Iron Supplementation with Ferrous Sulfate or Ferrous Bisglycinate for 12 Weeks Does Not Influence Group B Streptococcus Colonization in Cambodian Women: A Secondary Analysis of a Randomized Controlled Trial
Elisa Cirigliano, Annie Saint, Lulu X Pei, Catherine WY Wong, Siyun Wang, Jordie AJ Fischer, Hou Kroeun, Crystal D Karakochuk

TL;DR
A study in Cambodia found that iron supplements did not increase Group B Streptococcus colonization in women, but regional differences suggest local factors may influence infection risk.
Contribution
The study provides new evidence that iron supplementation does not increase GBS colonization in iron-replete women, while highlighting geographic variation in colonization risk.
Findings
Iron supplementation with ferrous sulfate or ferrous bisglycinate did not increase GBS colonization in Cambodian women.
Regional differences in GBS colonization were observed, with lower expression in one district compared to others.
Environmental or behavioral factors may influence GBS colonization risk in the study population.
Abstract
Iron deficiency in women of reproductive age can have severe adverse perinatal consequences. Although iron supplementation can be effective at treating iron deficiency, excess unabsorbed iron in the gut may also promote colonization by enteropathogens such as Group B Streptococcus (GBS), increasing the potential risk of maternal and neonatal infection. We examined whether 12 wk of supplementation with 18 mg elemental iron as ferrous bisglycinate, 60 mg as ferrous sulfate, or a placebo differentially influences GBS colonization in Cambodian women of reproductive age. This study is a secondary analysis of a randomized controlled trial conducted in 25 villages in 3 districts of Kampong Thom province, Cambodia, including 144 nonpregnant women (18‒45 y) who received 18 mg of elemental iron as ferrous bisglycinate, 60 mg ferrous sulfate, or placebo for 12 wk. GBS colonization was assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
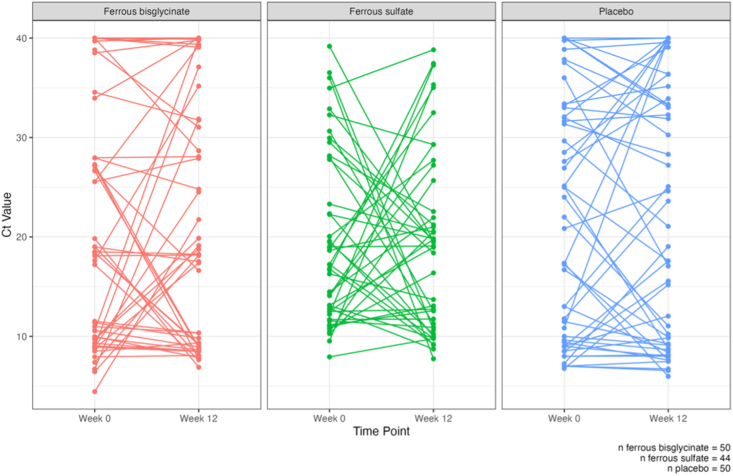 Figure 1
Figure 1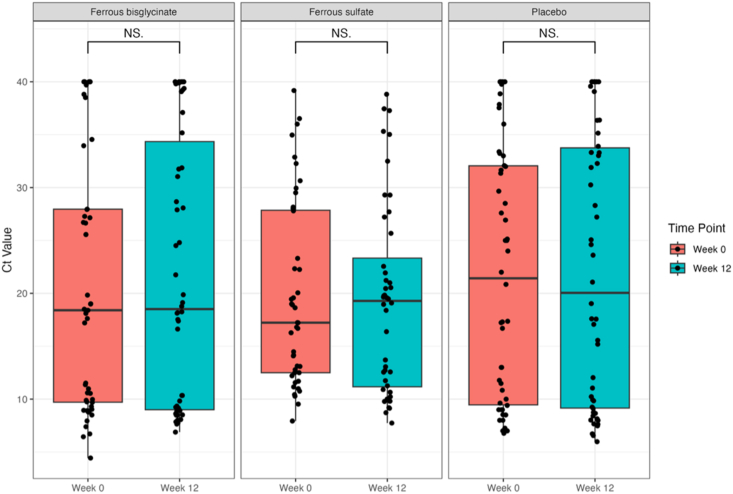 Figure 2
Figure 2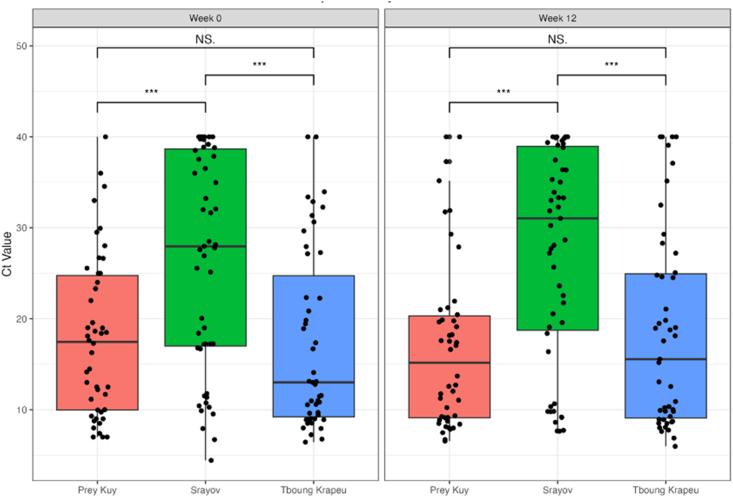 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Streptococcal Infections and Treatments · Sepsis Diagnosis and Treatment
Introduction
Adequate iron status is important for nonpregnant women of reproductive age who may soon become pregnant, because iron deficiency (ID) in the perinatal period can increase risk of adverse maternal and fetal outcomes, such as postpartum hemorrhage, low birthweight or small for gestational age infants, and stillbirth [1,2]. As such, the World Health Organization (WHO) global guidelines recommend daily oral iron supplementation with 30‒60 mg elemental iron for 12 wk for women and adolescents in regions where anemia prevalence is >40% [3]. Supplemental iron may be beneficial for individuals with ID anemia; however, for those with anemia due to other causes [e.g., hemoglobin (Hb) disorders, inflammation, malarial infection, and/or parasitic infections] [4], additional iron may be harmful.
Evidence has shown that excess unabsorbed iron plays an important role in the virulence and colonization of enteropathogens, such as Escherichia coli and Streptococcus agalactiae, in the human gut [5,6]. S. agalactiae, otherwise known as Group B Streptococcus (GBS), is an enteropathogen of concern because it is an opportunistic bacterial pathogen that colonizes the genital and gastrointestinal tracts of many adults and can develop into an invasive disease [7,8]. GBS colonization during pregnancy is a major concern and can lead to complications during or after labor for both the mother and the infant, including amniotic infection, sepsis, meningitis, and death [7,8]. For nonpregnant women, invasive GBS also has several clinical manifestations, including bacteremia, sepsis, pneumonia, soft-tissue infections, and urinary tract infections [[7], [8], [9], [10]]. In many developed countries, such as Canada and the United States, routine GBS screening is performed on pregnant women at 35‒37 weeks of gestation to assess the risk of perinatal GBS transmission [11]. However, in developing countries such as Cambodia, there is currently no policy to screen or treat pregnant women for GBS, and the prevalence of GBS in Cambodian women is largely unknown.
To explore if iron supplementation influences GBS colonization in Cambodian women, we examined the effects of oral iron supplements compared with placebo, specifically whether the form of iron in the supplement (ferrous sulfate compared with ferrous bisglycinate) differentially influences GBS colonization. We conducted real-time qPCR (RT-qPCR) on DNA extracted from stool specimens of Cambodian women to identify the target gene cfb, which encodes for the Christie-Atkins-Munch-Peterson (CAMP) factor in GBS [12], as an indicator of GBS colonization. We hypothesized that women who received the iron interventions would have a higher relative increase in cfb expression after 12 wk than women who received a placebo.
Methods
Study design, study population, and ethical approval
This study was a secondary analysis of a randomized controlled trial of oral iron supplementation in Cambodian women of reproductive age that included 480 women from rural Kampong Thom province [13]. The aims of the original trial were to assess mean ferritin concentrations and other biomarkers after 12 wk of daily oral iron supplementation of 18 mg elemental iron as ferrous bisglycinate, 60 mg ferrous sulfate, or placebo. Key findings of the trial have been published [13]. Ethical approval for the trial was obtained from The University of British Columbia Clinical Research Ethics Board (H18-02610) and the National Ethics Committee for Health Research in Cambodia (273-NECHR). The trial was registered at clinicaltrials.gov (NCT04017598) on 10 July, 2019 and the study protocol has been published [14].
The study population included healthy, nonpregnant women of reproductive age (18‒45 y) living in Kampong Thom, Cambodia, from 25 villages within the 3 districts of Prey Kuy, Srayov, and Tboung Krapeu. Recruitment began in December 2019, baseline visits started in January 2020, and the trial was completed in May 2020. Participants provided written informed consent, and blood and stool specimens were collected at the beginning and end of the 12-wk trial period. Women were excluded if they had consumed antibiotics, dietary supplements, vitamin or mineral supplements, or nonsteroidal anti-inflammatory drugs in the 12 wk prior to the trial. Enrolled participants were randomly assigned at each health center in a 1:1:1 ratio to receive ferrous bisglycinate, ferrous sulfate, or placebo (n = 160 for each trial arm) by a computer-generated list of random numbers prepared by the study coordinator (who did not have access to the random allocation sequence).
The trial supplements were produced by Natural Factors (Coquitlam, Canada). The ferrous bisglycinate capsule contained 18 mg elemental iron (experimental treatment), the ferrous sulfate capsule contained 60 mg elemental iron (standard treatment), and the placebo capsule contained microcrystalline cellulose (no elemental iron). All capsules and packaging were identical in size, shape, and color. Natural Factors was responsible for blinding and did not unveil intervention group codes to the statistical analysis team until the analysis for the primary outcome (ferritin concentrations) was completed.
Local research staff in Cambodia conducted regular home visits to monitor adherence to daily supplementation and to record any reported side effects. Trial investigators, research staff, and participants were blinded to the interventions, and the intervention group allocation codes were not unveiled to the research team until the primary outcome analysis was completed.
Sample collection and processing
Fasting venous blood specimens were collected from participants in the morning on day 1 and again after 12 wk of the intervention. Samples were collected in a 6-mL trace element-free tube, a 6-mL evacuated tube containing EDTA, and a 2-mL tube containing EDTA (Becton Dickinson). A complete blood count was performed using an automated hematology analyzer (Sysmex XN-1000; Sysmex Corporation) to measure Hb (grams per liter) and other hematologic indicators.
Women used an at-home collection kit [15] to obtain a neat stool specimen in their homes, which was transported to the local health center for pick up by the research staff. Neat stool and blood specimens were stored at ‒20°C until shipment on dry ice to The University of British Columbia (Vancouver, Canada), where they were stored at ‒80°C until analysis. Ferritin, α-1-acid glycoprotein, and C-reactive protein were measured using a sandwich-ELISA in Germany [16]. Ferritin was corrected for inflammation using α-1-acid glycoprotein and C-reactive protein concentrations as per globally-endorsed Biomarkers Reflecting the Inflammation and Nutritional Determinants of Anemia guidelines [17].
RT-qPCR detection of the cfb target gene
For the current study, a subset of stool specimens (n = 144) was randomly selected from each of the 3 arms using a computer-generated list (n = 50 ferrous bisglycinate, n = 44 ferrous sulfate, and n = 50 placebo). Only n = 44 specimens in the ferrous sulfate group were included due to missing baseline or endline matched pairs. DNA was extracted from stool specimens using the QIAamp PowerFecal Pro DNA kit (Qiagen) according to the manufacturer’s instructions. DNA purity was assessed using a nanodrop spectrophotometer (NanoDrop Technologies Inc.). RT-qPCR was performed on DNA extracted from stool specimens to identify the target gene, cfb, which encodes for the CAMP factor in GBS [12], as an indicator of GBS colonization. The target gene was amplified from extracted DNA using SsoAdvanced Universal SYBR Green Supermix (Bio-Rad Laboratories Inc.), with primers obtained from Integrated DNA Technologies Inc. (5’-TGGTAGTCGTGTAGAAGCCTTA-3’). To standardize input across reactions, an equal volume of DNA extract was added to each RT-qPCR well, keeping reaction composition constant across specimens. Because DNA concentration varied between stool extracts, the input mass of DNA was not normalized across samples, and results are presented as cycle threshold (Ct) values. All procedures were performed at The University of British Columbia (Vancouver, Canada) following the manufacturer’s instructions.
A 7-point standard curve (10-fold dilutions) was analyzed on each plate to confirm assay linearity and efficiency and to ensure between-plate comparability. Although the standard curve function was applied to Ct values for quality control (QC) purposes, Ct was not converted to absolute copies because 1) stool extraction yields varied and were not normalized to a fixed stool mass, and 2) aliquot volumes of DNA, not DNA mass, were used for each reaction. The Ct values indicate the number of cycles needed to replicate enough DNA to be detected [18,19]. The quantity of DNA in the sample is inversely correlated with the Ct value; the higher the quantity of target DNA present in the sample, the lower the Ct value will be [18,19].
Statistical analyses
The cutoff for cfb expression was established in 35 cycles; therefore, specimens with a Ct value <35 were deemed positive for cfb expression [19]. Specimens where cfb expression was not detected at all were given a Ct value of 40, which is above the threshold for cfb detection. This approach was chosen to retain all samples in the analysis, although assigning a fixed Ct value to undetected samples can contribute to a multi-modal distribution. Therefore, median IQR Ct values were reported, and nonparametric statistical tests (Kruskal-Wallis and Wilcoxon signed-ranked tests) were used to compare cfb expression across and within groups below. Kruskal-Wallis tests were used to compare cfb expression (Ct values) across the 3 treatment arms and between the 3 health center districts at week 0 and week 12 timepoints, with a post hoc Dunn test to determine which groups were significantly different (P < 0.01). Paired Wilcoxon signed-rank tests were used to compare differences between week 0 and week 12 within each treatment arm.
Results
Participant characteristics
Baseline characteristics of the enrolled cohort by trial arm are reported in Table 1. Women had a mean ± SD age of 34 ± 7 y, a BMI (kg/m^2^) of 23.6 ± 3.7, and a median [IQR] number of children of 2 [1, 3]. Information about the health status of the participants is detailed in Table 2 [16]. At baseline, the prevalence of anemia (Hb <120 g/L) was 17% (n = 25/144), ID based on inflammation-adjusted ferritin <15 μg/L was 6% (n = 9/144), and ID anemia based on inflammation-adjusted ferritin <15 μg/L and Hb <120 g/L was 3% (n = 5/144). Overall, 62% of women (n = 90/144) were highly adherent to the supplement regime, defined as consuming 80% or >67 of the 84 prescribed capsules over the 12 wk. Following 12 wk of supplementation, median [IQR] ferritin concentration was 89.4 [61.0, 121.0] μg/L in the ferrous sulfate group, 89.4 [49.2, 120.6] μg/L in the ferrous bisglycinate group, and 85.5 [42.8, 111.8] μg/L in the placebo group, with an ID prevalence of 0%, 0%, and 6% (n = 3/50) in each group respectively.TABLE 1Baseline characteristics of the enrolled Cambodian women by treatment arm.TABLE 118 mg Ferrous bisglycinate (n = 50)60 mg Ferrous sulfate (n = 44)Placebo (n = 50)Age, y33.2 ± 7.235.0 ± 6.634.1 ± 7.9BMI (kg/m^2^)22.6 ± 3.623.6 ± 3.524.5 ± 3.8Parity2 [2, 3]2 [1, 3]2 [1, 3]Household size4.8 ± 1.44.3 ± 1.24.4 ± 1.1Health center, % Prey Kuy, n = 4616/46 (35)14/46 (30)16/46 (35) Srayov, n = 5117/51 (33)17/51 (33)17/51 (33) Tboung Krapeu, n = 4717/47 (36)13/47 (28)17/47 (36)Flush to the septic tank household toilet, %46 (92)40 (91)46 (92)Water source, % Hand pump30 (60)29 (66)29 (58) Ringwell12 (24)8 (18)11 (22) Pond/river7 (14)3 (7)5 (10) Bottled water1 (2)4 (9)4 (8) Other0 (0)0 (0)1 (2)Animal(s) living in the home, %46 (92)37 (84)45 (90)Animal(s) living outside the home, %28 (56)24 (55)27 (54)Values are n (%), mean ± SD, or median [IQR].Abbreviations: BMI, body mass index; IQR, interquartile range; SD, standard deviation.TABLE 2Health status of enrolled Cambodian women by treatment arm.TABLE 218 mg Ferrous bisglycinate (n = 50)60 mg Ferrous sulfate (n = 44)Placebo (n = 50)Hemoglobin, g/L130.7 ± 13.1128.4 ± 12.7130.7 ± 11.4 Anemia (Hb <120 g/L), %9 (18)8 (18)8 (16)Serum ferritin,1μg/L62.6 [40.1, 108.3]74.7 [32.6, 105.8]84.7 [52.4, 114.1] Iron deficiency, ferritin <15 μg/L^1^, %3 (6)3 (7)3 (6) Iron deficiency anemia, Hb <120 g/L and ferritin <15 μg/L^1^, %3 (6)1 (2)1 (2)CRP, mg/L0.37 [0.09, 1.77]0.50 [0.09, 1.29]0.50 [0.05, 2.36] >5 mg/L, %4 (8.0)1 (2.3)6 (12.0)AGP, g/L0.60 [0.51, 0.75]0.51 [0.44, 0.69]0.58 [0.47, 0.79] >1 g/L, %6 (12.0)2 (4.6)6 (12.0)Adherence to supplementation2, %28 (56)29 (66)33 (66)Took antibiotics in last year, %20 (40)14 (32)20 (40)Values are n (%), mean ± SD, or median [IQR].Abbreviations: AGP, α-1-acid glycoprotein; CRP, C-reactive protein; Hb, hemoglobin; IQR, interquartile range; SD, standard deviation.1Serum ferritin values were corrected for inflammation [16].2Women were defined as adherent if they consumed ≥80% of the capsules at the week 12 capsule count.
Changes in cfb expression from 0 to 12 wk
Figure 1 shows individual-level changes in cfb expression (Ct values) from week 0 to week 12, across the 3 trial arms (n = 50 ferrous bisglycinate, n = 44 ferrous sulfate, and n = 50 placebo). Median Ct values for the cfb gene were examined for each trial arm between weeks 0 and 12 to determine if the dose and/or form of iron supplementation influences cfb expression (Figure 2). The median Ct values for each trial arm at each time point can be found in Table 3. We found no significant differences in cfb expression between weeks 0 and 12 in any of the trial arms. Similarly, we also found no significant difference in cfb expression between the 3 trial arms at the 12-wk timepoint.FIGURE 1Individual-level change in Ct values (cfb gene expression) from week 0 to 12. Ct, cycle threshold.FIGURE 1FIGURE 2Median [IQR] Ct values (cfb gene expression) at weeks 0 and 12 by treatment arm. Ct, cycle threshold; IQR, interquartile range; NS, non-significant.FIGURE 2TABLE 3Raw cycle threshold values and proportion of individuals with cycle threshold values <35 at each timepoint by treatment arm.TABLE 318 mg Ferrous bisglycinate (n = 50)60 mg Ferrous sulfate (n = 44)Placebo (n = 50)Ct values at 0 wk18.4 [9.7, 27.9]17.22 [12.5, 27.9]21.4 [9.5, 32.1] Ct <35 at 0 wk1, %41 (82)40 (91)41 (82)Ct values at 12 wk18.5 [9.0, 34.3]19.3 [11.2, 23.3]20.0 [9.2, 33.8] Ct <35 at 12 wk1, %37 (74)39 (89)38 (76)Values are n (%) or median [IQR].Abbreviations: Ct, cycle threshold; IQR, interquartile range.1A Ct value <35 indicates that cfb is present in detectable amounts.
Regional differences in cfb expression
To assess for other risk factors that contribute to GBS in Cambodian women, we also compared cfb expression across the 3 districts (Figure 3). Median [IQR] Ct values were 17.5 [10.0, 24.8] at week 0 and 15.2 [9.1, 20.3] at week 12 in Prey Kuy (n = 46); 28.0 [17.0, 38.7] at week 0 and 31.0 [18.7, 38.9] at week 12 in Srayov (n = 51); and 13.0 [9.2, 24.7] at week 0 and 15.6 [9.1, 24.9] at week 12 in Tboung Krapeu (n = 47). Significant differences in Ct values were detected only between Srayov and Prey Kuy, and between Srayov and Tboung Krapeu at both timepoints. At week 0, women from Srayov had significantly higher Ct values (lower cfb expression) than women from Prey Kuy (P = 0.0014) and Tboung Krapeu (P < 0.001). These differences persisted at week 12, with women from Srayov showing lower cfb expression than Prey Kuy (P < 0.001) and Tboung Krapeu (P = 0.001).FIGURE 3Median [IQR] Ct values (cfb gene expression) at weeks 0 and 12 by district. Ct, cycle threshold; IQR, interquartile range; NS, non-significant. ∗∗∗ indicates a statistically signficant difference between the compared groups.FIGURE 3
Discussion
Contrary to our hypothesis, 12 wk of daily iron supplementation did not significantly influence cfb expression in nonpregnant Cambodian women of reproductive age. Furthermore, no differential effect on cfb expression was detected between the 2 forms of iron (ferrous sulfate compared with ferrous bisglycinate), despite differences in the elemental iron dose (ferrous sulfate group receiving 60 mg elemental iron compared with ferrous bisglycinate group receiving 18 mg elemental iron). However, we did observe geographic differences in cfb gene expression: women from the Srayov health district had lower cfb expression than participants from Prey Kuy or Tboung Krapeu at both 0 wk and 12 wk, suggesting that these differences preceded this trial.
There are several environmental risk factors that have been shown to influence GBS colonization and infection. Previous studies have identified that fish consumption, frequency of sexual intercourse, and panty liner use increased the risk of GBS infection in adults [20,21]. However, the limited data we have available does not allow us to discern the causes of the observed regional differences.
It is important to note the very low prevalence of ID among our study population, especially in consideration of the interpretation of our null findings. Iron homeostasis in the body is tightly regulated by hepcidin, a liver peptide, which controls iron concentrations in the blood through degradation of ferroportin in iron-absorptive enterocytes and iron-recycling macrophages [22]. In iron-replete individuals, hepcidin is upregulated and ferroportin is degraded from the walls of the duodenal enterocytes, which limits iron absorption as a protective mechanism [22,23]. In other words, the absorption of the elemental iron from our study supplements may have been largely inhibited, given our study population was predominantly iron-replete. If this were the case, much of the supplemental iron may have remained unabsorbed and passed into the gut, where it has the potential to fuel the growth of enteropathogens, such as GBS. Thus, although our study population was ideal for testing the hypothesis that unabsorbed iron promotes GBS colonization, we still did not observe significant differences. However, it is possible that a longer duration of supplementation or higher elemental iron doses could yield different results.
Notably, >70% of participants in our study had detectable cfb expression (Ct <35) at either baseline or endline, indicating a high prevalence of GBS colonization among healthy, nonpregnant women. This finding has important implications. In many high-income countries, routine screening and intrapartum antibiotic prophylaxis are implemented to prevent vertical transmission of GBS during childbirth. In contrast, no formal screening policies currently exist in Cambodia, and the population-level prevalence of GBS colonization remains poorly characterized. Although our study does not assess active infection or clinical outcomes, the high proportion of cfb-positive individuals highlights the need for further research into GBS transmission dynamics and may support future policy discussions around maternal GBS screening in Cambodia.
We acknowledge some limitations in our study. First, the current gold standard for identifying GBS infection set by the Centers for Disease Control and Prevention is rectovaginal sample incubation in a selective medium broth and subculture on a blood agar plate [11]. We acknowledge the limitations in our methodological approach on the use of stool-based RT-qPCR to target the cfb gene, because this method cannot distinguish between viable colonization and the transient presence of DNA, and may miss some cfb-negative GBS strains. Microbiologic culturing (the clinical gold standard) for GBS would be ideal; however, the feasibility and resources were not available in rural Cambodia to undertake this approach. Several studies have tested the accuracy of RT-qPCR compared with culture techniques to develop a more rapid GBS detection test and have found that RT-qPCR targeting the cfb, sip, atr, and scpB genes has proven successful in identifying positive GBS cases in clinical settings [12,[24], [25], [26], [27]]. The cfb gene codes for the CAMP factor, which is the primary virulence factor in GBS [12]. Carrillo-Ávila et al. [24] (2018) found that GBS detection using RT-qPCR and the cfb target gene alone had a sensitivity of ∼94% and a specificity of ∼95% when compared with cultured samples [24]. However, Zhou et al. [12] (2023) isolated and sequenced GBS strains and found that ∼8% of the strains they isolated were CAMP-negative, concluding that cfb alone cannot be the presumptive test for GBS detection [12]. Second, the presence of cfb expression in a stool sample is not indicative that the individual had an active GBS infection. GBS colonization can be transient, meaning that colonization status changes over time [28]. Compounding with the fact that we only had 2 collection time points during the 12-wk trial, we were unable to capture short-term fluctuations in cfb expression throughout the trial, only the overall change. Despite these limitations, our study has several notable strengths. The use of a randomized controlled trial design with a matched baseline and endline sample for each participant provides a robust framework for assessing longitudinal changes in GBS colonization. The application of RT-qPCR for cfb detection enabled sensitive and high-throughput analysis of samples from a low-resource setting where culture-based diagnostics may not be feasible. Moreover, the use of stool specimens allowed for the noninvasive assessment of intestinal colonization, a key reservoir for GBS, and offered a practical alternative to rectovaginal sampling in this rural population. Although cfb alone may not capture all GBS strains, it remains a widely used and highly specific molecular marker. In the absence of GBS screening programs in Cambodia, our findings provide valuable foundational data on colonization prevalence and geographic variability among women of reproductive age.
In conclusion, to our knowledge, this is the first published study to examine the effect of iron supplementation on GBS colonization in women in Cambodia. In our cohort of predominantly iron-replete nonpregnant women of reproductive age, we did not detect any differences in GBS colonization across the 2 iron interventions, as compared with placebo. However, we observed significant regional differences in cfb expression. Although the estimated prevalence of active GBS infection in women cannot be ascertained from our data, it does raise caution, given the high proportion of individuals with Ct values <35 (indicating the cfb gene is present in detectable amounts). Currently, no policy exists in Cambodia to screen pregnant or nonpregnant women for GBS colonization. These findings provide a foundation for future research into GBS screening and disease risk in Cambodia.
Author contributions
The authors’ responsibilities were as follows– JAJF, HK, CDK: designed the research; JAJF, HK: oversaw specimen collection, transportation and storage; EC, AS, SW: analyzed specimens; EC, LXP, CDK: analyzed data; EC, LXP, CDK: drafted the manuscript; EC, AS, CWYW, SW, JAJF, HK, CDK: contributed to the editing and finalization of the submitted manuscript; CDK: had overall study oversight and primary responsibility for content; and all authors: read and approved the final manuscript.
Data availability
Data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval by the principal investigator.
Funding
This project was funded by the Canadian Institutes of Health Research (CIHR) Project Grant (ID400771).
Conflict of interest
LXP received graduate student scholarships from CIHR and reports a relationship with Balchem Corp that includes: travel reimbursement. JAJF received graduate student scholarships from CIHR. CDK reports a relationship with Balchem Corp that includes: receiving grants. CDK is a Michael Smith Foundation for Health Research Scholar and a CIHR Canada Research Chair in Micronutrients and Human Health. CDK is an editor for The Journal of Nutrition and played no role in the journal’s evaluation of the manuscript. All other authors report no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nair M.Choudhury M.K.Choudhury S.S.Kakoty S.D.Sarma U.C.Webster P.Association between maternal anaemia and pregnancy outcomes: A cohort study in Assam, India BMJ Glob. Health 112016 e 000026
- 2Shi H.Chen L.Wang Y.Sun M.Guo Y.Ma S.Severity of anemia during pregnancy and adverse maternal and fetal outcomes JAMA Netw. Open 522022 e 2147046
- 3World Health Organization Guideline: intermittent iron and folic acid supplementation in menstruating women 2011 World Health Organization Geneva
- 4Chaparro C.M.Suchdev P.S.Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries Ann. N Y Acad. Sci.14501201915313100852010.1111/nyas.14092 PMC 6697587 · doi ↗ · pubmed ↗
- 5Clancy A.Loar J.W.Speziali C.D.Oberg M.Heinrichs D.E.Rubens C.E.Evidence for siderophore-dependent iron acquisition in Group B Streptococcus Mol. Microbiol.5920067077211639046110.1111/j.1365-2958.2005.04974.x · doi ↗ · pubmed ↗
- 6Hantke K.Braun V.The art of keeping low and high iron concentrations in balance Storz G.Hengge-Aronis R.Bacterial stress responses 2000 ASM Press Washington, DC 275288
- 7Raabe V.N.Shane A.L.Group B Streptococcus (Streptococcus agalactiae)Microbiol. Spectr.722019
- 8Schuchat A.Group B Streptococcus Lancet.3539146199951561002396510.1016/S 0140-6736(98)07128-1 · doi ↗ · pubmed ↗