Simple water infusion via a non-traumatic tube facilitates endoscopic resection of an appendiceal-orifice polyp
Hajime Yoshii, Kazunori Takada, Kenichiro Imai, Sayo Ito, Kinichi Hotta, Hiroyuki Ono

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
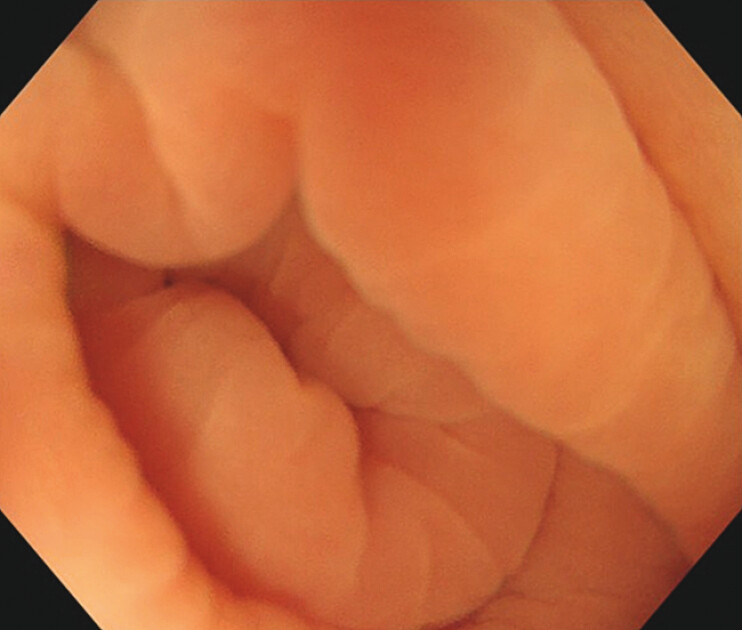 Fig. 1
Fig. 1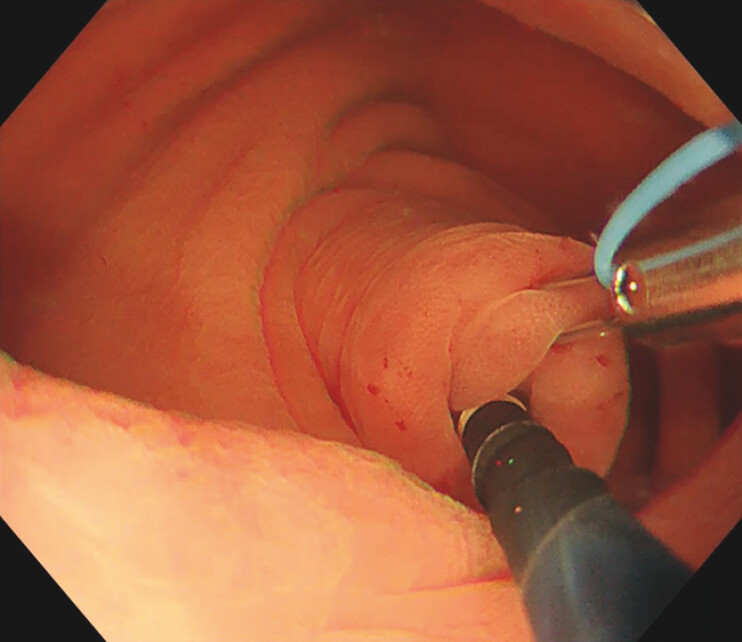 Fig. 2
Fig. 2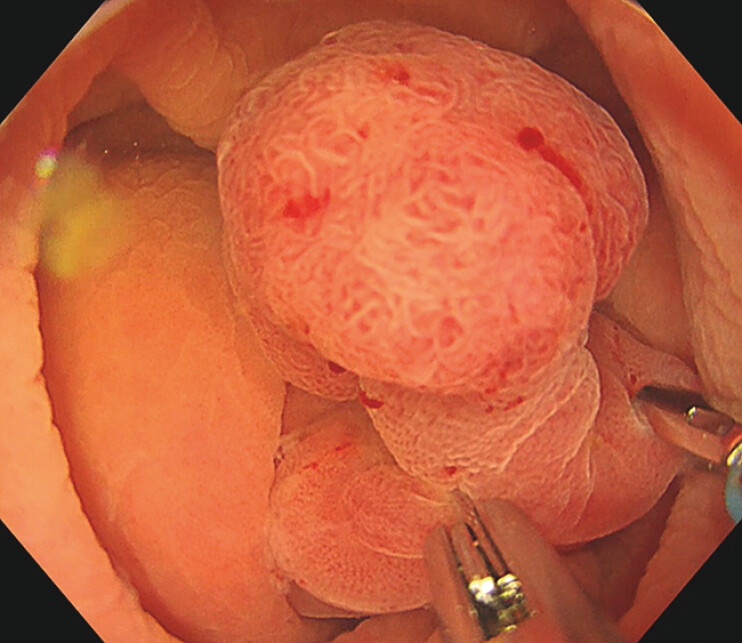 Fig. 3
Fig. 3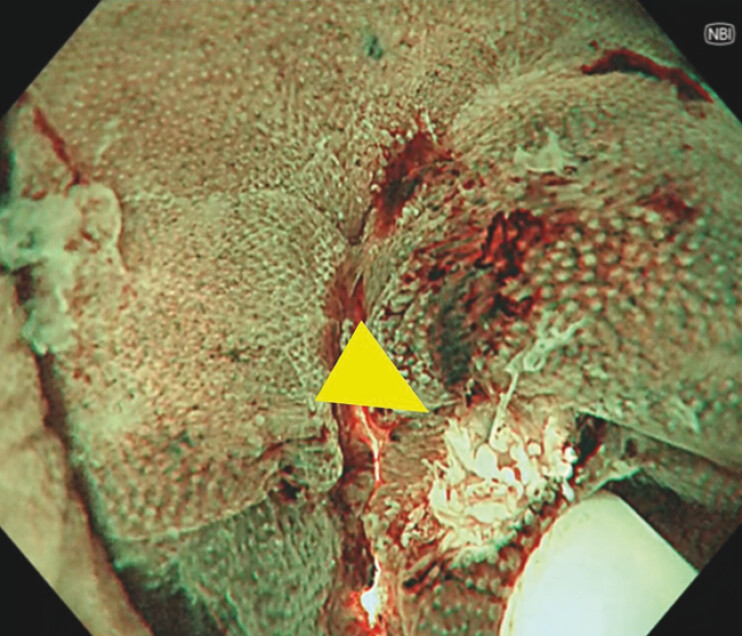 Fig. 4
Fig. 4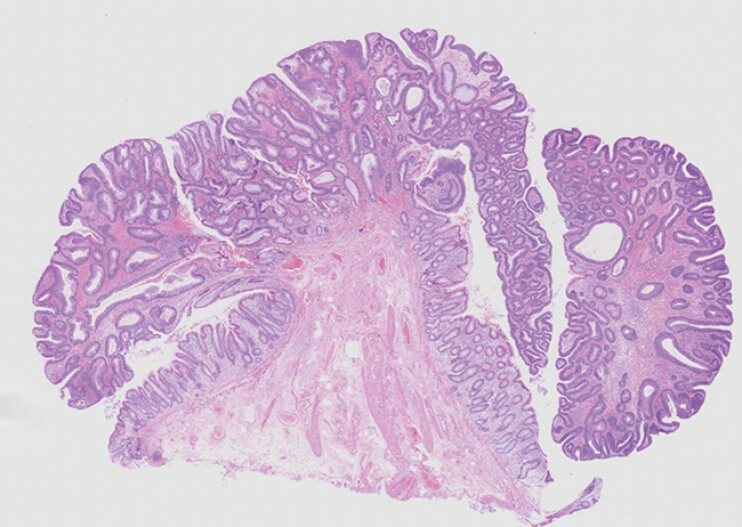 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Minimally Invasive Surgical Techniques · Gastric Cancer Management and Outcomes
We present the case of a 53-year-old man who was referred after fecal immunochemical test-positive colonoscopy revealing a polyp in the appendiceal orifice (AO). In our initial examination, the polyp could not be visualized with air insufflation or water immersion ( Fig. 1 ), even with traction using biopsy forceps. A repeat colonoscopy 3 months later failed to expose the lesion, even with traction using a multi-loop traction device (Boston Scientific Co. Ltd, Tokyo, Japan). Subsequently, a non-traumatic tube was carefully inserted into the appendiceal lumen ( Fig. 2 ). Continuous water infusion through the tube generated hydraulic pressure that extruded the polyp into the cecal lumen, thus permitting stable visualization ( Fig. 3 ). The lesion appeared pedunculated with a 10-mm head. Magnifying narrow band imaging revealed Japan NBI Expert Team classification Type 2A, consistent with adenoma. After placement of a hemostatic clip at the stalk base, en bloc resection was performed using underwater endoscopic mucosal resection. Complete resection was confirmed endoscopically and additional prophylactic clips were applied ( Fig. 4 ). The procedure was completed without any adverse events. Histopathological examination revealed a tubular adenoma with negative margins ( Fig. 5 ).
The lesion could not be visualized with water immersion.
A non-traumatic tube was inserted into the appendiceal lumen.
Continuous water infusion through the tube generated hydraulic pressure that extruded the polyp into the cecal lumen.
Complete resection was confirmed endoscopically. The arrowhead indicates the edge of the resection base.
Histopathology revealed tubular adenoma.
Polyps at the AO often require surgery because of difficulties in visualization and access 1 . To the best of our knowledge, this is the first report of targeted water infusion into the appendix via a non-traumatic tube to expose an AO polyp and enable safe resection using standard tools ( Video 1 ). The safety of appendiceal intubation and irrigation is supported by reports of endoscopic retrograde appendicitis therapy 2 3 . This simple and reproducible maneuver may expand endoscopic options and help avoid surgery for AO polyps.
Simple water infusion via a non-traumatic tube facilitates endoscopic resection of an appendiceal-orifice polyp.Video 1
Endoscopy_UCTN_Code_TTT_1AQ_2AD_3AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kurokawa T Kanemoto Y Azuma Y Endoscopically unobservable appendiceal adenoma treated using laparoscopically assisted surgery: A case report Int J Surg Case Rep 20218310594933975203 10.1016/j.ijscr.2021.105949 PMC 8129934 · doi ↗ · pubmed ↗
- 2Xu Z Jin L Wu W Clinical efficacy and safety of endoscopic retrograde appendicitis treatment for acute appendicitis: A systematic review and meta-analysis Clin Res Hepatol Gastroenterol 20234710224110.1016/j.clinre.2023.10224137925019 · doi ↗ · pubmed ↗
- 3Li Z Chen Y Zhang X Feasibility and effectiveness of endoscopic retrograde appendicitis therapy for uncomplicated acute appendicitis: a systematic review and meta-analysis Surg Endosc 2025394137414510.1007/s 00464-025-11797-z 40369281 · doi ↗ · pubmed ↗