β-Human Chorionic Gonadotropin–Secreting Giant Cell Tumor of Bone in the Mandible: Case Report and Comprehensive Literature Review
Andres Flores-Hidalgo, Sholeh Bazrafshan, Hether Khosa

TL;DR
A rare case of a hormone-secreting bone tumor in the jaw of a 16-year-old girl is reported, highlighting unusual diagnostic challenges.
Contribution
First reported case of β-hCG–secreting giant cell tumor of bone in the gnathic bones.
Findings
The tumor was confirmed to secrete β-hCG, as evidenced by elevated levels and their decline with treatment.
Genomic sequencing identified an H3-3A p.G35W mutation and a pathogenic FANCA p.R951Q variant.
Denosumab therapy led to clinical improvement and reduced β-hCG levels.
Abstract
Giant cell tumor of bone (GCTB) is a rare but locally aggressive neoplasm which most commonly arises in the epiphyses of long bones of young adults. Occurrence in the mandible is uncommon, and hormone secreting variants are extremely rare. We present the case of a 16-year-old female, who presented with progressive swelling and pain in the left mandible after extraction of adjacent teeth. On examination, she had a large ulcerated intraoral mass with marked tooth mobility; imaging revealed a 4.7-cm expansive lytic lesion with cortical erosions and displacement of the inferior alveolar canal. Histopathologic evaluation revealed sheets of mononuclear stromal cells interspersed with numerous osteoclast-like giant cells. Immunohistochemical stains showed strong positivity for H3G34W and p63. Genomic sequencing confirmed the presence of an H3-3A p.G35W hotspot mutation and also identified a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1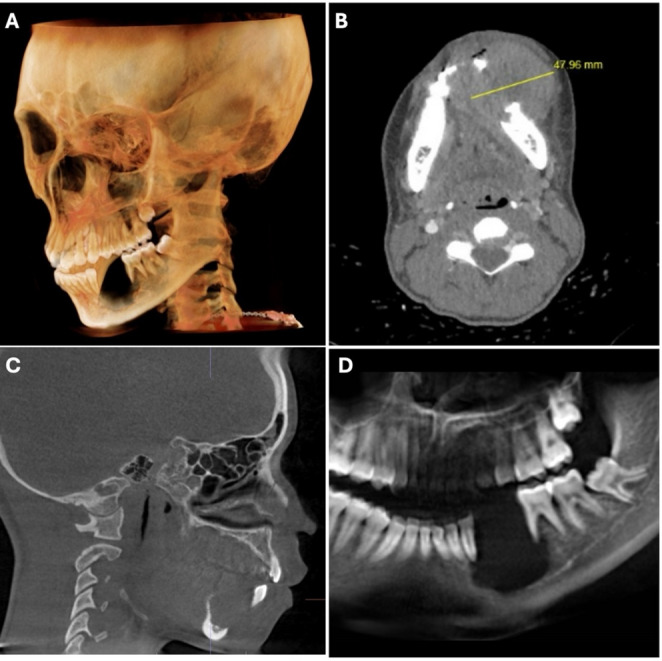 Figure 2
Figure 2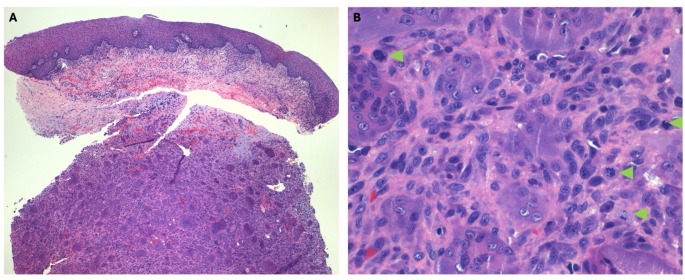 Figure 3
Figure 3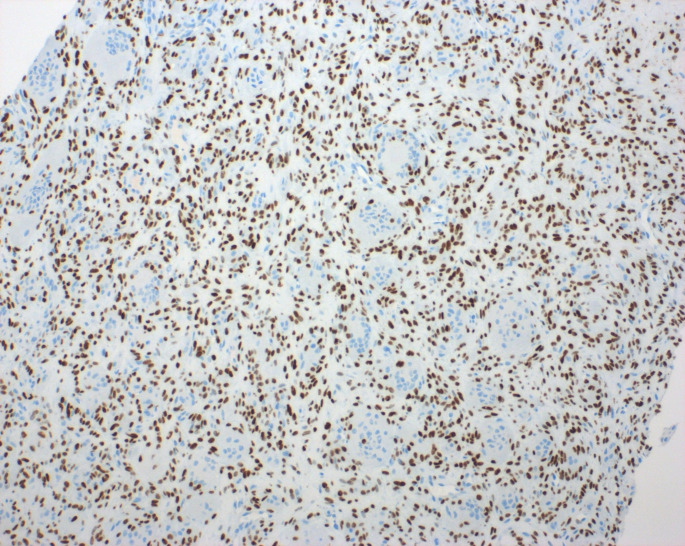 Figure 4
Figure 4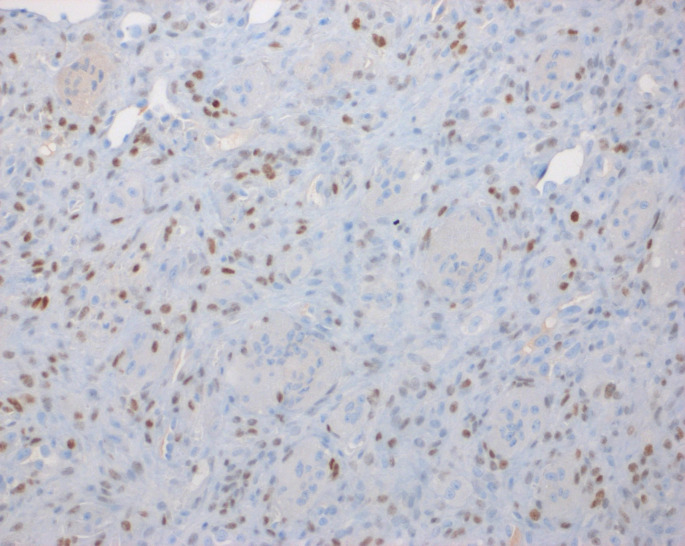 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Gestational Trophoblastic Disease Studies · Teratomas and Epidermoid Cysts
Introduction
Giant cell tumor of bone (GCTB) is a typically benign, but locally aggressive tumor characterized by the proliferation of mononuclear stromal cells with multiples osteoclast-like multinucleated giant cells. GCTB affects skeletally mature individuals between the ages of 20 and 40, and has a slight female predominance [1]. Although, GCTB generally arises in the epiphyseal regions of long bones (most commonly distal femur, proximal tibia, or distal radius), it may occur in virtually any region of the skeleton [2]. In recent years, advances in molecular pathology have demonstrated also that most conventional GCTB have mutations in the H3F3A gene, most often the G34W substitution that not only aids in tumor formation, but is also an essential diagnostic marker of GCTB [3, 4].
Although benign histologically, giant cell tumor of bone (GCTB) is notorious for its local recurrence, with some studies reporting rates of recurrence as high as 50% following curettage, and infrequently, metastasis to the lungs occurs. This report describes the case of a 16-year-old healthy female patient with a GCTB in the left mandible and details the clinical presentation, diagnosis, and significant histopathological and molecular findings [5].
Case Report
Clinical and Radiographic Presentation
A 16-year-old female was referred by an outside general dentist for evaluation and management of an expansile lesion to the left mandible. The patient had some swelling and discomfort a few weeks prior to her consultation. She obtained a second opinion from another dental provider who suspected it was a serious infectious process, and recommended tooth extractions and antibiotics. After extraction the patient felt her swelling and pain progressively increased. She was referred to the UC Health Medical Center, Division of Oral & Maxillofacial Surgery, for management.
The patient had no significant medical history and not known drug allergies. Clinical examination revealed unilateral enlargement of the lower third of the face. The intraoral examination revealed a large, ulcerated mass on the right mandible, premolar area (Fig. 1). Teeth #20 and 21 are absent and adjacent #22 and #30 show class IV mobility. A scanned Cone Beam computerized tomography (CBCT) taken of the area of interest revealed a large radiolucency, of ~ 4.7 cm in diameter, in the left mandible around teeth #20 and 21, to include inferior displacement of the inferior alveolar nerve. Erosion of the buccal and lingual cortex is evident (Fig. 2).
Fig. 1. Intraoral presentation of the lesion. Large, ulcerated mass on the left mandible
Fig. 2. Radiographic presentation. A 3D rendition of Cone Beam Computerized tomography (CBCT). B Transverse view with measurement of the diameter of the lesion. C Sagittal view. D Portion of panoramic radiograph
Histopathological Findings
Based on the clinical and radiological presentation, an incisional biopsy was performed on the same visit, under local anesthetic. A 2 cm x 2 cm piece of tissue was excised and sent for permanent histopathology. The microscopic findings showed a very cellular lesion with large, osteoclast-like, multinucleated giant cells intermixed with sheets of round to spindle mononuclear cells with pale eosinophilic cytoplasm, nuclei with dispersed chromatin and small nucleoli (Fig. 3a). Mitotic figures were also observed throughout the specimen (Fig. 3b), predominantly fewer than five per ten high-power fields. Hemorrhage, hemosiderin and foamy macrophages were seen too.
Fig. 3. Microcopy of incisional biopsy of the lesion. A Osteoclast-like multinucleated giant cells embedded in sheets of a mononuclear cell population underlying the surface oral mucosa [Hematoxylin and Eosin – 100X magnification]. B Higher power of magnification shows the multinucleated giant cells intermixed with a sheet of spindle cell mononuclear cells and scattered mitotic figures (green arrowheads) [Hematoxylin and Eosin – 400X magnification]
An initial diagnosis of giant cell granuloma (CGCG) was considered, but because of the aggressive behavior of the tumor and microscopic features, a H3G34W immunohistochemistry (IHC) was performed which showed strong nuclear reactivity in the neoplastic mononuclear cells of the tumor sparing multinucleated giant cells (Fig. 4). The p63 stain was also positive in the neoplastic population, though with a similar pattern to the stain to H3G34W (Fig. 5). From a clinical, microscopic, immunohistochemical, and molecular perspective a diagnosis of giant cell tumor of bone was made.
Fig. 4H3G34W immunohistochemical stain was performed showed strong nuclear reactivity in the neoplastic mononuclear cells sparing multinucleated giant cells [200X magnification]
Fig. 5p63 immunohistochemical stain shows a similar staining pattern as H3G34W [200X magnification]
Molecular Analysis
Cincinnati Children’s Cancer Sequencing (CinCSeq) Comprehensive Panel was performed and reported a homozygous hotspot H3-3 A p.G35W mutation consistent with histopathologic findings of specimen and rendered diagnosis. An additional pathogenic FANCA p.R951Q variant was found at variant allele frequency ~ 50%, which raised the possibility of germline. Tumor mutational burden was 3 mut/Mb. A complete listing of the identified DNA variants is found in Table 1.
Management
Pre-treatment assessment indicated a positive urine pregnancy test and β-human chorionic gonadotropin (β-hCG) serum level of 5.1 mIU/mL, but pregnancy had been definitively excluded. By the time of manuscript submission, the patient remained on active treatment. She was at Cycle 1, Day 21 of denosumab therapy (with plan of four weeks of weekly therapy transitioning to monthly maintenance dosing). At the last follow-up appointment, the tumor showed measurable decrease in size and the patient showed improvement in oral intake. Additionally, the β-hCG level had decreased to 2.6 mIU/mL, thus supporting its association with the neoplasm.
Discussion
Giant cell tumor of bone is an overall benign but locally aggressive neoplasm, which is defined as the proliferation of mononuclear stromal cells with multinucleated osteoclast-like giant cells scattered within the neoplasm. They are considered histologically benign, but GCTB has a marked tendency toward local recurrence, and in rare cases may metastasize, mostly to the lungs [1, 5].
GCTB accounts for approximately 4–5% of all primary bone tumors and 20% of all benign bone tumors [6, 7]. The principal demographic affected by GCTB is young adults between 20 and 40 years of age, with a slight female predominance, occurring primarily in the epiphyseal region of long bones - most commonly around the knee; GCTB can also occur in the distal radius and sacrum [8].
There is a clear link in the pathogenesis of GCTB to the H3-3 A gene changes, which encodes histone H3.3. The vast majority (approximately 92%) of all GCTBs have a mutation in codon 34, usually the p.Gly34Trp (G34W) [3, 4]. This mutation only happens in the neoplastic mononuclear stroma cells that are believed to be the neoplastic component of GCTB. The G34W mutation is believed to affect histone methylation patterns, thus modifying transcription and causing RANKL overexpression to promote osteoclastogenesis. The multinucleated giant cells are believed to be reactive from the monocyte–macrophage lineage cells, which arose from this signaling [9]. The H3-3 A gene that encodes the histone protein H3.3 acts as an oncogenic driver for developmental and transcriptional mechanisms. Canonical hotspot mutations arise at lysine 28 and glycine 34, with the G34 codon, specifically, the G34W substitution having the strongest correlation for giant cell tumor of bone [3].
There are also rare mutations such as the H3F3B alterations that have been reported, however, they are generally not related and may be related to specific anatomic locations [10]. The H3-3 A mutation has clinical significance since it is absent in histologic mimics such as aneurysmal bone cyst and chondroblastoma. Additionally, Gomes et al. 2014, found that H3-3 A p.Gly34 TRP, was not present in aggressive CGCG of the jaw and giant cell lesions of patients with cherubism [11].
Through next generation sequencing we also identified a pathogenic FANCA p.R951 variant. FANCA is a tumor suppressor gene that encodes the protein Fanconi anemia complementation group A, which is a member of the Fanconi anemia core complex that assembles at damaged chromatin and activates the DNA response by coordinating BRCA 1/2 proteins. Mutations of FANCA are the most prevalent, making up 65% of the heritable Fanconi’s anemia cases that are a cancer predisposition syndrome with elevated risk for a variety of malignant neoplasms [12].
GCTB consists histologically of three main cell types. The main cells are mononuclear stromal cells, the neoplastic cell population; these appear as round to oval cells with vesicular nuclei, moderate eosinophilic cytoplasm, and the occasional nucleolus. Multinucleated osteoclast-like giant cells, which can contain 20 to 50 + nuclei, are spaced randomly throughout the lesion and often clustered around hemorrhage. Finally, there are mononuclear histiocytic cells which are part of the reactive component and tend to be fewer than the stromal cells [13]. Mitotic activity is noted but atypical mitotic figures are infrequent in conventional GCTB. Areas of hemorrhage, hemosiderin deposition, and necrosis are common. Secondary aneurysmal bone cyst–like changes may be present in ~ 14% of cases [14]. Imunohistochemically the mononuclear stromal cells demonstrate strong nuclear positivity for H3.3 G34W mutation-specific antibody, whereas the giant cells are positive for CD68 [13, 15, 16].
Typical radiographic features include an eccentric lytic lesion affecting the epiphysis and extending to the subchondral bone with non-sclerotic margins, the lack of matrix mineralization, and an appearance similar to the radiographic presentation in our case [17]^,^ [18].
Although histologically benign, GCTB has a 20–50% local recurrence rate depending on surgical management [19]. Malignant giant cell tumor of bone is an uncommon aggressive variant that accounts for less than 5% of all GCTB. It can arise de novo (primary malignant GCTB) or more commonly as a secondary transformation from a previously established benign GCTB, generally after multiple recurrences or following prior radiotherapy [20]. Malignant transformation is very rare, typically occurs after radiation therapy, or with recurrent disease. The prognostic factors for recurrence include the site (distal radius and sacrum), inadequate surgical margins, and secondary aneurysmal bone cyst changes [21, 22].
β-human chorionic gonadotropin (β-hCG)–expressing giant cell tumor of bone (GCTB) is incredibly rare. Although the production of β-hCG has been defined for some bone sarcomas, for example, osteosarcoma [23]. However, β-hCG expression in GCTB, in gnathic bones, is exceedingly rare. To date, the only case found in the medical literature described the finding of a GCTB that had changes of an aneurysmal bone cyst-like changes in the head and neck region. In this case, the patient’s serum β-hCG levels returned to normal following resection, confirming that the tumor was the source of hormone production [24]. In our patient, the levels of β-hCG dropped with treatment with denosumab. To the best of our knowledge, this may be the first reported case of β-hCG secreting GCTB in the mandible. Yet, Lawless et al. (2014) published an institutional case series of 40 patients with β-hCG–secreting GCTB [23]. In one case, the tumor arose in the posterior mandible and showed mild positivity for β-hCG on IHC. However, the authors did not clarify whether this patient had elevated serum β-hCG levels and noted that, in several cases, there was a discrepancy between immunohistochemical expression and serum findings. A full summary of reported GCTB in the head and neck region is presented in Table 2.
There is a gap in the literature regarding the prognostic and therapeutic implications of β-hCG expression in GCTB. No systematic studies have been published that investigate the impact of β-hCG positivity on recurrence risk, metastatic risk, or therapy response in these tumors [24–26]. Therefore, more research is needed to investigate whether β-hCG expression has clinical relevance other than causing challenges in the diagnostic interpretation. The current standard of care for GCTB remains surgical curettage, either with or without local adjuvant therapy, and denosumab for unresectable or recurrent disease [25, 27]. Though β-hCG expression does not currently influence best treatment practices, recognition of this rare finding is important to ensure the correct diagnosis and highest quality clinical care [23, 24].
Complete surgical excision is the gold standard for GCTB in the mandible, ideally with negative margins to minimize chances of recurrence [27, 28]. Extended intralesional curettage with local adjuvants is preferred, where possible, with recurrence rates up to 27%, depending on technique and adjuvant used. En bloc resection may be required for large or recurrent lesions, but must be weighed against mandibular reconstruction morbidity, particularly in younger patients such as ours [27, 28].
The use of denosumab, a monoclonal antibody to RANKL has changed the management of unresectable or recurrent GCTB^28^. Denosumab reduces the number of giant cells and induces bone formation. While long-term follow up and recurrence rates after discontinuation remain under assessment [9, 16].
Conclusion
In conclusion, GCTB is rare in the gnathic bones and represents a small percentage of all documented cases. Our case of mandibular GCTB in an otherwise healthy 16-year-old female demonstrates the importance of ruling out GCTB when examining head and neck giant cells lesions, such as CGCG. While β-hCG expression does not presently impact established treatment protocols, its recognition is critical for accurate diagnosis, particularly those occurring in atypical locations and in atypical age groups or in patients, and the provision of the highest standard of clinical care.
The diagnosis requires the careful integration of clinical, radiographic, and histopathologic features, as well as molecular confirmation such as H3-3 A mutation testing. Although surgical resection remains the standard of care, the unique anatomy and functional role of the mandible require a thoughtful and individualized approach to minimize disease while maximizing esthetics and maintaining oral function.
Though the prognosis is usually reasonable following appropriate management, the risk of local recurrence, especially in younger patients, warrants long-term follow-up.
Table 1. Detailed results of DNA variant encountered by next generation sequencingBiomarkerVariantVAF/CNR (%)LocationClassification DNA variants
H3-3 A p.G35Wc.103G > T27exon-2Tier 1/2 FANCA p.R951Qc.2852G > A50exon-29Tier 1/2 ERCC2 p.L152Pc.455T > C49exon-6VUS PRKDC p.I3193Mc.9579 A > G47exon-69VUS TEK p.T693Ic.2078 C > T45exon-13VUS MSH6 p.?c.4001 + 10_4001 + 11insAACTA45intron-9VUS KMT2C p.S207Cc.620 C > G45exon-5VUS BCORL1 p.A130Tc.388G > A45exon-4VUS CSF1R p.T467Mc.1400 C > T44exon-9VUS BCOR p.P1156Tc.3466 C > A32exon-7VUS FGFR1 p.G348_S353delc.1043_1060del26exon-8VUS SLX4 p.P1317_P1321delc.3949_3963del5exon-12VUS Fusions/SV None Copy number variations None
Table 2. This table summarizes the clinical, pathological, and diagnostic features of reported cases of β-hCG secreting giant cell tumor of bone in the head and neck region, highlighting the extreme rarity of β-hCG production in this tumor type and anatomical location, as documented in the medical literatureCase/SeriesLocationβ-hCG SecretionKey findingsReferencesFitzhugh et al. [24]Sphenoid bone (skull base)Yesβ-hCG detected in serum and tumor; resolved after resection[24]Zhang et al. (2013)Skull (18 cases)NoNo β-hCG secretion reported[29]Freeman et al. (2016)Skull base (meta-analysis)NoNo β-hCG secretion reported[30]Gao et al. [28]Maxillofacial regionNoNo β-hCG secretion reported[28]Battoo et al. (2012)Nasal cavity/skull baseNoOncogenic osteomalacia, no β-hCG secretion[31]Akyigit et al. (2014)Temporal bone/TMJNoNo β-hCG secretion reported[32]Inoue et al. (2016)ClivusNoNo β-hCG secretion reported[33]
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang Z, Xu J, Yao Y, Chu S, Cheng H, Chen D, et al (2013) Giant celltumors of the skull: a series of 18 cases and review of the literature. J Neurooncol 115:437–4410.1007/s 11060-013-1242-z 24043601 · doi ↗ · pubmed ↗
- 2Freeman JL, Oushy S, Schowinsky J, Sillau S, Youssef AS (2016) Invasive Giant Cell Tumor of the Lateral Skull Base: A Systematic Review, Meta-Analysis, and Case Illustration. World Neurosurg 96:47–5710.1016/j.wneu.2016.05.08627269210 · doi ↗ · pubmed ↗
- 3Battoo AJ, Salih S, Unnikrishnan AG, Jojo A, Bahadur S, Iyer S, et al (2012) Oncogenic osteomalacia from nasal cavity giant cell tumor. Head Neck 34:454–710.1002/hed.2156222311466 · doi ↗ · pubmed ↗
- 4Akyigit A, Karlidag T, Sakallioglu ÖÖ, Polat C, Keles E (2014) Giant cell tumor of bone involving thetemporomandibular joint and temporal bone. J Craniofac Surg 25:1397–910.1097/SCS.000000000000087625006918 · doi ↗ · pubmed ↗
- 5Inoue A, Ohnishi T, Kohno S, Nishikawa M, Nishida N, Ohue S (2016) Role of denosumab in endoscopic endonasaltreatment for juvenile clival giant cell tumor: A case report and review of the literature. World Neurosurg 91:674.e 1–610.1016/j.wneu.2016.04.05427113403 · doi ↗ · pubmed ↗