Hemostasis via an endoscopic full-thickness suturing device with extended cap length method and red dichromatic imaging for deep colonic diverticular bleeding
Takahiro Muramatsu, Masakatsu Fukuzawa, Fumito Yamanishi, Makoto Arashiyama, Fumi Naruse, Tomohiro Kaketani, Takao Itoi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
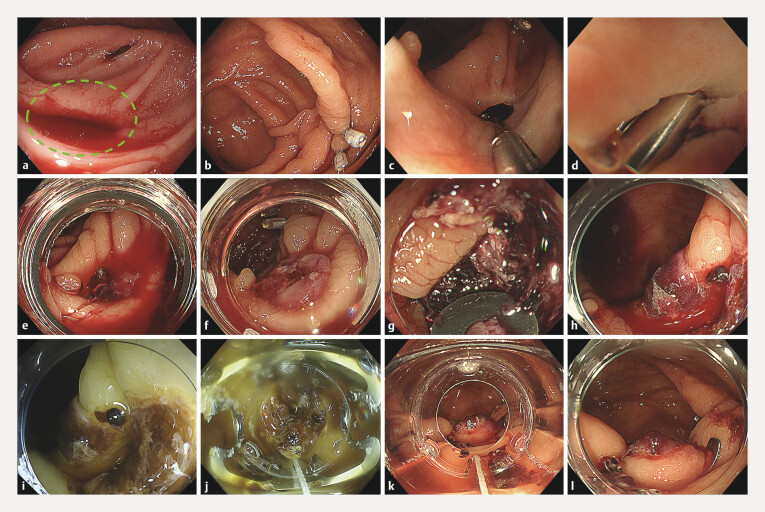 Fig. 1
Fig. 1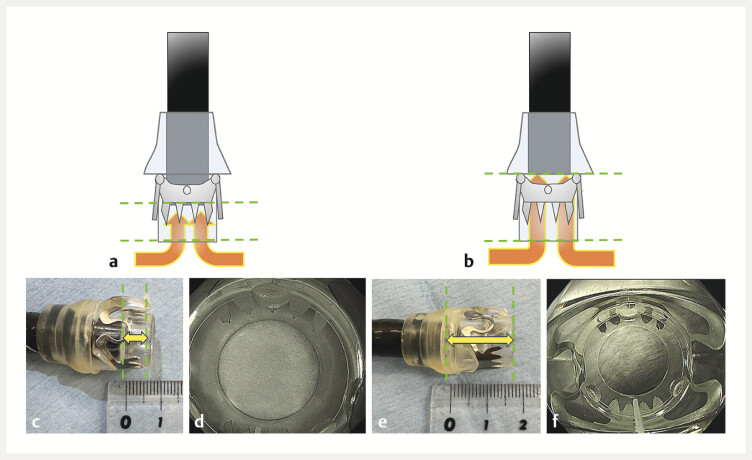 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Bleeding Diagnosis and Treatment · Diverticular Disease and Complications · Colorectal Cancer Screening and Detection
Diverticular bleeding accounts for approximately 60% of cases of acute lower gastrointestinal bleeding and is a common disease 1 . Endoscopic hemostasis is mainly achieved using endoclips or endoscopic band ligation (EBL), although rebleeding may occur. For such cases, an OTS-clip has been reported as an effective option 2 3 . Furthermore, red dichromatic imaging (RDI) can facilitate the identification of the diverticular bleeding site 4 5 . Herein, we describe a case of recurrent diverticular bleeding successfully treated by modifying the OTS-clip setup with an extended cap length method (ECLM) to increase the suction depth and by using RDI to improve the visualization of the bleeding site ( Video 1 ). A 74-year-old man who was taking aspirin for essential thrombocythemia was presented with hematochezia. Computed tomography revealed multiple diverticula, and upon emergency colonoscopy, we discovered active bleeding from a diverticulum of the ascending colon. After marking clips were fixed near the diverticulum, hemostasis was achieved via clipping; however, the diverticulum was so deep that the clips were hidden ( Fig. 1 a–d ). Rebleeding occurred the following day, and EBL yielded temporary hemostasis ( Fig. 1 e, f ), but bleeding recurred several hours later. As both clipping and EBL had failed, hemostasis via an OTS-clip was planned during third colonoscopy. Because the diverticulum was deep and the band had detached ( Fig. 1 g ), the OTS-clip was attached with an extended cap to increase the suction width ( Fig. 2 ). RDI was used to enhance the visibility of the bleeding site within the diverticulum. The diverticulum was fully inverted into the elongated OTS-clip cap, and the clip was deployed, resulting in complete hemostasis ( Fig. 1 h–l ). No further bleeding occurred.
Hemostasis achieved via an OTS-clip with an extended cap length method and red dichromatic imaging for bleeding from a deep colonic diverticulum.Video 1
Endoscopic images. a Active bleeding was observed from a diverticulum in the ascending colon (green dotted circle). b A marking clip was placed near the responsible diverticulum. c A clip was inserted into the diverticulum, which yielded hemostasis. d Primary hemostasis was achieved; however, the diverticulum was so deep that the clips were hidden. e Rebleeding was observed from the previously clipped diverticulum. f Endoscopic band ligation yielded temporary hemostasis. g During the third colonoscopy for recurrent bleeding, we discovered that the previously applied band had detached. h An endoscopic image under white-light imaging. i An endoscopic image under red dichromatic imaging. j The entire diverticulum was suctioned into an OTS-clip via an extended cap length method. k The OTS-clip was successfully deployed. l The OTS-clip was firmly fixed, resulting in successful hemostasis.
Schema of an OTS-clip deployed using an extended cap length method. a Schema of the normal deployment of the OTS-clip. b Appearance of the normal deployment of the OTS-clip. The cap length (from the endoscope tip to the tip of the OTS-clip cap) is 6 mm. c An endoscopic view of the normal deployment of the OTS-clip. d Schema of the OTS-clip deployed via the extended cap length method (ECLM). e Appearance of the OTS-clip deployed via the ECLM. The cap length (from the endoscope tip to the tip of the OTS-clip cap) is 12 mm. f An endoscopic view of the OTS-clip deployed via the ECLM. The endoscopic view is slightly narrower than that with normal deployment, but it does not interfere with the procedure.
In conclusion, an OTS-clip attached via the ECLM enabled the complete inversion and reliable hemostasis of a deep diverticulum. Combined with RDI, this approach may be useful as treatment for refractory diverticular bleeding.
Endoscopy_UCTN_Code_TTT_1AQ_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nagata N Kobayashi K Yamauchi A Identifying bleeding etiologies by endoscopy affected outcomes in 10,342 cases with hematochezia: CODE BLUE-J study Am J Gastroenterol 20211162222223434388140 10.14309/ajg.0000000000001413 PMC 8560163 · doi ↗ · pubmed ↗
- 2Doi H Sasajima K Takahashi M Using an over-the-scope clip for colonic diverticular hemorrhage Dig Endosc 201931 e 80e 8110.1111/den.1338430822362 · doi ↗ · pubmed ↗
- 3Yamaguchi D Tanaka Y Nomura T Over-the-scope clip rescue method of endoscopic hemostasis for severe acute colonic diverticular bleeding Dig Endosc 20243650650710.1111/den.1476438353173 · doi ↗ · pubmed ↗
- 4Saino M Aoyama T Fukumoto A Tracking the target in colonic diverticular bleeding using red dichromatic imaging Endoscopy 202153 E 425E 42610.1055/a-1327-170133506468 · doi ↗ · pubmed ↗
- 5Fukuda S Sakamoto T Suzuki H Utility of red dichromatic imaging for identifying the bleeding point in endoscopic hemostasis of colonic diverticular bleeding Video GIE 2022714915110.1016/j.vgie.2022.01.00235937193 PMC 9349056 · doi ↗ · pubmed ↗