Accuracy of reirradiation dose constraints for the mandible and carotids
Sara Bornedal, Jeehong Lee, Tim Melhus, Anna Embring, Eva Onjukka

TL;DR
The study evaluates the accuracy of reirradiation dose constraints for head and neck cancer, finding generally reliable results despite some anatomical and imaging challenges.
Contribution
A structure-based evaluation of deformable image registrations to assess uncertainty in reirradiation dose constraints.
Findings
Most cases showed subvoxel geometrical uncertainty in dose constraints.
Outliers were observed in carotid regions due to anatomical changes and poor image quality.
Previously suggested dose constraints remain reliable despite registration uncertainties.
Abstract
•Evaluation of intensity-based deformable image registrations for reirradiation.•Generally subvoxel geometrical uncertainty for organs at risk in the head and neck.•Outliers among carotids due to anatomical changes and poor image quality.•Provides confidence in reirradiation dose constraints for head and neck cancer. Evaluation of intensity-based deformable image registrations for reirradiation. Generally subvoxel geometrical uncertainty for organs at risk in the head and neck. Outliers among carotids due to anatomical changes and poor image quality. Provides confidence in reirradiation dose constraints for head and neck cancer. When reirradiation dose constraints are derived using accumulated dose, the underlying image registrations contribute to the uncertainty. We performed a structure-based evaluation of deformable image registrations, to estimate the uncertainty in previously…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
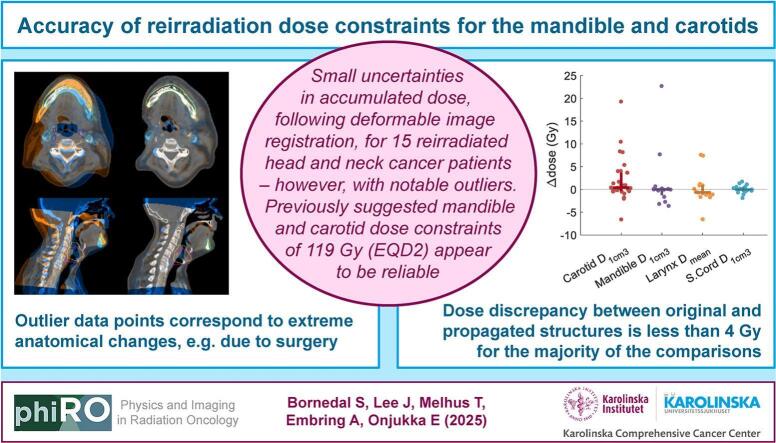 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Radiography and Imaging · Radiation Dose and Imaging · Advanced Radiotherapy Techniques
Introduction
1
The challenges in planning safe and effective reirradiation for recurrent- or second primary cancer have received increasing attention [1], [2], [3]. The uncertainties involved propagate to the interpretation of outcome data for organ-at-risk (OAR) dose response [4], resulting in scarce and uncertain dose constraints for the reirradiation setting [5]. According to a patterns-of-care survey, the pelvis and the head and neck are the most common sites of reirradiation, after the brain [5]. In previous work, we studied the accumulated dose to OAR, in relation to severe late side effects, for reirradiated head and neck cancer (HNC) patients receiving at least 100 Gy accumulated dose, in equivalent dose in 2-Gy fractions (EQD2) [6]. The results provided much needed support for previously proposed dose constraints regarding carotid blowout [7] and osteoradionecrosis (ORN) [8], which were based on very limited evidence. The dose summation was performed using dose distributions in EQD2 after deformable image registration (DIR) [9], according to consensus recommendations [10]. Even so, geometrical uncertainties are unavoidable in such a cohort, considering the anatomical changes associated with the temporal separation between the treatments (up to nearly 15 years), differences in treatment setup and the mix of external-beam radiotherapy and brachytherapy.
DIR is an effective means of mapping dose in the context of dose accumulation, and it seems to obtain a higher degree of consistency compared to alternative methods [4]. It has been implemented in clinical practice by some centres, but the majority still rely on rigid registration for dose mapping [5]. Commonly, concerns about the uncertainties of DIR prevent its adoption [11]. The accuracy of a DIR algorithm can only be assessed under controlled conditions, e.g. using physical or digital phantoms [12]. There is no standard procedure for estimating the uncertainty in real patient cases [13], but an indication is often sought through studying the consistency [4], [12], [14], e.g. between centres or between algorithms.
In the current analysis, we applied a structure-based evaluation of the DIR uncertainty in a cohort of reirradiated HNC cases, as an indication of the accuracy in this anatomical region at reirradiation, for one commercially available DIR algorithm. The specific aim was to estimate the uncertainty in accumulated dose metrics used to derive previously published dose–response relationships.
Material and methods
2
Dataset and dose accumulation
2.1
A sample of fifteen out of 54 cases from the study on side effects after HNC reirradiation [6], [9] were included in this analysis. These included the eleven most recent cases (one of which had ORN), and four additional cases with ORN and/or carotid blowout. The study was approved by the Swedish Ethical Review Authority.
The dose accumulation for the reirradiation study, and the corresponding image registrations, were performed in a research version (2023BR) of RayStation (Raysearch Laboratories, Stockholm, Sweden), after importing the treated plans from the original treatment-planning system. There were two computed tomography (CT) image sets per patient (primary treatment and reirradiation). For each patient, the most recent image set (used for treatment planning at reirradiation) was appointed reference. For all the sets of treatment plans, an initial rigid registration was performed, followed by an intensity-based DIR. The rigid registration prioritised agreement in the dose overlap region, with manual adjustments after the initial automatic registration. The DIR algorithm used was ANACONDA [15], which is proprietary to RaySearch. Further details about the performed image registrations are given in the supplementary materials.
Each dose distribution was converted to EQD2 in RayStation, using α/β = 3 Gy. The EQD2 distribution corresponding to the primary treatment was propagated to the reference image set, followed by an accumulation of the primary- and the reirradiation EQD2 distributions in the reference (reirradiation) image set.
Estimation of image registration uncertainty
2.2
Structure-based evaluation of the image registrations was performed. The supplementary materials include details on the OAR delineations. As carotid blowout and ORN were among the severe side effects in our cohort, and dose constraints were suggested in relation to these endpoints, the carotids and mandible were of particular interest (although not all cases of ORN developed in the mandible). The spinal cord and the larynx were also included, as relevant structures for dysphagia and myelopathy, respectively. Some cases of severe dysphagia were observed in the original cohort, but no myelopathy.
A quantitative evaluation of the geometrical uncertainty was performed by comparing the structures propagated from the primary treatment to the reference treatment-planning CT scan and the corresponding structures delineated directly in the reference image. A set of commonly used structure-based metrics with complementing strengths were calculated (e.g. [13]): the mean- and maximum distance to agreement, respectively (DTA_mean_ and DTA_max_), and the Dice similarity coefficient (DSC) [16]. These chosen metrics and their application are discussed in the supplementary materials.
Finally, the uncertainty in accumulated dose was estimated by evaluating the consistency between a dose metric of interest for the propagated structures, and for the structures delineated directly in the reference image set, respectively. For the carotids, the near maximum dose (D_1cm3_, i.e. the minimum dose to the hottest 1 cm^3^ of the volume) was considered, for the left and right carotid independently. This metric was used also for the mandible and the spinal cord, while for the larynx, the mean dose (D_mean_) was considered more relevant. Notably, this uncertainty estimation did not evaluate the actual dose mapping error, i.e. the variation in accumulated dose per voxel resulting from different image registrations.
Results
3
The visual evaluation of the registrations, using blending of the fused CT images and structure comparison, showed only small deviations (example in Fig. S1 in the supplementary materials), despite relatively large anatomical changes from the primary treatment to the reirradiation, in some cases.
With regard to the geometrical uncertainty, the results for the mandible and the spinal cord were excellent, with a median DTA_mean_ of 0.6 mm (inter-quartile range (IQR) = 0.5–1.2 mm) and 1.0 mm (IQR = 0.8–1.2 mm), respectively (Table 1, Table S1 and Figs. S2–S3). The carotids and the larynx showed a slightly higher median DTA_mean_ of 1.6 mm (IQR = 1.4–2.1 mm) and 1.8 mm (IQR = 1.7–2.2 mm), respectively. In addition to the overall discrepancies, larger local discrepancies were common, as quantified by DTA_max_. The median DTA_max_ ranged from 6.8-8.0 mm for all OAR except the spinal cord which had a value of 4.2 mm (IQR = 3.0–5.1 mm). There were 7 cases of a structure exceeding 15 mm in DTA_max_.Table 1. Mean- and maximum distance to agreement in millimeter.Carotid_LCarotid_RMandibleLarynxSpinal cordCaseDTA_mean_DTA_max_DTA_mean_DTA_max_DTA_mean_DTA_max_DTA_mean_DTA_max_DTA_mean_**DTA_max_13.112.43.112.83.151.72.313.81.25.121.76.22.37.50.35.21.96.40.94.731.89.11.46.10.66.81.67.80.82.941.57.61.04.50.34.31.89.41.04.451.49.41.67.60.34.31.57.10.82.961.25.70.93.41.311.91.87.71.33.173.917.35.216.20.58.65.719.41.25.381.37.81.47.30.43.00.94.01.07.091.97.60.94.71.612.61.87.50.72.4101.57.22.710.70.56.82.29.50.83.5111.69.92.112.30.622.22.79.41.25.1121.65.71.65.91.03.2−*−0.83.1132.110.22.115.32.958.21.88.41.44.2143.19.32.111.80.98.72.18.12.118.7151.37.81.24.70.56.01.45.90.00.3Median1.67.81.67.50.66.81.88.01.04.2IQR1.5–2.07.4–9.71.3–2.25.3–12.00.5–1.24.8–12.31.7–2.27.2–9.40.8–1.23.0–5.1 Missing value due to laryngectomyIQR = inter-quartile range
For the carotids, all except 6 (out of 30) propagated structures showed a discrepancy of 4 Gy (in EQD2) or less from the reference (delineated directly in the treatment-planning CT); this number was 2/15 for the mandible, 3/14 for the larynx (one patient had had a laryngectomy) and 0/15 for the spinal cord (Table 2 and Fig. S4). Since most of the outliers accumulated in a few patients (see supplementary materials), the discrepancy in the dose metric was 4 Gy or less (in EQD2) for 8/15 patients, and despite these outliers, the median value of the absolute difference in the full cohort was: 1.0 Gy (IQR = 0.4–3.9 Gy) in carotid D_1cm3_, 0.2 Gy (IQR = 0.1–3.0 Gy) in mandible D_1cm3_, 1.1 Gy (IQR = 0.8–1.7 Gy) in larynx D_mean_, and 0.5 Gy (IQR = 0.3–1.1 Gy) in spinal cord D_1cm3_. Please refer to the supplementary materials for details about outliers, a correlation analysis between geometric and dosimetric uncertainty metrics and the commissioning of the DIR tool.Table 2. Accumulated dose (EQD2, Gy) to OAR computed in the reference structure (Ref.) and the propagated structure (Prop.), respectively.Carotid_L D_1cm3_Carotid_R D_1cm3_Mandible D_1cm3_Larynx D_mean_Spinal cord D_1cm3_CaseRef.Prop.Ref.Prop.Ref.Prop.Ref.Prop.Ref.Prop.197.797.38.29.2133.2133.312.510.817.518.8252.352.497.0105.471.771.739.538.734.435.5393.092.564.668.2121.0121.248.247.636.636.5447.247.512.812.8110.7107.91.22.121.521.3594.594.713.413.3131.0131.025.023.835.934.8680.881.766.066.4113.7113.643.637.131.631.1787.395.598.3108.790.390.973.981.349.248.6840.842.5119.5119.0112.8111.224.125.044.244.79113.8117.574.572.8115.9123.643.942.335.435.71051.552.966.470.462.962.944.943.819.919.61174.073.649.449.7103.599.961.168.745.945.912126.0125.176.376.2112.8109.6−*−38.939.01395.4114.681.975.499.7122.446.247.435.733.814117.7115.765.069.1121.1120.851.550.632.634.31567.873.217.418.472.272.21.11.323.223.7 Missing value due to laryngectomy
Discussion
4
With the commercial solution for DIR used in the current analysis, we found the geometrical uncertainties in DIR to be generally small, in the setting of HNC reirradiation. The uncertainty in accumulated OAR dose was around 2–4 Gy (EQD2), with a median below 1 Gy (EQD2). This corresponds to 2–3 % of the mandible- and carotid dose-constraint of 119 Gy (EQD2). However, outliers can be expected for OAR like the carotids (low CT contrast, and a branching structure which can adapt its shape to the surrounding anatomy), and in cases of steep dose gradients or extreme anatomical changes from the primary setting to the reirradiation setting. The carotids appear vulnerable to such factors (see discussion about outliers in supplementary materials) and need to be evaluated carefully in the fused images before relying on DIR-based dose accumulation.
Quantitatively, the DTA_mean_ was typically around 2 mm or less, which indicates good conformity, as this is less than the voxel size and acceptable by previously suggested standards [19]. The median discrepancy in the dose metric was only up to 1.1 Gy, for all OAR analysed. Still, for the carotids, D_1cm3_ deviated more substantially in a few cases. When retrospectively reviewing the two cases of carotid blowout reported in our previous work [6], the carotids were confirmed to have been integrated in a relatively uniform dose overlap region, and they were clearly visible without interference from dental artefacts. Thus, the suggested dose constraint for carotid blowout is unlikely to suffer from major image-registration related uncertainty. The relevance of the geometric uncertainty metrics is discussed in the supplementary materials.
For the mandible, the deviation in D_1cm3_ was less than 4 Gy for all cases except two, indicating a low uncertainty except in cases of surgical resection. One of the patients with ORN in our previous work was such a case, but the ORN was located in the maxilla (with bone D_1cm3_ exceeding mandible D_1cm3_, and the hotspot located in the maxilla). Therefore, the uncertainty in the previously suggested dose constraint for ORN is expected to be reliable from a geometrical consideration. Even though ORN developed in the mandible in only one of the cases from that study, and the dose was thus evaluated in the general bone structure, the uncertainty can be expected to be similar or lower for bone compared to the mandible specifically. Similarly, the uncertainty in the accumulated dose to the spinal cord was very low, likely aided by the rigid anatomy and the clear image contrast for the vertebrae. For a discussion of the reliability and generalisability of the dosimetric uncertainty metrics, please see the supplementary materials.
In the setting of reirradiation, the uncertainty in the accumulated dose to OAR needs to be considered when applying a dose constraint [4]. In regions of poor agreement between fused images, it can be unsafe to consider DIR-based accumulated dose. Here, the best approach may be to consider a worst-case scenario, based on e.g. the maximum dose in EQD2 for the respective treatments, either globally or regionally. Where DIR-based dose accumulation is performed, planning risk volumes should be used to avoid steep dose gradients adjacent to OAR sensitive to hot spots, similarly to the primary treatment setting. The size of the margin should then take the uncertainty in the DIR into account.
The methods used to manage the image-registration related uncertainty in the current analysis follow current recommendations [13], [17], [18], including commissioning of the DIR tools, and evaluation of both the geometrical and the dosimetric uncertainty. The analysis considers a relatively simplistic estimate of the dosimetric uncertainty, with a focus on the consistency of dose metrics of interest, rather than on the actual dose mapping error. This consistency was evaluated from a single accumulated dose distribution, comparing different versions of the OARs. The selected approach followed from the aim to verify previously published dose constraints. For extended discussions regarding strengths, weaknesses and interpretations of the results, please refer to the supplementary materials.
In conclusion, the geometric uncertainty of the current DIR methodology was in the order of the voxel size for most of the cases, and OAR. However, local uncertainties of 1–2 cm were not uncommon. Specifically, regarding our previously suggested dose constraints for carotid blowout and ORN, these appear to be reliable with regard to the underlying DIR, based on the magnitude of the uncertainty demonstrated in the current analysis, and specific evaluation of the reported cases of severe side effects.
CRediT authorship contribution statement
Sara Bornedal: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. Jeehong Lee: Data curation, Investigation, Methodology, Writing – review & editing. Tim Melhus: Investigation, Methodology, Supervision, Writing – review & editing. Anna Embring: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing – review & editing. Eva Onjukka: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mayo C.S.Appelt A.L.Paradis K.C.Dawson L.A.Andratschke N.Vasquez Osorio E.M.Joining forces to advance reirradiation: establishing the Reirradiation C Ollaborative Group (Re COG)Int J Radiat Oncol Biol Phys 122202523424010.1016/j.ijrobp.2025.01.03840088225 · doi ↗ · pubmed ↗
- 2Vasquez Osorio E.Mayo C.Jackson A.Appelt A.Challenges of re-irradiation: a call to arms for physicists - and radiotherapy vendors Radiother Oncol 182202310958510.1016/j.radonc.2023.10958536842664 · doi ↗ · pubmed ↗
- 3West N.Covington E.Vasquez Osorio E.Stroom J.Duchateau M.Day M.Consistency in reirradiation scenarios: terminology, tissue recovery in calculations, units and reporting Radiother Oncol 202202511058710.1016/j.radonc.2024.11058739423959 · doi ↗ · pubmed ↗
- 4Hardcastle N.Vasquez Osorio E.Jackson A.Mayo C.Aarberg A.E.Ayadi M.Multi-centre evaluation of variation in cumulative dose assessment in reirradiation scenarios Radiother Oncol 194202411018410.1016/j.radonc.2024.11018438453055 · doi ↗ · pubmed ↗
- 5Willmann J.Appelt L.Balermpas P.Baumert G.de Ruysscher D.Hoyer M.Re-irradiation in clinical practice: results of an international patterns of care survey within the framework of the ESTRO-EORTC E 2-RAD Iat E platform Radiother Oncol 189202310994710.1016/j.radonc.2023.10994737806559 · doi ↗ · pubmed ↗
- 6Embring A.Onjukka E.Mercke C.Lax I.Berglund A.Bornedal S.Re-irradiation for head and neck cancer: cumulative dose to organs at risk and late side effects Cancers 132021317310.3390/cancers 1313317334202135 PMC 8269009 · doi ↗ · pubmed ↗
- 7Garg S.Kilburn J.M.Lucas J.T.Jr.Randolph D.Urbanic J.J.Hinson W.H.Reirradiation for second primary or recurrent cancers of the head and neck: dosimetric and outcome analysis Head Neck 38Suppl 12016 E 961E 96910.1002/hed.2413625993910 PMC 9176709 · doi ↗ · pubmed ↗
- 8Bots W.T.C.van den Bosch S.Zwijnenburg E.M.Dijkema T.van den Broek G.B.Weijs W.L.J.Reirradiation of head and neck cancer: long-term disease control and toxicity Head Neck 3920171122113010.1002/hed.2473328263446 PMC 5485062 · doi ↗ · pubmed ↗