Retroperitoneal lymph node dissection for growing teratoma syndrome in testicular cancer: a systematic review of surgical outcomes
Alberto Costa Silva, Afonso Morgado, João Alturas Silva, Pedro Oliveira, Noel Clarke, Rui Almeida Pinto, Aziz Gulamhusein

TL;DR
This review examines the surgical outcomes of retroperitoneal lymph node dissection for treating testicular cancer-related growing teratoma syndrome.
Contribution
The study provides a systematic review of surgical and oncological outcomes for retroperitoneal GTS management.
Findings
RPLND is effective for GTS, with disease-free survival rates between 41.7% and 100%.
Postoperative complications occurred in 12.5–44% of patients, with hospital stays ranging from 5 to 15 days.
Multicenter registries are recommended to improve data quality for GTS treatment.
Abstract
Growing Teratoma Syndrome (GTS) is a rare entity occurring in patients with non-seminomatous germ cell tumours (NSGCT) following chemotherapy. GTS is resistant to chemotherapy and radiotherapy, making retroperitoneal lymph node dissection (RPLND) the mainstay of treatment. This review aims to synthesize evidence on the surgical management and oncological outcomes of retroperitoneal GTS. A systematic review was conducted in accordance with PRISMA guidelines and registered in PROSPERO (CRD420251233173). PubMed and Embase were searched from inception to November 2025. Risk of bias was assessed using the ROBINS-I tool. Fifteen studies comprising 156 patients with NSGCT-associated retroperitoneal GTS treated with RPLND were included. The reported incidence ranged from 2.8% to 7.6%. Median patient age across studies was 16–38 years. Mixed NSGCT was present in 73–100% of orchidectomy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
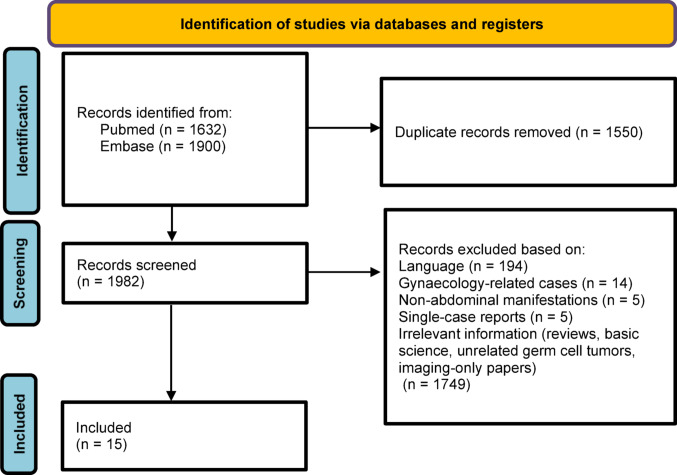 Figure 1
Figure 1- —Universidade do Porto
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Teratomas and Epidermoid Cysts · Neuroblastoma Research and Treatments
Introduction
Growing Teratoma Syndrome (GTS) is a rare clinical entity first described by Logothetis et al. in 1982 in the context of non-seminomatous germ cell tumours (NSGCTs) [1]. It is defined by the growth of masses during or after chemotherapy, despite normalization of serum tumour markers. Histologically, GTS is confirmed by the presence of teratoma tissue in the surgical specimen. The incidence of GTS has been reported in up to 7.6% of cases, occurring predominantly in the retroperitoneum [1, 2].
GTS pathogenesis remains poorly understood, reflecting a complex interplay of cellular differentiation, selective chemoresistance, and potential molecular reprogramming during treatment [3]. Clinically, GTS presents a management challenge. It is unresponsive to both chemotherapy and radiotherapy, and delayed recognition may result in significant morbidity due to tumour bulk or compression of adjacent structures. Moreover, mature teratoma tissue carries a risk of somatic-type malignant transformation [3, 4]. Surgical removal of retroperitoneal teratoma masses via retroperitoneal lymph node dissection (RPLND) remains the standard approach for managing GTS.
The present systematic review aims to analyse the current data on retroperitoneal GTS associated with testicular cancer, focusing on patient characteristics, RPLND metrics and oncological outcomes.
Methods
Evidence acquisition
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration ID: CRD420251233173).
Search strategy
A comprehensive literature search was carried out in PubMed/MEDLINE and Embase databases from inception to November 2025. The search strategy incorporated both free-text and MeSH terms (Supplementary material 1). Only articles published in English were considered. Reference lists of relevant articles were manually screened to identify additional eligible studies. Inclusion and eligibility criteria was determined using the PICOS framework (Supplementary material 2). Studies were excluded if they: included exclusively gynaecological or non-abdominal GTS cases; single case reports; included testicular GTS cases but did not provide granular data relevant to the review objectives; conference abstracts, or papers not published in peer-reviewed journals.
Study selection and data extraction
Two reviewers independently screened all titles and abstracts, followed by full-text evaluation (ACS and AG). Discrepancies were resolved by a third reviewer (NC). A standardised data collection form was used to extract study characteristics (author, year, country), number of patients, age, type of primary tumour, type of chemotherapy used before RPLND, interval to RPLND (the time between orchidectomy and RPLND), surgical outcomes (RPLND time, blood loss, adjunctive procedures), complication rates (stratified by Clavien-Dindo classification), and follow-up outcomes. For continuous variables, median and range values were reported.
Risk of bias assessment
The methodological quality of included studies was appraised using Risk of Bias In Non-randomised Studies of Interventions (ROBINS-I version 2) tool [5]. Each study was independently assessed by two reviewers (ACS and AG), and disagreements were resolved by a third party (NC). The results are presented in Supplementary Material 3.
Results
Search results
Overall, 3532 articles were found. After screening and eligibility assessment, 15 studies met the inclusion criteria (Fig. 1), including a total of 156 patients [1, 2, 6–18]. Data spanned from 1971 to 2019, including retrospective case series. The main characteristics of the included studies are provided in Table 1.
Fig. 1PRISMA flow diagram of study inclusion
Table 1. Summary of studies characteristicsStudyCountry Inclusion yearsNumber of patientsAgeyearsmedian (range)HistologyOrchidectomy,%Interval to RPLNDmonthsmedian (range)ChemotherapyHistology RPLND(%)Operative timeminutesmedian (range)EBLmLmedian (range)Adjunctive procedureComplications (CD, %)LOSdaysmedian (range)FU monthsmedian (range)OutcomesPrineethie et al., 2022 [17]India, 2001–2019727 (17–48)Mixed NSGCT: 100%. Teratoma component: NRNRBEPMT: 100%NRNRNRNRNRNRAll patients alive and disease-freeHsieh et al., 2022 [18]Taiwan, 2005–2019216 (25 − 16)Mixed NSGCT: 100%Teratoma component: NR30 (3–56)NRMT: 100%NRNRNRNRNR77 (16–137)All patients alive and disease-freeAcikgoz et al., 2021 [16]Turkey, 2004–20181229 (17–51)Mixed NSGCT: 89%Teratoma component: NRMT: 11%10 (4-104)BEPMT: 100%NRNRNRNRNR61 (8-184)Disease-free:41.7% Relapse: 58.3% (salvage TIP) 5-year OS: 73.7%Paffenholz et al., 2018 [14]Germany,2000–20162228 (22–34)Mixed NSGCT: 73%Teratoma component: 40%MT: 9.1%Pure EC: 9.1%Pure YST: 9.1%NRBEP, EP, PEIMT: 100%160 (142–320)300 (175–450)18%-Aorta resection + graft: 2-Cava resection + graft: 1-Resection of renal vein + Graft:1-Nephrectomy: 1-Bowel resection: 123%CD ≥ III: 18%-Hematoma with drainage: 1-Necrotizing pancreatitis: 1-Bowel perforation: 1-Bowel ischemia:110 (9–14)25Relapse: 9%Alive: 95.5%.Scavuzzo et al., 2014 [15]Mexico, 2014226 (23–28)Mixed NSGCT: 100%Teratoma component: 100%9 (5–12)BEPMT: 100%255 (250–360)2500NRNR5 (3–6)9 (8–10)All patients alive and disease-freeLee et al., 2014 [13]USA, 2005–20121523 (16–39)Mixed NSGCT: 80% Teratoma component:40% SGCT: 13% Unknown: 7% (after chemotherapy)3 (2–45)BEPMT: 100%372 (252–912)600 (100–7000)33%-Nephrectomy: 1-Renal artery anastomosis: 1-Renal arteryembolectomy: 1-IVC thrombectomy: 1-Resection of iliac vein: 127%CD ≥ III: 13%-Arytenoid dislocation: 1-Bilateral renal ischemia: 15 (3–19)8 (5–64)All alive and disease-freeStella et al., 2012 [12]France, 1992–20101229 (19–38)Mixed NSGCT: 75%. Teratoma component: NR Chorio: 16.7%. EC: 8.3%NRBEPMT: 91.7%MT + LMS: 8.3%NR225 (10-4000)100%-Aorta sectioningand anastomosis: 6-IVC resection: 3-Aorta sectioning andanastomosis + IVC resection: 1-Infrarenal aortic graft + nephrectomy: 225%CD ≥ III: 25%-Small bowelocclusion and surgery: 1-Perforated duodenal ulcer and surgery: 1 -Lymphocele requiring drainage: 115 (9–50)59 (10–262)Disease-free: 83.3%. Recurrence: 8.3% Death: 8.3% (melanoma)Spiess et al., 2007 [11]USA, 1980–2003919 (16–53)Mixed NSGCT: 89%Teratoma component: NRMT: 11%5 (3–21)NRMT: 100%432 (276–990)600 (200-11650)22%-Aortic repair: 1-Ureteral repair: 144%CD ≥ III: 22%-Chylous ascites with drainage: 1. -Death due to sepsis: 1NR24 (7-137)Disease-free: 77.8%5-year OS: 89%Andre et al., 2000 [10]France, 1985–19973029 (15–38)MT: 86% Mixed NSGCT: 10.7%. Teratoma component: NR Seminoma 3.3%20 (5–66)BEPMT: 100%NRNR10%-IVC thrombectomy: 3-Nephrectomy: 1NRNR48 (3–80)Alive: 90%Disease-free: 66.6%Maroto et al., 1997 [9]Spain, 1979–19941121 (16–50)Mixed NSGCT: 90.0%. Teratoma component: 82% EC: 9.1%9 (7–13)BEP, PVB, BOMP-EPIMT: 100%NRNRNRNRNR103 (33–179)Alive: 100% Disease-free: 54.5%Ravi et al., 1995 [8]India, NR338 (32–48)Mixed NSGCT: 100%Teratoma component: 100%NRBEP, IPVBMT: 100%NRNRNRNRNR22 (6–26)All alive and disease-freeTongaonkar et al., 1994 [7]India, NR424 (15–33)Mixed NSGCT: 100%Teratoma component: 75%NRBEP, VAB-6MT: 100%NRNRNRNRNR21 (6–36)All alive and disease-freeJeffery et al., 1991 [2]United Kingdom,1977–19901325 (17–47)Mixed NSGCT: 82%. Teratoma component: 77% Unknown: 8% (chemotherapy)2 (1–25)BEP, PVB, POMB/ACE,Teratoma: 100%. -AC: 7.7%NRNRNRNRNR20 (1–68)Disease-free: 80%. Alive: 92.3%Tonkin et al., 1989 [6]UK, 1977–1987821 (15–26)NSGCT: 100% Teratoma component: NR.4 (1–6)POMB/ACEMT: 100%NRNRNR12.5%CD ≥ III: 12.5%-Death from aortic rupture:1NR34 (8–60)Alive and disease-free: 75%Logothetis et al., 1982 [1]USA,1971–1980622 (16–32)Mixed NSGCT 83.3%. Teratoma component: 83.3% EC − 16.7%15 (8–19)#NRNRNRNRNRNR20 (5-108)All alive and disease-freeAC: adenocarcinoma; B-COMF: Bleomycin, Cyclophosphamide, Vincristine (Oncovin), Methotrexate, 5-Fluorouracil; BEP: Bleomycin, Etoposide, Cisplatin; CD: Clavien-Dindo classification; Chorio: choriocarcinoma; CISCA: Cyclophosphamide, Adriamycin (doxorubicin), Cisplatin; EC: Embryonal carcinoma; EBL: Estimated blood loss; EP: Etoposide, Cisplatin; FU: Follow-up; IPVB: Ifosfamide, Cisplatin, Vinblastine, Bleomycin; LOS: Length of stay; LMS: leiomyosarcoma; max: maximum; min: minimum; MT: Mature teratoma; NSGCT: Non-seminomatous germ cell tumor; OS: Overall survival; P: Cisplatin; PEI: Cisplatin, Etoposide, Ifosfamide; POMB/ACE: Cisplatin, Vincristine, Methotrexate, Bleomycin / Actinomycin D, Cyclophosphamide, Etoposide; PVB: Cisplatin, Vinblastine, Bleomycin; RPLND: Retroperitoneal lymph node dissection; TIP: Paclitaxel, Ifosfamide, Cisplatin; VB: Vinblastine; VAB-6: Vinblastine, Actinomycin D, Bleomycin, Cisplatin, Cyclophosphamide, Hydroxyurea; VIP: Etoposide, Ifosfamide, Cisplatin; XRT: Radiation therapy; YST: Yolk sac tumor; # VB + P; XRT, VB + P, B-COMF; VB, Adriamycin, Bleomycin, VP-16; VB, B-COMF; VB + P, B-COMF; Adriamycin, Bleomycin, VP-, CISCA II, VB
Evidence synthesis
The incidence of GTS among patients with NSGCT treated with chemotherapy was reported to range from 2.8% to 7.6% (2 studies) and the median age of presentation ranged from 16 to 38 years. Mixed NSGCTs were observed in 73–100% of cases (15 studies), with a teratoma component identified in 40–100% of these mixed tumours (7 studies). The teratoma component within mixed NSGCTs was 50–80% of the tumour volume (1 study) and pure mature teratoma was observed in 9–11% of orchidectomy specimens (3 studies). The median interval until RPLND ranged from 2 to 30 months. Most studies reported the use of BEP chemotherapy prior to RPLND (11 studies), with chemotherapy interruption required in 4.5% due to compressive symptoms (1 studies). Symptoms associated with the enlarging mass were reported in 50% to 83.3% of cases, with documented growth rates ranging from 0.5 to 0.7 cm per month (2 studies).
Pathological evaluation of RPLND specimens revealed mature teratoma in 91.7–100% (14 studies), with somatic-type malignant transformation observed in 7.7–8.3% of cases (2 studies). The median operative time for RPLND ranged from 160 to 432 min (4 studies), and estimated blood loss (EBL) varied from 225 mL to 2500 mL (5 studies). Adjunctive procedures were required in 10% to 100% of patients and median length of hospital stay (LOS) ranged from 5 to 15 days. (4 studies). Postoperative complication rates ranged from 12.5% to 44%, with Clavien-Dindo grade ≥ III complications occurring in 12.5% to 25% of patients (5 studies).
Follow-up ranged from 8 to 103 months (14 studies). At last follow-up, disease-free survival ranged from 41.7% to 100%, and overall survival from 73.7% to 100% (15 studies).
Discussion
GTS remains a rare but clinically significant scenario in patients with NSGCT, with its pathogenesis still not fully understood. Despite the time elapsed since its initial description in 1982, limited published data continues to hinder consensus on its management and biological behaviour. Several hypotheses have been proposed to explain the development of GTS. One suggests that chemotherapy alters the kinetics of totipotent malignant germ cells, prompting their transformation into benign mature teratomatous components [19]. The retroconversion theory posits that chemotherapy destroys only the immature malignant cells, leaving behind mature benign teratomatous elements that continue to grow [20]. A third hypothesis considers the possibility of spontaneous differentiation of malignant cells into non-malignant components during treatment [21]. More recently, a molecular model has been proposed in which embryonal carcinoma cells differentiate into teratoma-forming transit amplifying cells capable of self-renewal or further differentiation into tissues of all three germ layers [4]. A recent study integrating transcriptional and proteomic profiling with tumour growth rate stratification proposed that specific biomarkers may aid in identifying GTS and anticipating its growth behaviour. Also, the authors advocate for an updated definition of GTS, describing it as a “continuously growing teratoma that might harbour occult non-seminomatous components considerably reduced during therapy but outgrowing over time again” [22]. Together, these theories highlight the complex and multifactorial nature of GTS pathogenesis.
Our systematic review aggregates data from 15 studies over five decades, involving 156 patients with an incidence up to 7.6% of patients with NSGCT treated with chemotherapy [2, 6]. Teratoma was identified in most orchidectomy specimens, although it was not always the predominant histological component, and some authors have questioned its predictive value for subsequent GTS development [4]. Teratoma was consistently present in the RPLND specimens, with two studies reporting cases of somatic-type malignancy, which is a recognised risk associated with teratoma progression.
Due to the resistance of GTS to both chemotherapy and radiotherapy, RPLND remains the cornerstone of treatment and is generally performed after systemic therapy is completed. However, over half of patients may experience compressive symptoms such as abdominal pain, acute renal failure, obstructive pyelonephritis or bowel obstruction [12, 15]. In rare cases, chemotherapy may need to be interrupted to allow surgical intervention due to life-threatening organ compression, as reported in one study (4.5%) [14]. Radiologically, these masses appear partially cystic, often multiloculated, with enhancing septations, progressive enlargement, and expanding cystic areas [17, 23]. The growth pattern is highly unpredictable, though some reports document rates between 0.5 and 0.7 cm per month [11, 13].
The surgical complexity is significant, with studies reporting high rates of adjunctive procedures including nephrectomies, bowel and major vascular resections, which reflects the local behaviour of GTS despite its benign histology. However, the wide range of adjunctive procedure rates (10% to 100%) likely reflects differences in patient selection, as the study reporting 100% involved a vascular surgery-led cohort that may not be representative. When excluding this outlier, reported rates range from 10% to 33%. The broad variation in median operative time (160–432 min), blood loss (225–2500 mL), and length of hospital stay (5–15 days), along with major postoperative complications (Clavien-Dindo ≥ III) reported in up to 25% of patients, further underscore the procedural heterogeneity and technical challenges involved. The wide interval to RPLND (8–103 months) may reflect a spectrum of GTS phenotypes, ranging from early aggressive to late indolent presentations. However, none of the included studies evaluated whether timing influenced surgical complexity or clinical outcomes.
From an oncological perspective, disease-free and overall survival rates were high. However, details regarding management of recurrence after RPLND were underreported, particularly the need for additional surgical resection or systemic therapy.
This systematic review has several limitations. All included studies were retrospective case series with limited patient numbers and inconsistent follow-up durations. There was substantial heterogeneity in the reporting of surgical outcomes, histopathological details, and follow-up, resulting in uneven data availability with some outcomes being reported in only one study, while others were consistently documented across all included studies, which also precluded a meta-analysis. Moreover, the risk of bias across the included studies imposes caution when interpreting the findings. The rarity of the condition, combined with inconsistent reporting, underscores the challenges in drawing conclusions. Data about reporting extra-abdominal manifestations of GTS were excluded, although it is noteworthy that the syndrome can present in diverse locations including the lungs, cervical and inguinal lymph nodes, mediastinum, forearm, mesentery, liver, and pineal gland [18, 23, 24]. These presentations often require distinct management strategies beyond the urological domain, although multidisciplinary surgical collaboration can be necessary to achieve complete resection.
This syndrome rarity and complexity further highlight the importance of centralizing testicular cancer care in high-volume, specialized centres with experienced multidisciplinary teams [25]. Multicentre collaborative databases and prospective registries are crucial for generating high-quality, standardised data on patients with GTS in the context of testicular cancer.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jeffery GM, Theaker JM, Lee AHS, Blaquiere RM, Smartand CJ, Mead GM (1991) The growing teratoma syndrome ; volume 61, pages 195-202 , DOI 10.1111/j.1464-410x.1991.tb 15109.x 10.1111/j.1464-410x.1991.tb 15109.x 2004236 · doi ↗ · pubmed ↗
- 2Salzillo C et al (2024) Gonadal teratomas: a state-of-the-art review in pathology. Multidisciplinary Digital Publishing Institute (MDPI) 10.3390/cancers 1613241210.3390/cancers 16132412 PMC 1124072939001474 · doi ↗ · pubmed ↗
- 3Hiester A, Nettersheim D, Nini A, Lusch A, Albers P (2019) Management, treatment, and molecular background of the growing teratoma syndrome. 10.1016/j.ucl.2019.04.00810.1016/j.ucl.2019.04.00831277736 · doi ↗ · pubmed ↗
- 4Tonkin KS, Rustin GJS, Wignall B, Paradinas F, Bennett+ M (1989) Successful treatment of patients in whom germ cell tumour masses enlarged on chemotherapy while their serum tumour markers decreased. European Journal of Cancer, Volume 25, Issue 12 , page 1739-1743 ;10.1016/0277-5379(89)90343-X 10.1016/0277-5379(89)90343-x 2483686 · doi ↗ · pubmed ↗
- 5Tongaonkar H 6, Deshmane VH, Dalal AV, Kulkarni JN, Kamat MR (1994) Growing teratoma syndrome , Journal of Surgical Oncology 55:56-60 (1994) ,10.1002/jso.293055011610.1002/jso.29305501168289455 · doi ↗ · pubmed ↗
- 6Maroto P et al (1997) Growing teratoma syndrome: experience of a single institution. European Urology, volume 32, pages 305-309 , DOI 0302-2838/97/0323-0305$ 12.00/0 9358218 · pubmed ↗
- 7Andre F et al The growing teratoma syndrome: results of therapy and long-term follow-up of 33 patients. volume 36, page 1389-1394 , DOI: 10.1016/s 0959-8049(00)00137-4 10.1016/s 0959-8049(00)00137-410899652 · doi ↗ · pubmed ↗
- 8Hong WK, Wittes RE, Hajdu ST, Cvitkovic E, Whitmore WF, Golbey RB (1977) The evolution of mature teratoma from malignant testicular tumors; volume 40; pages 2987-2992; DOI: 10.1002/1097-0142(197712)40:6<2987::aid-cncr 2820400634>3.0.co;2-a 10.1002/1097-0142(197712)40:6<2987::aid-cncr 2820400634>3.0.co;2-a 563283 · doi ↗ · pubmed ↗