Effectiveness of remineralizing dentifrices against caries lesions: A systematic approach
Fatima T. Zahra, Mehmood Asghar, Muhammad S. Zafar, Asma T. Shah, Muhammad Kaleem

TL;DR
This study reviews how well remineralizing toothpastes, like those with bioactive glass, work to repair early tooth decay compared to fluoride-only products.
Contribution
The paper systematically compares the effectiveness of bioactive glass and CPP-ACP dentifrices against fluoride-only ones in remineralizing caries lesions.
Findings
Bioactive glass-based dentifrices showed greater mineral deposition and improved surface microhardness than fluoride-only products.
CPP-ACP and bioactive glass outperformed fluoride in reducing lesion depth in in vitro studies.
Methodological issues like limited randomization and small sample sizes reduced the reproducibility of results.
Abstract
Dental caries remains a prevalent global oral health problem. Fluoride promotes enamel remineralization but is less effective on deeper lesions. Non-invasive agents, including bioactive glass and casein phosphopeptide-amorphous calcium phosphate (CPP-ACP), aim to enhance remineralization and prevent caries. A systematic review of in vitro studies was conducted following PRISMA 2020 guidelines. PubMed, Ovid, Cochrane Library, ScienceDirect, and Scopus were searched for studies published before 31 December 31, 2024. Titles, abstracts, and full texts were screened independently by two reviewers. Risk of bias was assessed using a modified CONSORT checklist. Among 142 records identified, 38 were screened, 21 full texts retrieved, and 11 studies met the inclusion criteria. Bioactive glass-based dentifrices generally outperformed fluoride-only formulations, with greater mineral deposition,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1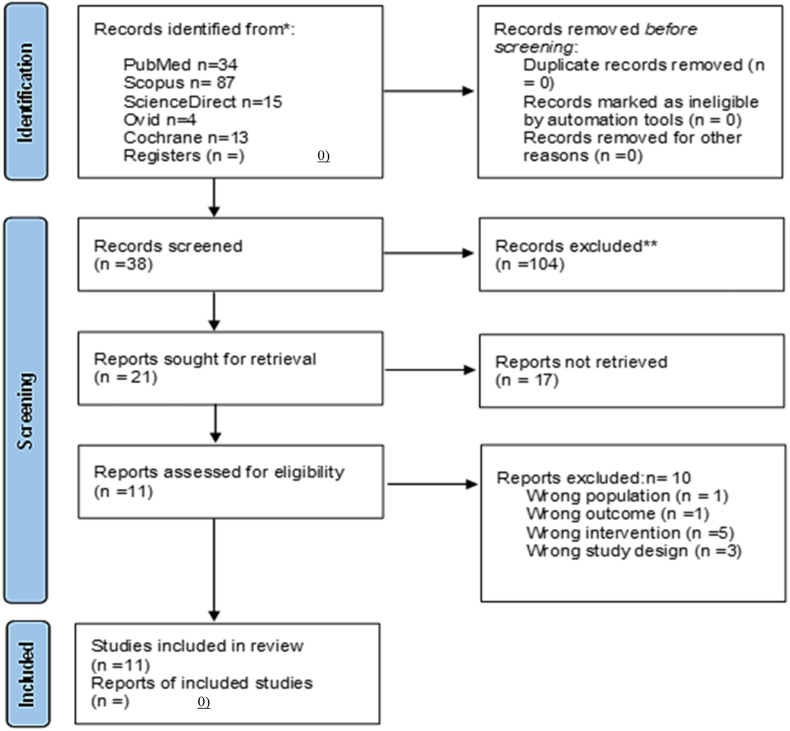 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Dental Erosion and Treatment · Dental materials and restorations
Introduction
Dental caries remains one of the most prevalent oral health problems worldwide, affecting individuals in all age groups.1, 2, 3 The progression of caries involves an imbalance between demineralization and remineralization, leading to loss of minerals from the enamel and dentine surface due to acid production by cariogenic bacteria..4 Traditional fluoride-based intervention has long been used to enhance enamel remineralization and reduce lesion progression.5^,^6 However, fluoride alone has a limited effect on restoring the lost mineral content in deeper lesions, thereby prompting research into alternative bioactive remineralization strategies.6^,^7 In particular, bioactive materials such as bioactive glass, casein phosphopeptide-amorphous calcium phosphate (CPP-ACP), and metal fluoride-modified formulations have emerged as promising agents for non-invasive caries management.8, 9, 10
Bioactive glass formulations consisting of calcium sodium phosphosilicate (e.g., Novamin) and fluoride-doped variants (e.g., BiominF) release calcium, phosphate, and fluoride ions to stimulate hydroxyapatite formation and remineralization.11, 12, 13 Similarly, CPP-ACP has been investigated for preventing demineralization and promoting enamel repair due to its calcium- and phosphate-stabilizing properties.8 Recent studies also suggest that incorporating these bioactive glass materials into dentifrices and preventive treatments can dramatically improve their ability to restore lost mineral contents and prevent lesion progression.14, 15, 16, 17, 18, 19, 20 The large amount of clinical evidence shows the promise of these approaches but methodological inconsistencies in in-vitro studies prevent the definition of clear clinical guidelines.15
Much of the research into remineralization is complicated by the wide diversity of protocols employed, with differences in the pH cycling methods, durations of demineralization and remineralization, and outcome measures.16 Moreover, many studies failed to apply critical methodological requirements such as randomization, blinding, and sample size justification, which are all essential for improving the validity and reproducibility of findings,21 making it difficult to determine the most effective remineralization strategies.22 Thus, it is necessary to thoroughly review in vitro studies and organize the data produced in an appropriate manner to obtain a better understanding of the advantages and disadvantages of different remineralization methods and their future implications.
Fluoride has been shown to influence enamel repair kinetics, with a threshold concentration above which remineralization ceases, highlighting the limitations of in vitro systems due to diffusion, crystal growth, and ion gradients.23 Considerable variability exists in terms of fluoride release and cariostatic efficacy among toothpastes and restorative materials,24^,^25 and clinical factors such as dentifrice use and diet further impact outcomes.26 In addition to fluoride, bioactive materials including bioactive glass, glass–ceramics, and calcium phosphate composites exhibit potential for enhancing enamel remineralization, although material-dependent differences persist.27, 28, 29 These findings highlight the need to specify standardized in vitro and clinical protocols for reliably assessing the remineralization potential and comparing similar results.
In the present study, a modified CONSORT checklist was used to systematically review the quality and methodological strength of in vitro studies of bioactive remineralization agents.30 By evaluating factors such as study design, intervention protocols, outcome measures, and statistical analysis, this review provides valuable insights into the reliability of current evidence, ultimately contributing to the development of more standardized and clinically relevant remineralization strategies, as depicted in Figure 1.Figure 1. Comparison of remineralization strategies for effective enamel repair.Figure 1
Methodology
Study objective and inclusion parameters
To assess the effectiveness of bioactive glass-containing dentifrices, metal fluoride formulations, and CPP-ACP at enhancing dentine remineralization and preventing caries progression based on in vitro evidence, a systematic review was performed following the updated guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA 2009). The following PICO framework was designed to address the research objective:
- •P (Population): In vitro studies of dentine remineralization
- •I (Intervention): Bioactive glass-containing dentifrices, metal fluoride formulations, and CPP-ACP
- •C (Comparison): Untreated control groups
- •O (Outcome): Mineral deposition, surface microhardness, lesion depth reduction, and overall remineralization effectiveness
Inclusion criteria
The reviewed articles were filtered using the following inclusion criteria to meet the aims of the reviewer.
- 1.All methodological approaches were deemed eligible.
- 2.The study used human or animal source (bovine) teeth with natural or artificially induced caries.
- 3.Studies that measured the remineralization efficacy of bioactive glass either alone or in combination with other agents.
- 4.Outcome measure: All studies related to remineralization, caries prevention, and safety.
- 5.Full-text articles available.
- 6.Written in English.
Exclusion criteria
- 1.Studies published in languages other than English were excluded.
- 2.Studies were excluded if the full text was not available.
- 3.Articles not focused on dentine caries
- 4.Animal studies, case reports, and case series.
- 5.Systematic review and grey literature
Literature search and selection
Article selection was conducted by two researchers. Five online databases were searched electronically for relevant literature. MEDLINE, PubMed, Ovid, Cochrane Library, and Scopus were searched to identify relevant studies published up to December 31, 2024 (Table 1). Medical subject headings (MeSH) and Boolean operators were selected to retrieve the articles in the database search terms. A different set of keyword search criteria was used for different forms of efficient searching on web pages. In total, 142 records were identified across the included databases (Cochrane Library: 13; Ovid: 4; PubMed: 34; ScienceDirect: 15; Scopus: 87). After sequential screening of titles/abstracts (n = 38) and full texts (n = 21), 11 studies remained eligible for inclusion, as summarized in Table 2.Table 1. Databases used and MeSH strategies.Table 1. DatabaseSearch QueryPubMed(((Fluoride ion OR fluorine compound OR sodium fluoride (NaF) OR stannous fluoride (SnF2) OR monofluorophosphate (MFP) OR fluoride treatment OR fluoridation) AND (bioactive ceramics OR bioglass OR silicate glass OR calcium phosphate glass OR osteoinductive glass OR glass ionomer)) AND (dentifrice OR toothpaste OR fluoride gels)) AND ((dentifrice OR toothpaste OR fluoride gel) AND (caries OR demineralization OR cavity))Ovid(Fluoride ion OR fluoride treatment) AND (caries OR demineralization)ScienceDirect(Fluoride ion OR fluoride treatment) AND (bioactive glass OR remineralization) AND (dentifrice OR toothpaste) AND (caries OR demineralization)Cochrane library(Fluoride ion OR fluoride treatment) AND (bioactive glass OR remineralization) AND (dentifrice OR toothpaste) AND (caries OR demineralization)Scopus(((Fluoride ion OR fluorine compound OR sodium fluoride (NaF) OR stannous fluoride (SnF2) OR monofluorophosphate (MFP) OR fluoride treatment OR fluoridation) AND (bioactive ceramics OR bio glass OR silicate glass OR calcium phosphate glass OR osteoinductive glass OR glass ionomer)) AND (dentifrice OR toothpaste OR fluoride gel)) AND ((dentifrice OR toothpaste OR fluoride gel) AND (caries OR demineralization OR cavity))Table 2. Database search and screening summary.Table 2. Step/DatabaseNumber of ReferencesTotal references retrieved142Cochrane library13Ovid4PubMed34ScienceDirect15Scopus87Duplicates removed0Title and abstract screened38Full-text screened21Studies excluded10Studies included11
Only articles published by December 31, 2024, were included, with no search limitations. The articles were stored using EndNote (Clarivate Analytics, EndNote 20, 2021). After removing duplicates, initial article screening was performed based on titles and abstracts. Full texts of screened articles were retrieved and then screened according to PRISMA guidelines.31 Full-text screened articles were also searched manually for references to include eligible studies.
The process based on selecting, screening, including, and excluding studies is depicted in the PRISMA 2020 flowchart (Figure 2).31Figure 2. Systematic review process based on the updated PRISMA 2020 guidelines.Figure 2
Data collection and extracted variables
To ensure unbiased selection, reviewers FTZ and MA independently screened the titles and abstracts against the inclusion criteria. Any disagreements were resolved by a third referee (MK). To ensure eligibility, the full texts of short-listed studies was retrieved and critically assessed before final inclusion in the review process.
Assessment of risk of bias in studies included
The data from selected studies were extracted using a customized Excel spreadsheet. Two independent reviewers (FTZ and MA) assessed the risk of bias and the level of evidence in the selected studies using the modified Consolidated Standards of Reporting Trials (CONSORT) checklist32 for reporting in vitro studies of dental materials. Studies that were excluded based on the inclusion criteria are listed in Table 3.Table 3. Studies not eligible for systematic review.Table 3. Source Author and YearCountryStudy Aims and RationaleReason for IneligibilityChristoffersen, Christoffersen23Denmark, NetherlandsInvestigated the effect of fluoride ions on remineralization of demineralized enamelNot focused on dental cariesChung, millett24UKStudied fluoride release and cariostatic ability of orthodontic bonding materialsFocus on orthodontic bonding not general dental cariesDe Queiroz, Nouer26BrazilIn vivo evaluation of effect of fluoride dentifrice on demineralization/remineralization at the bracket/enamel interfaceOrthodontic study not focused on general dental cariesEggert and Neubert25GermanyIn vitro investigation of fluoride ion release from toothpaste compoundsFocus on fluoride toothpaste rather than dental caries managementMilly, festy27UKExamined bioactive glass in white spot lesion remineralizationStudy on white spot lesions rather than general dental cariesQiu, Lu28ChinaEvaluated a novel bioactive glass–ceramic for dental applicationsFocus on bioactive glass development rather than dental caries treatmentDegli Esposti, Zheng29–Investigated composite materials made of amorphous calcium phosphate and bioactive glass nanoparticles for preventive dentistryNot directly related to dental caries treatmentChung, millett24UKAnalyzed fluoride uptake and release in orthodontic materialsFocus on orthodontics not general caries managementEggert and Neubert25GermanyInvestigated fluoride ion release in a permeation modelNot focused on dental caries treatmentQiu, Lu28ChinaEvaluated remineralization potential of novel bioactive glass materialsNot specific to dental caries treatmentTable 4CONSORT-based quality assessment of in vitro studies.Table 4. Study (Author, Year)Title & AbstractIntroductionObjectivesSample Size JustificationRandomization & BlindingOutcome Measures & Statistical AnalysisOverall QualityBakry, abbassy11YesYesYesNoNoANOVA, microhardness, SEMModerateDai, mei12YesYesYesNoNoMicro-Computed Tomography (CT), mineral analysis, ANOVAModeratede moura, de melo simplício34YesYesYesNoNoMicrohardness, SEM, ANOVAModerateParkinson, siddiqi16YesYesYesNoNoSurface hardness, TMR, ANOVAModerateSuryani, Gehlot14YesYesYesNoNoMicrohardness, SEM, ANOVAModerateWang, mei8YesYesYesNoNoKnoop hardness, SEM, Tukey's testModerateAli, farooq21YesYesYesNoNoVickers hardness, statistical analysis reportedModerateDai, mei12YesYesYesNoNoMicro-CT, lesion depth analysisModerateKhamverdi, farmani15YesYesYesNoNoMicrohardness, SEM, ANOVAModerateSuryani, Gehlot14YesYesYesNoNoVickers hardness, SEM, ANOVAModerateAras, Celenk33YesYesYesNoNoMicrohardness, SEM, ANOVAModerateCT, Computed Tomography.
These studies were excluded based on the predefined criteria, including language, type of study, lack of focus on dental caries, and non-human studies.
Results
Key features of studies included
The initial search yielded a total of 142 papers from electronic databases. Using EndNote 20 software, the studies were then screened (titles and abstracts) to obtain a total of 38 studies. Full texts were retrieved for 21 of these studies for detailed analysis of eligibility for inclusion in the systematic review, and one study was not included because the full text could not be retrieved. Subsequently, 10 studies were excluded for various reasons, and 11 studies were included in the final analysis. The general characteristics of studies included in the systematic review are shown in Table 5, and the data from previous studies and significant findings are listed in Table 6. Heterogeneity among the studies included in the review prevented meta-analysis.Table 5. General characteristics of studies included.Table 5. Author and YearCountryStudy DesignRemineralization Measurement DeviceTime pointsAhmed samir bakry et al. (2020)Not specifiedIn vitroSEM, EDS, TMR, microhardness testing4 daysLin Lu Dai et al. (2022)ChinaIn vitroMicro-CT, mineral loss analysis4 daysMarcoeli silva de moura et al. (2019)BrazilIn vivoMicrohardness testing, SEM28 daysParkinson et al. (2017)USAIn situSurface microhardness, TMR, SEM28 daysSuryani et al. (2021)IndiaEx vivoVickers microhardness, SEM15 cyclesYu Wang et al. (2016)China, New ZealandIn vitroKnoop microhardness, SEM, AFM15 daysS. Ali et al. (2019)Not specifiedIn vitroVickers microhardness testing24 hDai LL et al. (2022)ChinaIn vitroMicro-CT, lesion depth analysisNot specifiedZahra Khamverdi et al. (2023)IranIn vitroMicrohardness testing, SEM14 daysParas mull Gehlot et al. (2021)IndiaEx vivoVickers microhardness, SEM28 daysAras et al. (2019)Not specifiedIn vitroSEM, microhardness testingNot specifiedTable 6Summary of results from studies included.Table 6. Study (Author, Year)Sample TypeSubstrateCaries TypeMeasured Outcomes & EquipmentReported FindingsBakry, abbassy11In vitroEnamelWhite spot lesionsTMR, SEM, EDS, microhardnessBiominF® paste reduced mineral lossDai, mei12In vitroDentineArtificial lesionsMicro-CT, mineral loss analysisStrontium-doped bioactive glass improved mineralizationde moura, de melo simplício34In vivoEnamelOrthodontic lesionsMicrohardness, SEMFluoridated dentifrice was most effectiveParkinson, siddiqi16In situEnamelArtificial lesionsSurface microhardness, TMR, SEMCSPS did not enhance effect of fluorideSuryani, Gehlot14Ex vivoEnamelErosion lesionsVickers microhardness, SEMbioactive glass (BAG) and CPP-ACPF obtained highest remineralizationWang, mei8In vitroEnamelEarly caries lesionsKnoop hardness, SEM, atomic force microscopy (AFM)NovaMin and Pro-Relief were highly effectiveAli, farooq21In vitroEnamelArtificial lesionsVickers microhardnessBiominF® was more effective than Novamin®Dai, mei12In vitroDentineRoot cariesMicro-CT, lesion depth analysisStrontium-doped bioactive glass reduced lesion depthKhamverdi, farmani15In vitroEnamelArtificial lesionsMicrohardness, SEMNano-bioactive glass improved remineralizationSuryani, Gehlot14Ex vivoEnamelErosion lesionsVickers microhardness, SEMBAG and CPP-ACPF were most effectiveAras, Celenk33In vitroEnamelArtificial lesionsSEM, microhardness testingBAG exhibited significant remineralization potentialAFM, atomic force microscopy; BAG, bioactive glass.
Assessment of potential bias in selected studies
According to the modified CONSORT checklist (Table 4), the 11 studies included were characterized by moderate quality with a low risk of bias, clear objectives, appropriate methodologies, and valid statistical analyses. However, none of the studies incorporated randomization, blinding, or sample size justification, which are critical for minimizing bias. The modified CONSORT checklist (Table 4) highlights these methodological strengths and limitations, emphasizing the need for standardized research protocols in in-vitro remineralization studies.30
Summary of results
Overview of studies included
In the following, the findings are synthesized from the 11 studies included in the systematic review with respect to the substrate type, caries nature, measured outcomes, specimen dimensions, group size, and grouping of intervention or restoration. The effectiveness of fluoride-based bioactive glass dentifrice at preventing dentine caries was the same across all of these factors.
Sample type and substrate
Most of the studies utilized human enamel and dentine specimens, although some employed bovine enamel models due to their similar structure to human teeth.8 Human enamel is considered the gold standard for remineralization research, but bovine models are often used as they are readily available and provide greater standardization. However, differences in mineral density and permeability between human and bovine enamel may influence remineralization outcomes, and thus limit the translation of in vitro findings into clinical practice.12
Caries type and specimen dimension
The studies investigated various carious models, including white spot lesions, artificially demineralized enamel, and dentine caries. The dimensions of specimens varied across studies, and some used sectioned premolars or molars.10^,^15 The use of an artificial caries model allows controlled lesion formation, mimicking early-stage demineralization. However, variations in lesion depth, demineralization time, and acid exposure protocols across studies introduced inconsistencies that may have affected comparability.14
Sample size and grouping
A major limitation across studies was the lack of sample size justification and none provided prior power calculations, raising concerns regarding statistical robustness. The studies employed sample sizes that ranged between n = 15–40 per group, divided into treatment and control groups. These groupings enabled comparative analysis but the absence of a predefined sample size calculation weakened the reliability of the reported results, and may have led to underpowered or overestimated estimates. Future studies should incorporate sample size estimation based on statistical power analyses to strengthen the quality of the evidence obtained.
Intervention and control groups
Bioactive glass-containing dentifrices were tested in six studies11^,^12^,^14, 15, 16^,^33 and fluoride-based pastes in five studies.12^,^15^,^16^,^21^,^34 These studies either used fluoride dentifrices as an intervention or control group to compare with bioactive glass and CPP-ACP formulations. In three studies,8^,^14^,^34 CPP-ACP formulations were tested as remineralizing agents. Studies that compared fluoride-only treatments with bioactive glass formulations consistently reported superior remineralization outcomes in bioactive glass groups.12^,^14 However, differences in treatment application protocols (e.g., frequency and duration of exposure) may have influenced the outcomes. The control groups varied across studies, including untreated enamel, placebo treatment, or fluoride-only interventions, making direct comparisons challenging.15
Measured outcomes and equipment used
Standardized techniques were employed to assess remineralization effects, such as surface microhardness tests (three used Vickers14^,^15^,^21 and one Knoop8), transverse microradiography (TMR) in two studies,11^,^16 scanning electron microscopy (SEM) in four studies,11^,^14^,^15^,^34 and energy dispersive X-ray spectroscopy (EDS) in two studies.11 Almost all studies (81.8 %) employed microhardness for mineral recovery testing, and SEM, TMR, and microhardness testing were used to observe structural and morphological changes.16 These techniques provide reliable enamel assessments, but discrepancies or errors in testing parameters and measurement intervals across studies may have introduced methodological inconsistencies.14
Reported findings and comparative assessment
All studies with bioactive glass-containing dentifrices reported better remineralization effects than those with fluoride-only formulations. In particular, two studies11^,^12 found that bioactive glass-containing dentifrices enhanced remineralization more effectively than dentifrices with fluoride-only formulations, and they also resulted in greater mineral deposition, lesion depth reduction, and hydroxyapatite formation. These findings were further supported in two other studies14^,^15 that demonstrated increases in enamel hardness recovery and enhanced surface integrity with bioactive glass. These findings suggest that bioactive glass is a better method for repairing early tooth damage. The CPP-ACP formulation obtained a strong remineralization effect, reinforcing its use as an auxiliary treatment to fluoride therapy.8
Discussion
According to this systematic review, bioactive glass-containing dentifrices are preferable for promoting enamel and dentine remineralization, and studies support their potential use in non-invasive caries management. Most studies found that bioactive glass formulations doped with fluoride or strontium significantly increased mineral deposition and reduced the lesion depth compared with conventional fluoride-only treatments.8^,^12 Furthermore, bioactive glass increased calcium and phosphate ion concentrations, as well as fluoride, to provide a more dynamic remineralization process, with enhanced enamel repair and tubular occlusion.11 These findings are consistent with the growing consensus that a greater capacity for protection against dentine caries can be achieved through using multifunctional mineralization agents rather than fluoride alone.
However, although the findings are promising, definitive therapeutic conclusions cannot be drawn because of the very different methodologies employed in individual studies. Restrictions that hinder the direct comparison of results include variations in pH cycling models, lesion induction protocols, treatment application frequencies, and control groups.14^,^15 In addition, differences in specimen types, such as human versus bovine enamel, may have influenced remineralization outcomes due to differences in the composition and permeability of minerals.16 These differences highlight the importance of utilizing a standardized protocol for in vitro remineralization research to reduce the likelihood of unreliable or noncomparable findings.
The review identified a key limitation due to the lack of randomization, blinding, and sample size justification across all studies. Prior power calculations were not provided or described in any of the studies, which is a concern that may affect the statistical robustness of their findings.21 Specimen allocation to random samples and blinded outcome assessment prevents avoidable biases in the choice and assessment of outcomes that could lead to overestimation of the effectiveness of demineralizing agents.14 Future in vitro studies will yield better results by incorporating these methodological safeguards.
Microhardness testing (Vickers and Knoop), SEM, TMR, and EDS were consistently used to evaluate mineral recovery and structural integrity.8^,^12 These techniques provide quantitative and qualitative assessments of remineralization, and thus a better understanding of enamel and dentine repair mechanisms. Unfortunately, differences in measurement intervals and evaluation criteria made comparisons among studies difficult. Therefore, it is necessary to standardize assessment methodologies, including uniform lesion preparation, remineralization exposure times, and post-treatment evaluation criteria, to enhance the reproducibility and clinical clarity of in vitro findings.14
The findings considered in this review support the use of bioactive remineralization agents to advance caries prevention and non-invasive dental treatments. Despite strong in vitro evidence supporting the efficacy of bioactive glass and CPP-ACP formulations, their clinical application remains unclear due to the limitations discussed above. Further investigation is also needed because no significant difference was reported between bioactive glass and fluoride.16 Future research should focus on real-world settings through high-quality in situ and randomized controlled trials with standardized methodologies to allow their validation.15 Addressing the current methodological gaps can allow bioactive remineralization research to provide strong evidence to support the development of effective, evidence-based preventive strategies for dentine caries management.
Conclusion
This review indicates the effectiveness of bioactive glass dentifrice, CPP-ACP, and fluoride formulations in promoting dentine remineralization, with significant improvements in mineral deposition, surface microhardness, and lesion depth reduction, emphasizing the potential use of these agents in non-invasive caries management. All studies demonstrated remineralization potential, but future research should incorporate randomization and blinding to further improve the reliability of the findings. Overall, this systematic review provides strong evidence that bioactive remineralization agents exhibit encouraging performance in vitro, but their translation into evidence-based dental applications requires stronger methodologies and validation through high-quality in situ and clinical trials.
Ethical approval
Not applicable.
Author contributions
Conceptualization: FTZ. Data Curation: FTZ. Investigation: FTZ and MA. Writing-Original Draft: FTZ and MA. Writing, Review, and Editing: FTZ, MA, MSZ. Approval of final Manuscript: all authors. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Data availability statement
Not applicable.
Source of funding
This study was not supported by any sponsor or funder.
Conflict of interest
All authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fejerskov O.Nyvad B.Kidd E.Dental caries: the disease and its clinical management 2015 Wiley
- 2Freitas S.A.A.Oliveira N.M.A.de Geus J.L.Souza S.F.C.Pereira A.F.V.Bauer J.Bioactive toothpastes in dentin hypersensitivity treatment: a systematic review Saudi Dent J 33720213954033480327910.1016/j.sdentj.2021.04.004PMC 8589619 · doi ↗ · pubmed ↗
- 3Al Buraiki M.J.Ingle N.A.Baseer M.A.Al Mugeiren O.M.Minervini G.Long term remineralizing effect of casein phosphopeptide amorphous calcium phosphate in white spot lesions: a systematic review and meta-analysis Technol Health Care 3232024123912543759955010.3233/THC-230722 · doi ↗ · pubmed ↗
- 4Manton D.Diagnosis of the early carious lesion Aust Dent J 58s 1201335392372133610.1111/adj.12048 · doi ↗ · pubmed ↗
- 5ten Cate J.M.Buijs M.J.Miller C.C.Exterkate R.A.Elevated fluoride products enhance remineralization of advanced enamel lesions J Dent Res 871020089439471880974810.1177/154405910808701019 · doi ↗ · pubmed ↗
- 6Srinivasan N.Kavitha M.Loganathan S.C.Comparison of the remineralization potential of CPP-ACP and CPP-ACP with 900 ppm fluoride on eroded human enamel: an in situ study Arch Oral Biol 55720105415442059355510.1016/j.archoralbio.2010.05.002 · doi ↗ · pubmed ↗
- 7Pitts N.B.Zero D.T.Marsh P.D.Ekstrand K.Weintraub J.A.Ramos-Gomez F.Dental caries Nat Rev Dis Primers 32017170302854093710.1038/nrdp.2017.30 · doi ↗ · pubmed ↗
- 8Wang Y.Mei L.Gong L.Li J.He S.Ji Y.Remineralization of early enamel caries lesions using different bioactive elements containing toothpastes: an in vitro study Technol Health Care 24520167017112723309110.3233/THC-161221 · doi ↗ · pubmed ↗