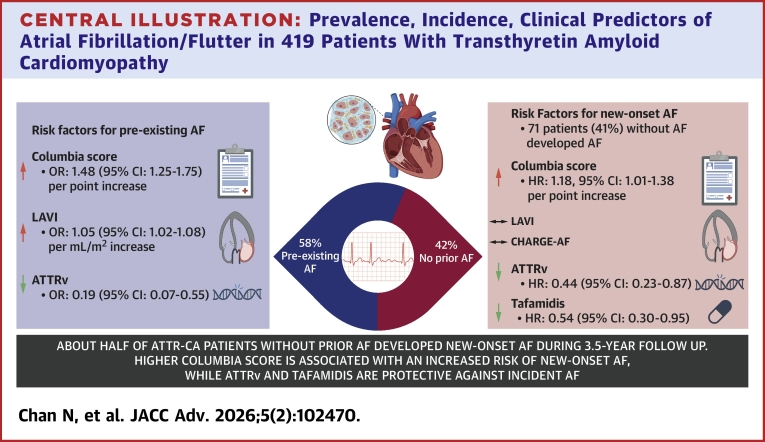 Figure 1
Figure 1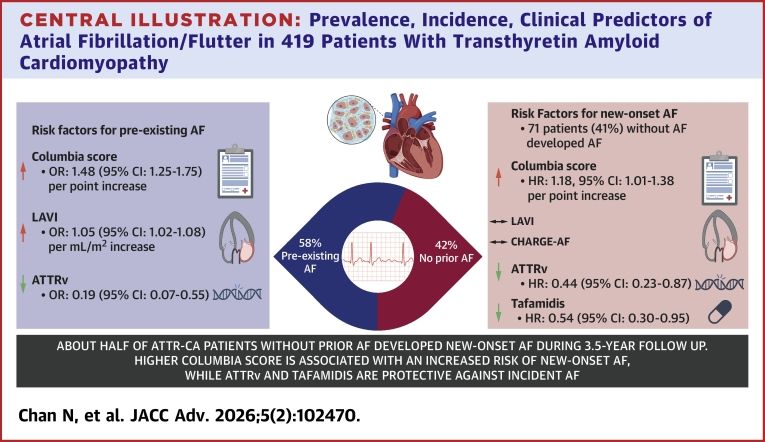 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Parathyroid Disorders and Treatments · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Transthyretin cardiac amyloidosis (ATTR-CA) is an underappreciated etiology of diastolic heart failure in the older adult population. This form of restrictive cardiomyopathy is caused by degeneration of the normal tetrameric transthyretin protein complex from either aging (wild-type amyloid transthyretin [ATTRwt]) or inherited mutations (hereditary amyloid transthyretin [ATTRv]), which generates monomers that coalesce into insoluble, misfolded protein fibrils and subsequently deposit in tissues.1 Progressive infiltration of cardiomyocytes by amyloid fibrils in both atria and ventricles results in adverse chamber remodeling and fibrosis that potentiates development of tachyarrhythmias such as atrial fibrillation/flutter (AF), which have been observed in 48% to 88% in ATTR-CA cohorts.2, 3, 4, 5
Managing AF in ATTR-CA is challenging due to a lower rate of successful electrical cardioversion,6^,^7 and catheter ablation. Prior studies had conflicting results with regards to both safety/periprocedural complications and efficacy,3^,^7^,^8 with concerns of high chances for arrhythmia recurrence. However, greater success rates of rhythm control strategies seemed to be observed in earlier stage disease.5^,^9^,^10 Moreover, thromboembolic events represent major concerns as amyloid-mediated atrial mechanical dysfunction increases the risk of intracardiac thrombosis/systemic embolism4 and warrants timely initiation of prophylactic pharmacotherapy for stroke regardless of CHA_2_DS_2_Vasc Score.11
In light of these clinical considerations, there is growing interest in the role of clinical prediction models for early identification of ATTR-CA subjects with increased likelihood of having pre-existing or new onset AF. Prompt risk stratification can help determine which patients need more intensive surveillance for incident AF and timely initiation of appropriate anticoagulation. The CHARGE-AF score, previously derived from the general population,12^,^13 has not been validated in ATTR-CA. The Columbia staging system is prognostic for survival,14 but its utility in predicting incident AF is not known. Furthermore, the effect of disease-modifying therapy on the development of incident AF is unclear. The purpose of our study is multifold: 1) determine the prevalence, phenotypic characteristics, and relevant factors associated with pre-existing AF in ATTR-CA patients on presentation; 2) evaluate the incidence and clinical predictors for incident AF in ATTR-CA during follow-up, including the utility of CHARGE-AF score and Columbia staging system; 3) determine whether disease-modifying therapy with tafamidis delays the onset of incident AF.
Methods
This is a single-center retrospective observational cohort study of 419 patients diagnosed with ATTR-CA from 2001 to 2021, with approval by the Institutional Review Board. Diagnosis of ATTR-CA was made by either endomyocardial biopsy or technetium pyrophosphate scan per the American Society of Nuclear Cardiology guidelines.15^,^16 Light chain amyloidosis was excluded by the absence of detectable monoclonal protein on serum and urine immunofixation electrophoresis, as well as normal serum-free light chain assay results, or biopsy.
The study cohort was first stratified into individuals with and without AF at baseline, as ascertained based on review of prior electrocardiograms (ECG), extended rhythm monitoring if performed, device interrogations when applicable, and documented history. For each of these 2 groups of subjects, baseline variables, including demographics, comorbidities, medications, implanted devices, vital signs, laboratory results, and echocardiographic measurements from standard clinical protocols, were collected on initial presentation. Hypertension, diabetes, coronary artery disease, myocardial infarction, stroke/transient ischemic attack, and smoking were based on charted history. Chronic kidney disease (CKD) was confirmed by history and an estimated glomerular filtration rate <60 mL/min/m^2^ per the modified diet in renal disease equation.
For cardiac biomarkers, when needed, high sensitivity troponin T and B-type natriuretic peptide were converted as follows: troponin T = hsTnT/1,000; NT-proBNP = BNP × 6, as we have performed previously.14 Staging of disease, which has prognostic implications on mortality, were determined as per previously established definitions (Supplemental Table 1).14^,^17^,^18 Left ventricular chamber dimensions and volumes (including stroke volume) as well as left ventricular mass and cardiac output were all indexed to body surface area. Myocardial contraction fraction was the ratio of left ventricular stroke volume to myocardial volume.19^,^20 Binary logistic (see statistical analysis section) was performed for the outcome of prevalent AF.
From the subcohort of individuals without any AF prior on initial presentation, we then identified which of these patients developed de novo AF on subsequent follow-up. The presence of incident AF was ascertained from review of charted history, ECGs, extended rhythm monitoring, and device interrogations. Clinical characteristics were compared between those with and without new onset AF, which was ascertained by the same methodology described previously. We also calculated each subject’s CHARGE-AF score (Supplemental Table 2) and recorded whether tafamidis was prescribed during any time point of these patients’ disease courses. Time-to-event analysis (see statistical analysis section) was performed for the endpoint of incident AF.
Statistical analysis
Continuous variables were reported as medians with IQRs, whereas categorical variables were reported as number of patients followed by percentages. The differences in characteristics among groups were assessed by the Kruskal-Wallis test for continuous dependent variables and chi-Square test (or Fisher exact test) for nominal dependent variables.
Binary logistic regression was performed to determine factors associated with prevalent AF. Covariates were selected a priori to include age, race, ATTR genotype, cardiac amyloidosis staging, and left atrial (LA) volume index (LAVI), whereby all variables with P values <0.10 on univariable analysis were then entered into the multivariable model.
For incident AF, the date of initial presentation was defined as the beginning of the follow-up period. The end follow-up date was defined as the last date of clinical contact, death/heart transplant, or AF occurrence, whichever occurs first, as of September 30, 2022. Time-to-event analysis, with censoring after 5-years of follow-up, was performed using Cox proportional hazard modeling to assess the effects of relevant factors on the development of new onset AF. Covariates were selected a priori based on their clinical relevance, to include CHARGE-AF score (which already incorporates age and race), gender, ATTR genotype, cardiac amyloidosis staging, LAVI, and tafamidis use. All variables with P values <0.10 in the univariable analysis were included in the multivariable model. All statistical tests were 2-sided, with a significance level set at α = 0.05. All statistical analyses were completed in IBM SPSS Statistics (version 28) (2021).
To test the proportional hazards (PHs) assumption, time-dependent covariates (as interaction terms between each covariate and the log of time) were added to the original Cox PH model and found nonsignificant P values (P > 0.05) for all the time interaction terms. In addition, a supremum test and cumulative Martingale residuals (based on Schoenfeld residuals) further tested the PH assumption of the continuous covariates. The supremum test showed P values of 0.13 and 0.55 for the Columbia score and LAVI respectively, and the cumulative Martingale residuals plots did not show any trend over time, demonstrating that the PH assumption was held. Collinearity was not found; the highest variance inflation factor found was for the ATTRv variable, 1.3 (>10 suggests collinearity) and condition indices (CIs) were all below 16 (>30 suggests collinearity).
Results
Among the 419 study subjects, 175 (42%) had no prior AF, whereas 244 (58%) had pre-existing AF (prevalent AF cohort) (Table 1). Compared to the no AF group, the prevalent AF cohort was older (78 years vs 74 years), had more individuals of White race (84.0% vs 68.6%), but fewer of Hispanic ethnicity (2.5% vs 7.4%) and fewer with ATTRv (13.1% vs 39.4%). Those with prevalent AF had more advanced NYHA functional class (III to IV symptoms of 48.7% vs 33.8%), prior stroke/transient ischemic attack (14.8% vs 5.7%), CKD (65.6% vs 44.6%), and need for diuretic agents (82.0% vs 65.7%). The median follow-up for the no baseline AF cohort is 3.58 (95% CI: 2.86-4.20) years. As expected, those with prevalent AF were more frequently treated with various antiarrhythmic medications and anticoagulation (and less frequently on aspirin). Labs show that the prevalent AF group had worse renal function and N-terminal pro–B-type natriuretic peptide levels than the no AF cohort. The cohort with AF at baseline also had greater proportion of individuals having intermediate to advanced (stage II to III) disease, per National Amyloidosis Centre (NAC) (47.1% vs 31.6%) and Columbia (70.3% vs 48.9%) staging systems. Echocardiographic features were similar between the 2 groups, except that the prevalent AF group had greater LA diameter (4.7 cm vs 4.4 cm) and LAVI (48.1 mL/m^2^ vs 40.9 mL/m^2^).Table 1. Baseline Characteristics of Study Cohort (N = 419)nNo AF (n = 175, 42%)nPrevalent AF (n = 244, 58%)P ValueDemographics Age, y17574 (68, 79)24478 (73, 82)<0.0001 Male175148 (84.6%)244215 (88.1%)0.293 White race175120 (68.6%)244205 (84.0%)<0.0001 ATTRv17569 (39.4%)24432 (13.1%)<0.0001 Hispanic ethnicity17513 (7.4%)2446 (2.5%)0.016 Body mass index, kg/m^2^17426.2 (23.8, 28.7)24426.5 (24.1, 29.7)0.283 NYHA functional class175244<0.0001 I28 (16.0%)14 (5.7%) II88 (50.3%)111 (45.5%) III54 (30.9%)114 (46.7%) IV5 (2.9%)5 (2.0%)Comorbidities Hypertension17591 (52.0%)244125 (51.2%)0.876 Diabetes17518 (10.3%)24430 (12.3%)0.524 CAD17552 (29.7%)24492 (37.7%)0.089 MI17511 (6.3%)24418 (7.4%)0.664 Stroke/TIA17510 (5.7%)24436 (14.8%)0.004 CKD17578 (44.6%)244160 (65.6%)<0.0001 Smoking1752440.122 Active6 (3.4%)2 (0.8%) Former66 (37.7%)103 (42.2%) Never103 (58.9%)139 (57.0%)Antiarrhythmics Beta-blocker17570 (40.0%)244151 (61.9%)<0.0001 Amiodarone1753 (1.7%)24433 (13.5%)<0.0001 Dofetilide1750 (0%)2446 (2.5%)0.043 Calcium channel blockers17513 (7.4%)24421 (8.6%)0.663 Digoxin1752 (1.1%)24414 (5.7%)0.016Heart failure therapy ACEI/ARB/ARNI17564 (36.6%)24479 (32.4%)0.372 MRA17545 (25.7%)24480 (32.8%)0.119 Loop diuretic agents175115 (65.7%)244200 (82.0%)<0.0001 Thiazides17520 (11.4%)24429 (11.9%)0.886Antiplatelet ASA17591 (52.0%)24469 (28.3%)<0.0001 Clopidogrel17514 (8.0%)24413 (5.3%)0.272 Ticagrelor1750 (0%)2441 (0.4%)1.000 Prasugrel1752 (1.1%)2440 (0%)0.174 Ticlopidine1750 (0%)2441 (0.4%)1.000 Dipyridamole1750 (0%)2441 (0.4%)1.000Anticoagulation Warfarin1755 (2.9%)24472 (29.5%)<0.0001 DOAC1753 (1.7%)244140 (57.4%)<0.0001Other CV medications Statin17599 (56.6%)244148 (60.7%)0.402Devices PPM only1759 (5.1%)24439 (16.0%)<0.0001 ICD17517 (9.7%)24434 (13.9%)0.193Vitals Systolic blood pressure, mm Hg173120 (108, 130)244117 (104, 126)0.187 Diastolic blood pressure, mm Hg17370 (64, 80)24470 (60, 80)0.207 Heart rate, beats/min17373 (64, 82)24476 (65, 82)0.724Labs Creatinine (mg/dL)1751.17 (0.95, 1.45)2441.32 (1.08, 1.70)<0.0001 eGFR (mL/min/m^2^)17463 (49, 77)24453 (40, 67)<0.0001 troponin T (ng/L)1570.05 (0.03, 0.11)2200.05 (0.02, 0.10)0.682 NT-proBNP (pg/mL)1741885 (914, 4,039)2402,623 (1,748, 4,641)<0.0001Amyloidosis staging Mayo1682330.868 196 (57.1%)139 (59.7%) 240 (23.8%)51 (21.9%) 332 (19.0%)43 (18.5%) Gilmore1742400.005 1119 (68.4%)127 (52.9%) 232 (18.4%)59 (24.6%) 323 (13.2%)54 (22.5%) Columbia174239<0.0001 Stage I (1-3 points)89 (51.1%)71 (29.7%) Stage II (4-6 points)69 (39.7%)127 (53.1%) Stage III (7-9 points)16 (9.2%)41 (17.2%)Echo LVEF, %14049 (33, 55)19050 (35, 55)0.959 IVS, cm1381.7 (1.5, 1.9)1811.6 (1.4, 1.8)0.056 PWT, cm1351.6 (1.4, 1.8)1771.5 (1.3, 1.8)0.399 RWT1340.73 (0.59, 0.88)1750.70 (0.52, 0.88)0.401 LVEDDi, cm/m^2^1362.3 (2.1, 2.5)1752.3 (2.0, 2.5)0.446 LVESDi, cm/m^2^1341.8 (1.6, 2.2)1751.8 (1.5, 2.1)0.504 LVEDVi, mL/m^2^13644 (38, 54)17544 (36, 53)0.784 LVESVi, mL/m^2^13423 (17, 32)17523 (17, 31)0.769 LVSVi, mL/m^2^13420 (14, 25)17521 (16, 25)0.596 LV mass index, g/m^2^132154 (127, 191)172148 (120, 180)0.099 Cardiac index, L/min/m^2^)1331.5 (1.1, 1.8)1751.5 (1.2, 1.9)0.473 MCF, %13213 (9, 18)17314 (10, 20)0.167 LA diameter (cm)1484.4 (4.0, 4.8)2014.7 (4.2, 5.0)<0.0001 LAVI (mL/m^2^)13240.9 (34.9, 48.2)16848.1 (40.5, 56.6)<0.0001ACEI = angiotensin-converting enzyme inhibitor; AF = atrial fibrillation/flutter; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor neprilysin inhibitor; ASA = aspirin; ATTRv = hereditary amyloid transthyretin; CAD = coronary artery disease; CKD = chronic kidney disease; CV = cardiovascular; DOAC = direct oral anticoagulant; eGFR = estimated glomerular filtration rate; ICD = implantable cardioverter-defibrillator; IVS = intraventricular septal thickness; LVEDDi = left ventricular diastolic dimension index; LVEDVi = left ventricular diastolic volume index; LVESDi = left ventricular systolic dimension index; LVESVI = left ventricular stroke volume index; MCF = myocardial contraction fraction; MI = myocardial infarction; MRA = mineralocorticoid receptor antagonist; NT-proBNP = N-terminal pro–B-type natriuretic peptide; LA = left atrial; LAVI = left atrial volume index; LV = left ventricular; LVEF = left ventricular ejection fraction; PPM = permanent pacemaker; PWT = posterior wall thickness; RWT = relative all thickness; TIA = transient ischemic attack.
Binary logistic regression model for the effect of clinically relevant covariates on the presence of pre-existing AF is shown in Table 2. On multivariable analysis, Columbia score (OR: 1.48; 95% CI: 1.25-1.75; P < 0.0001, per point increase in score) and LAVI (OR: 1.05; 95% CI: 1.02-1.08; P < 0.0001, per mL/m^2^ increase) were associated with greater odds of prevalent AF, whereas ATTRv had lower odds of prevalent AF (OR: 0.19; 95% CI: 0.07-0.55; P = 0.002) when compared to ATTRwt.Table 2. Baseline Characteristics of Subjects Without Any Prior AF On Initial Presentation, Stratified by Those Who Develop and Do Not Develop Incident AF During Follow-Up (N = 175)nNo Incident AF (n = 104, 59%)nIncident AF (n = 71, 41%)P ValueDemographics Age, years10474 (66, 80)7175 (71, 79)0.505 Male10482 (78.8%)7166 (93.0%)0.011 White race10464 (61.5%)7156 (78.9%)0.015 ATTRv10451 (49.0%)7118 (25.4%)0.002 Hispanic ethnicity10411 (10.6%)712 (2.8%)0.055 Height, cm103173 (165, 178)71173 (165, 180)0.217 Weight, kg10376 (68, 85)7182 (70, 90)0.057 Body mass index, kg/m^2^10326.0 (23.4, 28.2)7126.4 (24.0, 29.7)0.233 NYHA functional class104710.022 I22 (21.2%)6 (8.5%) II47 (45.2%)41 (57.7%) II30 (28.8%)24 (33.8%) IV5 (4.8%)0 (0.0%) CHARGE-AF score10414.0 (13.2, 14.7)7114.3 (13.6, 14.8)0.064Comorbidities Hypertension10461 (58.7%)7130 (42.3%)0.033 Diabetes10412 (11.5%)716 (8.5%)0.509 CAD10433 (31.7%)7119 (26.8%)0.48 MI1047 (6.7%)714 (5.6%)1.000 Stroke/TIA1043 (2.9%)717 (9.9%)0.093 CKD10444 (42.3%)7134 (47.9%)0.466 Smoking104710.42 Active2 (1.9%)4 (5.6%) Former39 (37.5%)27 (38.0%) Never63 (60.6%)40 (56.3%)Antiarrhythmics Beta-blocker10440 (38.5%)7130 (42.3%)0.615 Amiodarone1043 (2.9%)710 (0%)0.273 Calcium channel blockers1047 (6.7%)716 (8.5%)0.67 Digoxin1041 (1.0%)711 (1.4%)1.000Heart failure therapy ACEI/ARB/ARNI10438 (36.5%)7126 (36.6%)0.991 MRA10424 (23.1%)7121 (29.6%)0.334 Loop diuretic agents10465 (62.5%)7150 (70.4%)0.278 Thiazides10410 (9.6%)7110 (14.1%)0.362Antiplatelet ASA10454 (51.9%)7137 (52.1%)0.98 Clopidogrel1047 (6.7%)717 (9.9%)0.454 Prasugrel1040 (0%)712 (2.8%)0.163Anticoagulation Warfarin1043 (2.9%)712 (2.8%)1.000 DOAC1041 (1.0%)712 (2.8%)0.567Other CV medications Statin10456 (53.8%)7143 (60.6%)0.379Devices PPM only1043 (2.9%)716 (8.5%)0.161 ICD10411 (10.6%)716 (8.5%)0.641Vitals Systolic blood pressure, mm Hg102120 (106, 130)71119 (110, 130)0.698 Diastolic blood pressure, mm Hg10270 (62, 78)7170 (65, 80)0.103 Heart rate, bpm10473 (64, 83)7173 (65, 80)0.686Labs Creatinine (mg/dL)1041.16 (0.94, 1.45)711.17 (1.00, 1.45)0.511 eGFR (mL/min/m^2^)10364 (50, 77)7162 (46, 76)0.521 troponin T (ng/L)990.05 (0.02, 0.09)700.05 (0.03, 0.12)0.319 NT-proBNP (pg/mL)1031830 (780, 3,837)711904 (1,081, 4,257)0.173Amyloidosis staging Mayo98700.987 156 (57.1%)40 (57.1%) 223 (23.5%)17 (24.3%) 319 (19.4%)13 (18.6%) Gilmore103710.599 170 (68.1%)49 (69.0%) 221 (20.4%)11 (15.5%) 312 (11.7%)11 (15.5%) Columbia103710.557 Stage I (1-3 points)54 (52.4%)35 (49.3%) Stage II (4-6 points)38 (36.9%)31 (43.7%) Stage III (7-9 points)11 (10.7%)5 (7.0%)Echo LVEF, %8247 (34, 56)5850 (33, 55)0.786 IVS, cm811.6 (1.4, 2.0)571.7 (1.5, 1.9)0.725 PWT, cm791.5 (1.3, 1.8)561.6 (1.4, 1.8)0.469 RWT780.71 (0.56, 0.90)560.74 (0.60, 0.86)0.649 LVEDDi, cm/m^2^802.3 (2.0, 2.6)562.2 (2.1, 2.4)0.324 LVESDi, cm/m^2^781.8 (1.6, 2.2)561.8 (1.5, 2.1)0.711 LVEDVi, mL/m^2^8046 (37, 56)5643 (39, 50)0.573 LVESVi, mL/m^2^7824 (17, 33)5622 (18, 31)0.896 LVSVi, mL/m^2^7819 (14, 28)5621 (14, 25)0.921 LV mass index, g/m^2^77162 (126, 193)55151 (131, 181)0.664 Cardiac index, L/(min∗m^2^)771.4 (1.1, 1.8)561.5 (1.1, 1.8)0.989 MCF, %7712 (9, 19)5514 (9, 17)0.93 LAVI (mL/m^2^)7839.5 (34.0, 48.3)6441.5 (36.6, 48.2)0.167Disease modifying agents on follow-up Tafamidis10456 (53.8%)7139 (54.9%)0.888 Diflunisal10416 (15.4%)7117 (23.9%)0.155Abbreviation as in Table 1.Table 3. Binary Logistic Regression for Pre-Existing AF on Initial Presentation95.0% CIUnivariable ModelORLowerUpperP ValueAge, per year1.0541.0281.080<0.001White race (reference: non-White)2.4091.5093.847<0.001ATTRv (reference: ATTRwt)0.2320.1440.375<0.001Hispanic (reference: non-Hispanic)0.3140.1170.8440.022Columbia score, per point1.3051.1691.457<0.001LAVI, per mL/m^2^1.0641.0391.089<0.001Multivariable ModelAge, per year1.0290.9921.0670.126White race (reference: non-White)0.7910.2972.1070.639ATTRv (reference: ATTRwt)0.1930.0680.5470.002Hispanic (reference: non-Hispanic)0.5770.1572.1190.407Columbia score, per point1.4821.2531.752<0.001LAVI, per mL/m^2^1.0481.0221.075<0.001From the total of 419 (total study sample size), 298 observations were used in the multivariate logistic regression model. 121 observations were removed due to missing values for explanatory variables.ATTRwt = wild-type amyloid transthyretin; other abbreviations as in Table 1.
Of the 175 subjects who had no prior AF at baseline, 104 (59%) did not developed de novo AF (no incident AF cohort) and 71 (41%) developed new onset AF (incident AF cohort) during the follow-up (Table 3). The presence of AF was determined from serial ECGs in 56 (78.9%) patients, cardiac device interrogation in 10 (14.1%) patients, and extended rhythm monitoring in 5 (7.0%) patients. Compared to the no incident AF group, the incident AF cohort had more individuals of male sex (93.0% vs 78.8%) and White race (78.9% vs 61.5%) but fewer with a genetic variant of ATTR (25.4% vs 49.0%), NYHA class I functional status (8.5% vs 21.2%), and history of hypertension (42.3% vs 58.7%). From the 175 subjects with no prevalent AF, 18 (10.3%) underwent heart transplant and 67 (38.3%) died. There were no major differences in age, ethnicity, body habitus, CHARGE-AF score, other comorbidities, implanted devices, vital signs, labs, or echocardiographic findings between the 2 groups.
Cox proportional modeling for the effect of clinically relevant covariates on incident AF is shown in Table 4. The median follow-up time was 2.0 years for the overall subcohort, 1.9 years for the incident AF cohort, and 2.5 years for the no incident AF cohort. On multivariable analysis, per point increase in Columbia score (HR: 1.18; 95% CI: 1.01-1.38; P = 0.035) was predictive of incident AF, whereas CHARGE-AF was not significant even on the univariable model. Moreover, ATTRv (HR: 0.44; 95% CI: 0.23-0.87; P = 0.017) and tafamidis (HR: 0.54; 95% CI: 0.30-0.95; P = 0.034) were protective.Table 4. Cox Proportional Hazard Modeling for Endpoint of Incident AF95.0% CIUnivariable Cox RegressionHRLowerUpperP ValueMale (reference: female)2.5451.0256.3200.044ATTRv (reference: ATTRwt)0.5320.3110.9100.021Hispanic (reference: non-Hispanic)0.3980.0971.6260.199CHARGE-AF score, per point1.2000.9501.5150.125Columbia score, per point1.1821.0431.3400.009LAVI, per mL/m^2^1.0381.0111.0650.005Tafamidis0.6640.4151.0620.087Multivariable Cox RegressionMale (reference: female)1.750.6005.1190.305ATTRv (reference: ATTRwt)0.440.2250.8650.017Columbia score, per point1.181.0121.3840.035LAVI, per mL/m^2^1.030.9991.0510.058Tafamidis0.540.3010.9540.034From the total of 175 with no prior AF on initial presentation, 132 observations were used in the multivariate Cox PH model. 43 observations were removed due to missing values for explanatory variables.Abbreviation as in Tables 1 and 2.
Discussion
This study explored the clinical factors associated with prevalent AF at initial presentation and predictors of de novo AF during the follow-up for patients diagnosed with ATTR-CA. The major findings are: 1) ATTRwt, greater Columbia score, and dilated LA are most closely associated with pre-existing AF; and 2) the Columbia score, but not the CHARGE-AF score, was predictive of new onset AF, whereas ATTRv and tafamidis were protective against it (Central Illustration).Central IllustrationPrevalence, Incidence, Clinical Predictors of Atrial Fibrillation/Flutter in 419 Patients With Transthyretin Amyloid CardiomyopathyCreated in BioRender, Brailovsky Y (2025), https://BioRender.com/btmxrvj. AF = atrial fibrillation/flutter; ATTR = transthyretin amyloid; LAVI = left atrial volume index; ATTRv = hereditary amyloid transthyretin; ATTR-CA = transthyretin cardiac amyloidosis.
Prior literature has reported an AF prevalence of about 50 to 88% in ATTR-CA(2-5), of which our study’s prevalence falls within the previously reported range (at initial presentation: 58% [244/419]; overall final rate when adding the 71 incident AF cases: 75% [315/419]). Most recently, Papathanasiou et al2 performed a retrospective cohort study of 133 cardiac amyloidosis patients seen at their tertiary care center over a 15-year period. Their overall AF prevalence was 71%, with 80% (43/54) of ATTRwt and 12.5% (1/8) of ATTRv having pre-existing AF. Although these were slightly different from our study population (67% [212/318] of ATTRwt and 32% [32/101] of ATTRv), we both show that proportionally more ATTRwt than ATTRv had AF at baseline.2 This difference of AF prevalence between ATTRwt and ATTRv may be more reflective of the difference in prevalence of AF in varying races rather than reflective of underlying pathophysiology of ATTR-CA. Patients with ATTRwt are predominantly White, whereas ATTRv are predominantly black in our cohort. It has been previously demonstrated that in general population AF prevalence is substantially higher in White compared to Black patients.21
Similar to our cohort, prior studies showed that subjects with prevalent AF, when compared to those with no AF, were older individuals who more often had NYHA functional class III to IV functional status, CKD, and greater LAVI. We also demonstrate increasing prevalence of AF with worsening ATTR-CA disease severity per NAC staging and Columbia staging, the latter of which incorporates NAC stage + NYHA functional class + diuretic dose (NAC stage I: 52% [127/246], NAC stage II: 65% [59/91], NAC stage III: 70% [54/77]; Columbia stage I: 44% [71/160]; Columbia stage II: 65% [127/196]; Columbia stage III: 72% [41/57]).
In contrast to the known high prevalence of AF, the real incidence during the follow-up remains unclear. Ascertainment of de novo AF is challenging. AF can be documented on routine ECG during follow-up or only assessed for symptomatic episodes. Additionally prolonged monitoring can be used to assess for paroxysmal AF. The mode and duration of monitoring would yield varying incidence of AF, with longer duration of monitoring with 30-day event monitor and implantable loop recorder likely associated with higher yield, as has been previously shown in patients with stroke.22^,^23 Using a combination of ECGs, device interrogations and long-term rhythm monitoring could introduce an ascertainment bias as not all subjects underwent long-term monitoring and only those with devices have them interrogated. Those subjects with more assessments for incident AF (e.g. electrocardiogram, long term monitoring and/or device interrogation) are more likely to have it detected. Such strategy is a strength of our study in that we evaluated for incident AF using a multimodal approach, which differs from other studies in which incident AF is only detected by ECGs.
Ascertainment of de novo AF was first addressed by Donnellan et al.5 in a retrospective cohort study of 382 ATTR-CA patients (71% ATTRwt, 29% ATTRv). They found that 60.2% patients developed incident AF and older age (HR: 1.02 per year; 95% CI: 1.005-1.03; P = 0.007), advanced NAC ATTR-CA stage (HR: 1.18; 95% CI: 1.005-1.39; P = 0.04), and higher LAVI (HR: 1.01 per ml/m^2^; 95% CI: 1-1.02; P = 0.045) to be associated with developing AF,5 similar to our findings. In our study, we ascertained the presence of AF via several methods, including cardiac device interrogation in 35% of patients, extended outpatient rhythm monitoring in 54% of patients, and serial ECGs in 11% of patients.
A more recent investigation was performed by a multicenter retrospective observational cohort study by Fumagalli et al.24 which consisted of 266 consecutive ATTRwt patients. In this population, history of AF was confirmed by the review of prior clinical documentation of arrhythmia episodes, and all patients had at least annual Holter monitoring. In their study, 29% subjects developed de novo AF,24 with a median time to AF onset of 27 months.24 On multivariable Fine-Gray Regression analysis, with mortality as a competing risk for incidence of de novo AF, they demonstrate several markers on baseline ECG to be predictive of incident AF (increased PR interval and QRS duration) as well as increased LA diameter.24 Patients with at least 2 risk factors (PR ≥ 200 ms, QRS ≥120 ms, or LA diameter ≥50 mm) had the highest risk of developing de novo AF compared to patients without risk factors (HR: 14.918; 95% CI: 3.242-31.646; P = 0.008). Although this represented the first study to directly associate ECG parameters to de novo AF in ATTRwt, staging was not able to be performed due to missing biomarkers.
The incidence of AF in our study was 41% (71/175 subjects without prior AF), which falls in the middle of the values reported by these 2 previous studies.5^,^24 We confirmed the predictive utility of ATTR-CA staging for incident AF via the Columbia score, of which per point increase led to a 18% greater risk for incident AF, but LAVI or LA diameter failed to reach significance. What is intriguing and not looked at by either of the prior investigations, is the lack of utility for the CHARGE-AF score for ATTR-CA patients despite its value in predicting de novo AF in the general population. This may be explained by the fact that all the ATTR-CA patients all had heart failure and are likely sicker than general population with AF thereby lowering its discriminatory ability. ATTRv was also shown to be strongly protective against incident AF, although unclear if this could partially be attributed to lower age. In addition, a cross-sectional analysis of the MESA (Multiethnic Study of Atherosclerosis) study has demonstrated that the prevalence of clinically detected AF is significantly lower in African American compared to in White patients,25 which may explain the protective effect of ATTRv in our cohort, most of whom are African Americans with Val142Ile mutation. However, in that same study, unbiased AF detection using ambulatory monitoring in the same individuals revealed minimal difference in the proportion with AF by race.25 In our study, a multimodal approach for AF detection was used to minimize such bias.
Moreover, given that disease-modifying therapy was known to be prescribed to most of our patients (54.3% [95/175]) unlike prior studies, we were able to perform an analysis of the effect of tafamidis on incident AF. We found that tafamidis exerted a strong protective effect with an estimated 46% reduction in the incident AF. This is consistent with findings from a prior retrospective study of ATTR-CA patients from our center, which showed that after adjustment for measured confounders including age, sex, left ventricular ejection fraction, obesity, hypertension, and LA diameter, tafamidis use reduced the risk of incident AF development by 57%, P = 0.03.26 Prior imaging studies have demonstrated tafamidis delays structural and functional changes in the heart, as reflected by lesser deterioration of biventricular ejection fraction and global longitudinal strain, LA reservoir strain, left ventricular mass index, and extracellular volume.27, 28, 29 These effects may in part mediate the observation that tafamidis use is associated with lower incidence of atrial fibrillation. Notably, in the ATTR-ACT (Tafamidis in Transthyretin Cardiomyopathy Clinical Trial) trial, although events were very low, tafamidis was associated with a lower risk of hospitalization for stroke/transient ischemic attack (2.7% vs 4.5%) and lower risk of hospitalization for arrhythmias (15.2% vs 21.5%).30
Study Limitations
There are several limitations to our investigation. First, this is a single-center retrospective observational cohort study, with inherent selection bias and residual confounding in our modeling that prevents definitive conclusions about which clinical factors are the most important in determining AF development. Second, AF was assessed as either present or absent, without accounting for duration of episodes, which may be important in some cases with regards to clinical significance. Third, despite our thorough approach to assess for AF, occult low-burden AF may have been missed since not all subjects had long-term monitoring or implanted devices and patients with paroxysmal and asymptomatic AF are most likely to be missed. Fourth, we did not collect baseline electrocardiographic parameters on all individuals and did not explore ECG-derived predictors of future AF, but this is of interest and should be explored in future studies. Fifth, LA strain was not routinely assessed. We did not assess the impact of sodium glucose co-transporter 2 inhibitors on patient outcomes, as a substantial proportion of patients were enrolled before approval and wide implementation of this class of medications. Tafamidis use was determined at baseline, and it was not included in the model as a time-varying covariate. Finally, the limited duration and modality of AF monitoring may have led to underestimation of incident AF cases, particularly if AF was paroxysmal or asymptomatic. Further research with multicenter subject pools would be helpful to validate our results.
Conclusions
More than half of ATTR-CA patients have pre-existing AF on initial presentation, which is most closely associated with ATTRwt, greater Columbia stage, and dilated LA. About half of the ATTR-CA patients without prior AF subsequently developed new onset AF during 3.5 year follow-up, which was predicted by the Columbia score but not CHARGE-AF score. ATTRv and tafamidis were protective against incident AF.
Funding support and author disclosures
Dr Maurer has received grant support from 10.13039/100000002NIH R01 HL139671 and R01AG081582-01; consulting income from BridgeBio, Ionis, Novo-Nordisk, Pfizer, Astra Zeneca, Alnylam, and Intellia; and institutional support in the form of clinical trial funding from Pfizer, Attralus, Ionis, BridgeBio, Intellia, and Alnylam. Dr Brailovsky has received consulting fees from BridgeBio, AstraZeneca, Pfizer, and Alnylam. Dr Yarmohammadi has received consulting fee from Biotronik. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ruberg F.L.Maurer M.S.Cardiac amyloidosis due to transthyretin protein: a review Jama 33120247787913844158210.1001/jama.2024.0442 PMC 11167454 · doi ↗ · pubmed ↗
- 2Papathanasiou M.Jakstaite A.M.Oubari S.Clinical features and predictors of atrial fibrillation in patients with light-chain or transthyretin cardiac amyloidosis ESC Heart Fail 92022174017483517888710.1002/ehf 2.13851 PMC 9065861 · doi ↗ · pubmed ↗
- 3Mints Y.Y.Doros G.Berk J.L.Connors L.H.Ruberg F.L.Features of atrial fibrillation in wild-type transthyretin cardiac amyloidosis: a systematic review and clinical experience ESC Heart Fail 520187727792991655910.1002/ehf 2.12308 PMC 6165925 · doi ↗ · pubmed ↗
- 4Bukhari S.Barakat A.F.Eisele Y.S.Prevalence of atrial fibrillation and thromboembolic risk in wild-type transthyretin amyloid cardiomyopathy Circulation 1432021133513373377926810.1161/CIRCULATIONAHA.120.052136 · doi ↗ · pubmed ↗
- 5Donnellan E.Wazni O.M.Hanna M.Atrial fibrillation in transthyretin cardiac amyloidosis: predictors, prevalence, and efficacy of Rhythm control strategies JACC Clin Electrophysiol 62020111811273297254610.1016/j.jacep.2020.04.019 · doi ↗ · pubmed ↗
- 6El-Am E.A.Dispenzieri A.Melduni R.M.Direct current cardioversion of atrial arrhythmias in adults with cardiac amyloidosis J Am Coll Cardiol 7320195895973073271310.1016/j.jacc.2018.10.079PMC 6378685 · doi ↗ · pubmed ↗
- 7Touboul O.Algalarrondo V.Oghina S.Electrical cardioversion of atrial arrhythmias with cardiac amyloidosis in the era of direct oral anticogulants ESC Heart Fail 92022355635643590387910.1002/ehf 2.14082 PMC 9715864 · doi ↗ · pubmed ↗
- 8Ullah W.Ruge M.Hajduczok A.G.Adverse outcomes of atrial fibrillation ablation in heart failure patients with and without cardiac amyloidosis: a nationwide readmissions database analysis (2015-2019)Eur Heart J Open 32023 oead 02610.1093/ehjopen/oead 026PMC 1009825437065605 · doi ↗ · pubmed ↗