A rare case of hepatic hilar lymphangioma diagnosed using endoscopic and transabdominal ultrasonography
Koichi Soga, Mayumi Yamaguchi, Masaru Kuwada, Ryosaku Shirahashi, Ikuhiro Kobori, Masaya Tamano

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
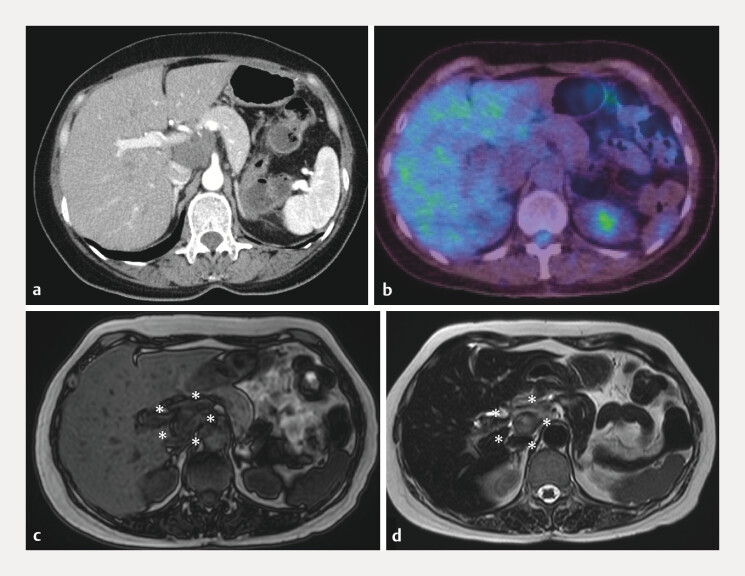 Fig. 1
Fig. 1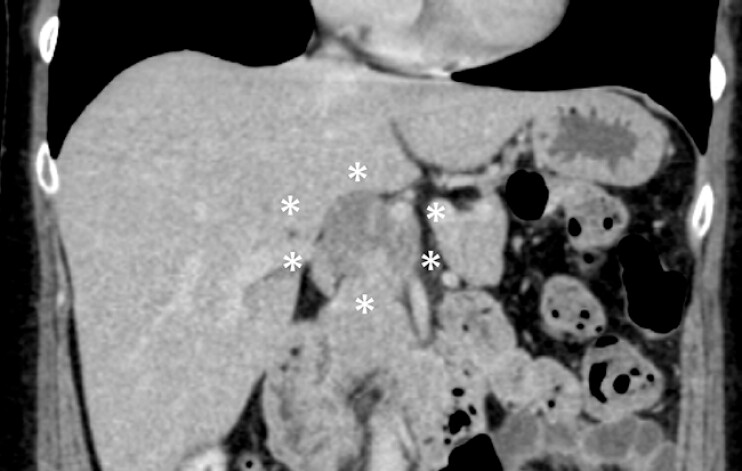 Fig. 2
Fig. 2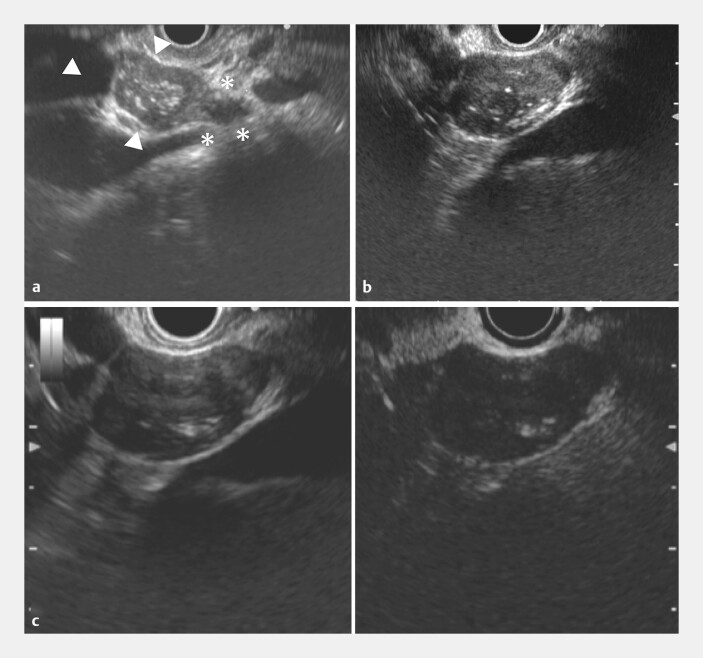 Fig. 3
Fig. 3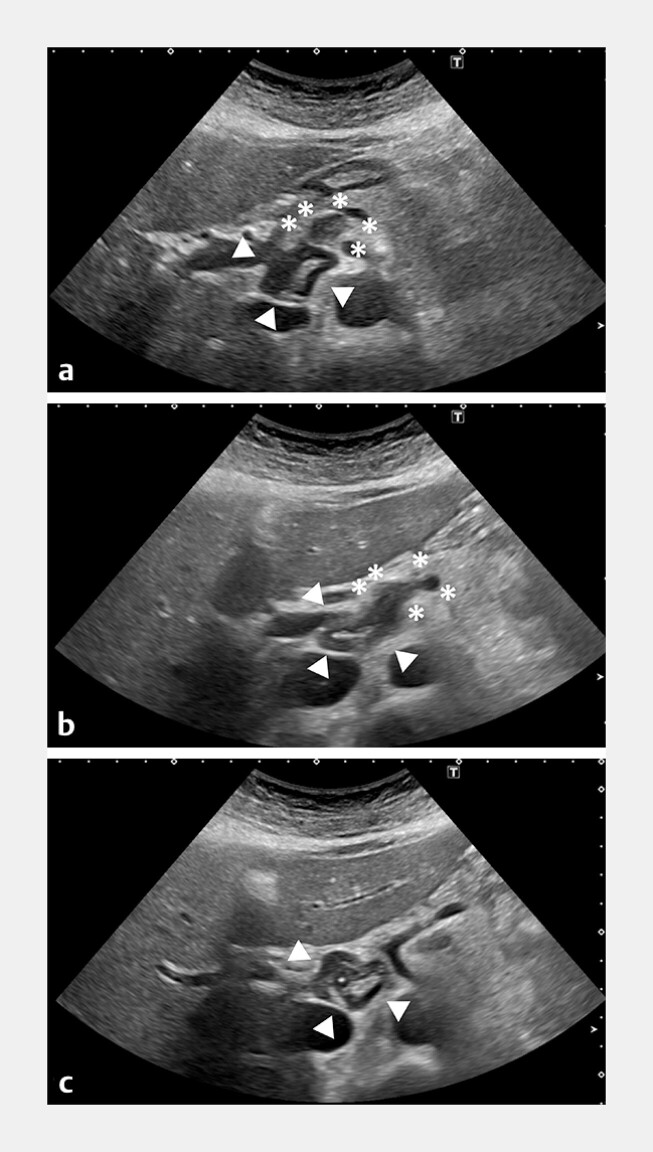 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Lymphatic Disorders and Treatments · Hepatocellular Carcinoma Treatment and Prognosis
Lymphangiomas are rare benign tumors arising from congenital lymphatic system malformations. Intra-abdominal lymphangiomas are uncommon, accounting for less than 5% of lymphangioma cases 1 . Hepatic or hepatoduodenal ligament lymphangiomas are exceedingly rare and of particular clinical interest owing to their anatomical locations.
A 49-year-old woman experienced epigastric pain and nausea early in the morning, followed by pain-induced transient loss of consciousness. She was admitted to the cardiology department with a suspected celiac artery dissection. Subsequent imaging revealed a 4-cm mass in the hepatic hilum; however, a definitive diagnosis could not be established. Abdominal computed tomography (CT) at admission revealed a mildly hyperdense soft tissue area around the celiac artery, without contrast enhancement, suggesting arterial dissection or hematoma. Magnetic resonance imaging (MRI) revealed hematomas of different ages ( Fig. 1 ).
Imaging studies performed for evaluation following emergency admission for epigastric pain. a Contrast-enhanced CT (arterial phase) showing a lesion with almost no enhancement, except for a faint linear enhancement within the mass, possibly reflecting septations or hemorrhage. b Positron emission tomography-CT showing no abnormal FDG uptake in the lesion with no elevation of the standardized uptake value, suggesting no evidence of malignancy. c A MRI T1-weighted image (DIXON opposed-phase) showing the lesion as hypointense, with heterogeneous signal intensity suggestive of an intralesional hemorrhage (asterisk). d A MRI T2-weighted image showing a hyperintense lesion with internal septations and fluid components, consistent with hemorrhage within a lymphangioma (asterisk). CT, computed tomography; MRI, magnetic resonance imaging.
No symptom recurrence occurred during the subsequent 3 months. A hepatic hilar mass was suspected as the cause, and the patient was referred to our department for further evaluation. Follow-up CT conducted 3 months later revealed shrinkage of the lesion, excluding the celiac artery dissection ( Fig. 2 ).
Follow-up contrast-enhanced CT at 3 months following initial presentation. Delayed-phase imaging showing a slight reduction in tumor size, with faint linear enhancement observed along the tumor margin and within the lesion (asterisk). The patient remained asymptomatic without any recurrent abdominal pain during follow-up. CT, computed tomography.
Endoscopic ultrasonography (EUS) revealed a 40-mm mass in the hepatic hilum with internal hyperechoic spots and a marginal solid component believed to be a normal lymph node. Contrast-enhanced EUS using Sonazoid demonstrated minimal contrast within the internal septa, indicating a fibrotic lesion. Based on these findings, a hemorrhagic lymphangioma with secondary degeneration was suspected. Similar findings were obtained on transabdominal ultrasonography ( Fig. 3 , Fig. 4 , Video 1 ).
Endoscopic ultrasound (EUS) findings at 6 months after initial presentation. a EUS demonstrating a lymphangioma (triangle) arising continuously from a normal lymph node (asterisk). A mosaic pattern of mixed echogenicity, continuous with the lymph node structure, can be observed. b A focused EUS view of the lymphangioma showing heterogeneous echotexture with hypoechoic areas and septation-like structures, characteristic of lymphangiomas. c left: A conventional EUS image showing internal septation-like structures and cystic changes within the lesion. c right: Contrast-enhanced EUS taken using a Sonazoid system showing a linear inflow of contrast medium into the lesion, consistent with the faint linear enhancement pattern seen on delayed-phase CT (following on from Fig. 2 ). CT, computed tomography.
Transabdominal ultrasonography at 6 months after initial presentation. a–c Sequential images of the hepatic hilum demonstrating continuity from a lymph node to the lymphangioma. The proper hepatic artery passes through the region surrounded by the lymph node (asterisk) and the lymphangioma (triangle). Panel a presents a lymph node and a lymphangioma, panel b shows the transition from a lymph node to a mass lesion, and panel c depicts the main lymphangioma.
A rare case of hepatic hilar lymphangioma diagnosed using endoscopic and transabdominal ultrasonography.Video 1
The features of lymphangiomas are generally nonspecific, making diagnosis challenging. This case is remarkable as both EUS and transabdominal ultrasonography allowed detailed visualization of a hepatic hilar lymphangioma, which is extremely rare. Contrast-enhanced EUS enabled the noninvasive assessment of the internal tumor architecture, highlighting its potential diagnostic value in characterizing benign cystic or vascular lesions in the hepatic hilum.
Endoscopy_UCTN_Code_CCL_1AF_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.