Skull base invasive aspergillosis in a peritoneal dialysis patient: A rare and devastating complication
Nattapakorn Mai-on, Rubash Nath Yogi, Piyaporn Towangnang, Talerngsak Kanjanabuch

TL;DR
A rare and severe fungal infection in a peritoneal dialysis patient leads to life-threatening complications, highlighting the need for early detection and precise treatment.
Contribution
This is the first documented case of skull base invasive aspergillosis in a peritoneal dialysis patient.
Findings
Invasive Aspergillus flavus mastoiditis progressed to skull base osteomyelitis in a peritoneal dialysis patient.
Despite aggressive treatment, the infection spread to the carotid sheath and caused severe complications.
Molecular sequencing confirmed the species as A. flavus, excluding other cryptic species.
Abstract
Aspergillus mastoiditis with skull base osteomyelitis is an exceptionally rare but life-threatening infection in patients undergoing peritoneal dialysis (PD). We report a 60-year-old man with diabetic kidney failure on PD who developed invasive Aspergillus flavus mastoiditis progressing to skull base osteomyelitis. Despite early mastoidectomy, PD catheter removal, and voriconazole therapy achieving therapeutic levels, the infection advanced to involve the carotid sheath and parapharyngeal space, resulting in severe neurologic and systemic complications. Molecular sequencing confirmed A. flavus, excluding cryptic species such as A. tamarii. This case represents the first documented instance of skull base invasive aspergillosis in a PD patient and underscores the importance of early suspicion, species-level molecular confirmation, and multidisciplinary management in this formidable and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
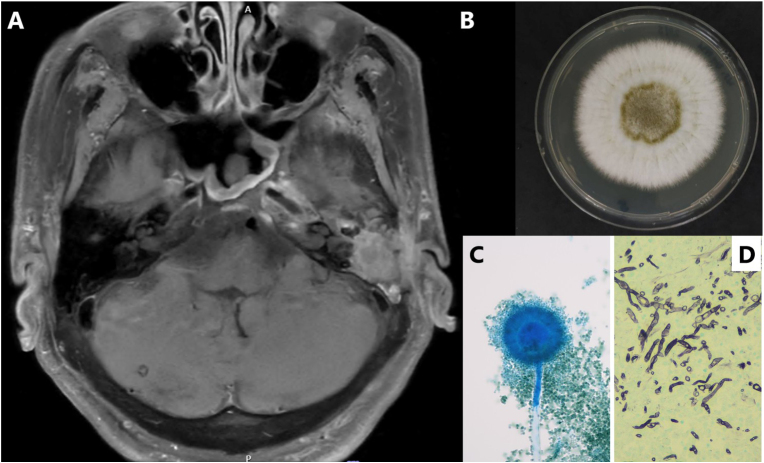 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Antifungal resistance and susceptibility · Sinusitis and nasal conditions
Introduction
1
Patients with kidney failure receiving peritoneal dialysis (PD) are particularly susceptible to infections, owing to uremia-associated immune dysfunction, frequent hospital administration, and a high burden of chronic comorbidities [1]. While bacterial peritonitis remains the most common infectious complication, fungal infections—especially extrapulmonary invasive aspergillosis—are exceedingly rare and carry high mortality. Among these, malignant otitis externa (MOE) with skull base osteomyelitis caused by Aspergillus species is an ultra-rare but devastating entity in the dialysis population. To date, only two cases have been reported in the literature—one from the UK involving concomitant P. mirabilis infection and another from Norway reported in Norwegian—both occurring in hemodialysis patients, with none previously documented in PD patients [2,3].
We describe a rare case of skull base invasive aspergillosis caused by Aspergillus flavus in a patient with diabetic kidney failure receiving PD. The infection progressed rapidly despite a combination of aggressive antifungal therapy and surgical intervention—underscoring the substantial diagnostic and therapeutic challenges encountered in this vulnerable population.
Case presentation
2
A 60-year-old Thai male monk with kidney failure secondary to diabetic kidney disease had been receiving nightly intermittent peritoneal dialysis (NIPD, 2 L × 5 exchanges) for two years. His comorbidities included poorly controlled type 2 diabetes mellitus, ischemic cardiomyopathy status post coronary artery bypass grafting with a left ventricular ejection fraction of 17 %, peripheral artery disease, prior ischemic stroke, post-parathyroidectomy secondary hyperparathyroidism, and severe protein–energy malnutrition.
He presented with a one-month history of left-sided otalgia and otorrhea without systemic symptoms. Two weeks later, he developed worsening otalgia, foul-smelling otorrhea, and new-onset left facial palsy. Temporal bone computed tomography (CT) revealed bony erosion involving the petrous portion of the temporal bone and adjacent skull base. Otoscopy demonstrated tympanic membrane perforation without granulation. Initial laboratory evaluation showed leukocyte count 9.64 × 10^3^/μL (Neu 72 %, Lym 11 %, Mono 6 %, Eos 9 %, Baso 1.3 %), hemoglobin 13.6 g/dL, hematocrit 44.1 %, and platelet 145 × 10^3^/μL. Chemistry results included Cr 6.1 mg/dL, Na 137 mmol/L, K 4.4 mmol/L, Cl 103 mmol/L, CO_2_ 25 mmol/L, AST 31 U/L, ALT 44 U/L, ALP 136 U/L, Ca 8.5 mg/dL, P 3.5 mg/dL, and Alb 2.3 g/dL.
A left mastoidectomy with facial nerve decompression was performed on July 27, 2024 (day 0). Surgical tissue was submitted for diagnostic evaluation. Portions were processed for histopathology, while parallel samples underwent Gram staining, acid-fast bacilli staining, modified acid-fast bacilli staining, and potassium hydroxide preparation, all of which were negative. Tissue specimens were cultured on blood agar, chocolate agar, and MacConkey agar for bacterial pathogens; on Sabouraud dextrose agar (SDA) and potato dextrose agar for fungal organisms; and on Loewenstein–Jensen medium and mycobacterial growth indicator tube culture system for mycobacteria. Polymerase chain reaction testing for Mycobacterium tuberculosis was also performed and yielded negative results.
Empirical intravenous piperacillin–tazobactam was started, followed by oral ciprofloxacin after discharge. Bacterial cultures remained negative; however, fungal culture grew A. flavus. After 7 days of incubation on SDA, colonies exhibited a velvety, yellow-green surface with pale reverse pigmentation (Fig. 1B), and lactophenol cotton blue mounts demonstrated rough conidiophores, biseriate phialides, and globose conidia (Fig. 1C). Upon receipt of the pathology report confirming invasive fungal disease (Fig. 1D), the patient was readmitted for definitive management.Fig. 1**(A)** MRI of the skull base demonstrating progressive osteomyelitis of the left petrous temporal bone with extension into the nasopharynx, carotid sheath, parapharyngeal space, and prevertebral muscle. **(B)**Aspergillus flavus colony on Sabouraud dextrose agar after 7 days of incubation, exhibiting a velvety yellow-green surface with pale reverse pigmentation. (C) Lactophenol cotton blue mount (400 × ) showing rough conidiophores, biseriate phialides, and globose conidia characteristic of A. flavus. (D) Histopathology of mastoid tissue demonstrating tissue-invasive septate hyphae on Gomori methenamine silver (GMS) stain (200 x).Fig. 1
Molecular sequencing performed on the cultured isolate confirmed A. flavus using four primer sets—SSU (18SF–18SR), ITS (ITS1–ITS4), and LSU (NL1–NL4; LR0R–LR7) [[4], [5], [6], [7]]—each demonstrating 100 % query coverage and ≥99.7 % sequence identity (Table 1). DNA was extracted using the magLEAD® 12gC system (Precision System Science, Japan) according to the manufacturer's protocol with minor modifications. The sequences were deposited in GenBank (OL655454.1, KJ999737.1, ON231619.1, HQ395773.1). Antifungal susceptibility testing, performed according to the CLSI M38-A3 broth microdilution method [8], showed MIC values of 1 μg/mL for amphotericin B, 0.5 μg/mL for voriconazole, >16 μg/mL for itraconazole, and 0.5 μg/mL for posaconazole and isavuconazole, interpreted using EUCAST ECOFFs for A. flavus [9].Table 1. Molecular identification of Aspergillus flavus from mastoid tissue culture.Table 1. OrganismPrimer SetScoreQuery CoverIdentityAccession No.A. flavusSSU (18SF–18SR)778/778100 %100 %OL655454.1A. flavusITS (ITS1–ITS4)909/909100 %100 %KJ999737.1A. flavusLSU (NL1–NL4)946/946100 %100 %ON231619.1A. flavusLSU (LR0R–LR7)1982/1982100 %99.72 %HQ395773.1
Voriconazole therapy was initiated with a loading dose of 6 mg/kg twice daily on day 7, followed by 4 mg/kg twice daily administered orally (body weight 38 kg; total daily dose 200–400 mg), with dosing adjustments guided by therapeutic drug monitoring. The trough level on day 5 was 3.2 μg/mL. Despite adequate drug exposure, serial CT and magnetic resonance imaging (MRI) showed progressive skull base osteomyelitis with extension into the nasopharynx, carotid sheath, parapharyngeal space, and prevertebral muscle (Fig. 1A). Neurosurgical intervention was deemed unfeasible.
The patient subsequently developed focal seizures due to local invasion, followed by septic and cardiogenic shock requiring intensive care unit admission, vasopressor support, and continuous kidney replacement therapy. His course was further complicated by Clostridioides difficile colitis and transaminitis, necessitating temporary interruption of antifungal therapy.
Given relentless disease progression, lack of surgical options, and the patient's deteriorating condition, a multidisciplinary team—nephrology, infectious diseases, otolaryngology, and neurosurgery—reached a consensus to transition care toward comfort measures and end-of-life support.
Discussion
3
This case highlights a rare and devastating manifestation of extrapulmonary invasive aspergillosis: mastoiditis with skull base osteomyelitis caused by A. flavus in a patient receiving PD. While Pseudomonas aeruginosa remains the leading pathogen in MOE, this infection extended beyond the external auditory canal to involve the mastoid and skull base—features more consistent with invasive fungal mastoiditis rather than MOE alone [10,11].
Patients on PD, particularly those with diabetes mellitus, malnutrition, and repeated broad-spectrum antibiotic exposure, are predisposed to opportunistic fungal infections due to uremia-associated immune dysfunction [1,12]. Although fungal peritonitis is the most recognized invasive fungal complication in PD, non-peritoneal invasive mold infections remain rare but clinically significant. The MycoPDICS registry further demonstrated that filamentous mold infections in PD patients, while uncommon, are associated with high mortality and a high likelihood of transition to hemodialysis [13].
Accurate species identification is vital. Aspergillus tamarii, a cryptic species, has previously been misidentified as A. flavus by morphology alone in PD-related peritonitis [14]. In our case, molecular sequencing of ribosomal DNA using four validated primer sets confirmed A. flavus with high confidence, preventing potential misclassification and ensuring appropriate antifungal selection.
Clinically, Aspergillus mastoiditis often mimics chronic bacterial otitis, presenting with persistent otalgia, otorrhea, and, in advanced stages, cranial nerve involvement such as facial palsy. Imaging that demonstrates bony erosion of the petrous temporal bone or skull base should prompt suspicion for fungal osteomyelitis. In this case, diagnosis was established through histopathology demonstrating septate hyphae, compatible culture growth, and definitive species-level molecular identification.
Management of invasive Aspergillus mastoiditis requires timely surgical debridement and systemic antifungal therapy supported by susceptibility testing and therapeutic drug monitoring. Voriconazole is considered first-line therapy due to its potent activity, superior bone and central nervous system (CNS) penetration, and demonstrated clinical advantage over amphotericin B [[15], [16], [17]]. Although voriconazole therapy in this patient achieved therapeutic plasma levels, the disease progressed aggressively, reflecting the challenges of treating advanced osteoinvasive disease where pharmacologic therapy alone may be insufficient.
Once fungal osteomyelitis extends to the skull base, carotid sheath, and parapharyngeal or prevertebral compartments, surgical intervention becomes technically unfeasible. In such circumstances, multidisciplinary collaboration—encompassing otolaryngology, infectious diseases, nephrology, neurosurgery, and palliative care—is essential for individualized decision-making and, when appropriate, transition to comfort-focused care.
This case underscores several key principles: (1) Fungal mastoiditis should be considered in PD patients with refractory otitis, particularly when cranial neuropathies or bony erosion are present; (2) Species-level identification using molecular diagnostics is crucial to avoid misclassification and guide targeted therapy; (3) Voriconazole remains the preferred antifungal agent, but optimal outcomes depend equally on early diagnosis and feasible surgical source control; and (4) Multidisciplinary management is indispensable in advanced disease.
Ultimately, invasive Aspergillus mastoiditis in PD patients, although rare, can be rapidly progressive and life-threatening. A high index of suspicion, early diagnostic evaluation, and coordinated care are essential to improve outcomes in this vulnerable population.
CRediT authorship contribution statement
Nattapakorn Mai-on: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. Rubash Nath Yogi: Writing – review & editing, Data curation. Piyaporn Towangnang: Writing – review & editing, Data curation. Talerngsak Kanjanabuch: Writing – review & editing, Validation, Supervision, Conceptualization.
Conflict of interest
This research was generously supported by the Health Systems Research Institute (HSRI), Thailand [Grant No. 68-109], and the Thailand Science Research and Innovation Fund, Chulalongkorn University, Thailand [Grant No. HEA_FF_68_018_3000_002]. TK has received consultancy fees from VISTERRA and AstraZeneca as a country investigator, a research funding from the National Research Council of Thailand. He has also received speaking honoraria from AstraZeneca, Alexion Pharmaceuticals Inc., Fresenius Medical Care, and Baxter Healthcare. The remaining author declared no commercial or financial relationships that could be construed as potential conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kato S.Chmielewski M.Honda H.Pecoits-Filho R.Matsuo S.Yuzawa Y.Aspects of immune dysfunction in end-stage renal disease Clin. J. Am. Soc. Nephrol.3520081526153310.2215/CJN.0095020818701615 PMC 4571158 · doi ↗ · pubmed ↗
- 2Stangeland K.W.Baardsen R.Weber C.Gjøse B.F.Biserød L.E.Koch H.W.A man in his fifties with pain in the head, neck and ear canal Tidsskr. Nor. Laegeforen 14213202210.4045/tidsskr.22.0144 Norwegian 36164783 · doi ↗ · pubmed ↗
- 3Thompson A.C.Zammit-Maempel I.Stafford F.Narayanan M.Kanagasundaram N.S.Necrotising otitis externa: an unusual cause of cranial nerve palsy in a diabetic haemodialysis patient J R Coll. Phys. Edinb.4012010262810.4997/JRCPE.2010.10621125035 · doi ↗ · pubmed ↗
- 4Einsele H.Hebart H.Roller G.Löffler J.Rothenhofer I.Müller C.A.Detection and identification of fungal pathogens in blood by using molecular probes J. Clin. Microbiol.35619971353136010.1128/jcm.35.6.1353-1360.19979163443 PMC 229748 · doi ↗ · pubmed ↗
- 5White T.J.Bruns T.Lee S.J.Taylor J.Amplification and direct sequencing of fungal ribosomal RNA genes for phylogenetics PCR Prot.: Guide Meth. Appl.1811990315322
- 6O’Donnell K.Ribosomal DNA internal transcribed spacers are highly divergent in the phytopathogenic ascomycete Fusarium sambucinum (Gibberella pulicaris)Curr. Genet.22199221322010.1007/BF 003517281525873 · doi ↗ · pubmed ↗
- 7Rehner S.A.Samuels G.J.Taxonomy and phylogeny of Gliocladium analysed from nuclear large subunit ribosomal DNA sequences Mycol. Res.986199462563410.1016/S 0953-7562(09)80409-7 · doi ↗
- 8The European Committee on Antimicrobial Susceptibility Testing – EUCAST Overview of antifungal ECOF Fs and clinical breakpoints for yeasts and moulds [Internet]Available from:https://www.eucast.org/astoffungi/clinicalbreakpointsforantifungals 2025