Primary Intraventricular Amelanotic Melanoma: Case Report and Literature Review
Carlos Mávita Corral, Flavio Hernandez-Gonzalez, Kevin S Toache, Marco A Rodriguez-Florido, Luis A Gallego Hermosillo, Alejandro Suarez-Ramirez, Pedro A Gonzalez-Zavala

TL;DR
A rare case of amelanotic melanoma in the brain is reported, highlighting its diagnostic difficulty and poor prognosis despite treatment.
Contribution
This case report adds to the limited literature on primary intraventricular amelanotic melanoma and emphasizes the challenges in diagnosis and treatment.
Findings
The tumor was confirmed as amelanotic melanoma using histopathology and immunohistochemistry.
Despite surgery and immunotherapy, the tumor recurred and led to fatal hepatic failure.
The case underscores the aggressive nature and poor prognosis of this rare tumor.
Abstract
Primary amelanotic melanoma of the central nervous system (CNS) represents an exceedingly rare neoplasm within the category of primary CNS melanocytic tumors. The absence of melanin pigmentation often complicates its identification, necessitating histopathological and immunohistochemical evaluation for accurate diagnosis. We describe the case of a 70-year-old man who presented with Parkinsonian features and was found to have a well-circumscribed intraventricular mass in the left atrium of the lateral ventricle (38×45×29 mm), hypointense on T1-weighted MRI with heterogeneous enhancement. Surgical resection was performed via a trans-intraparietal sulcus approach. Histopathology confirmed amelanotic melanoma, supported by immunopositivity for S-100, Melan-A, and HMB-45. The patient received adjuvant whole-brain radiotherapy followed by immunotherapy with nivolumab and ipilimumab. Although…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
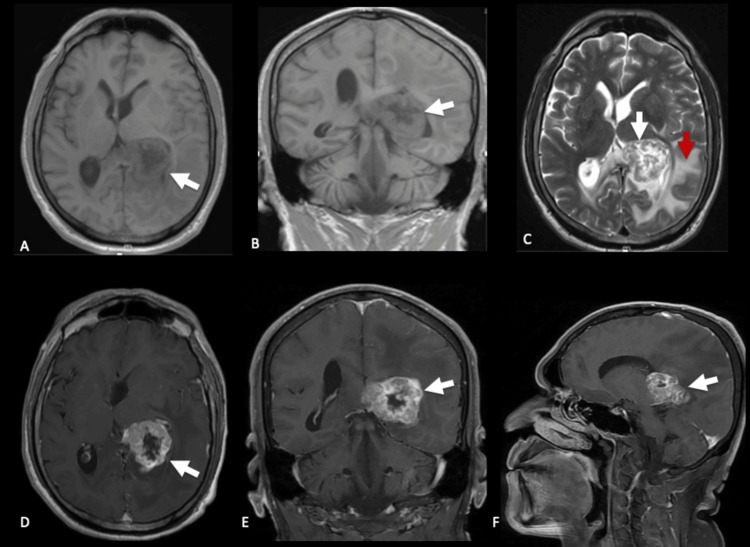 Figure 1
Figure 1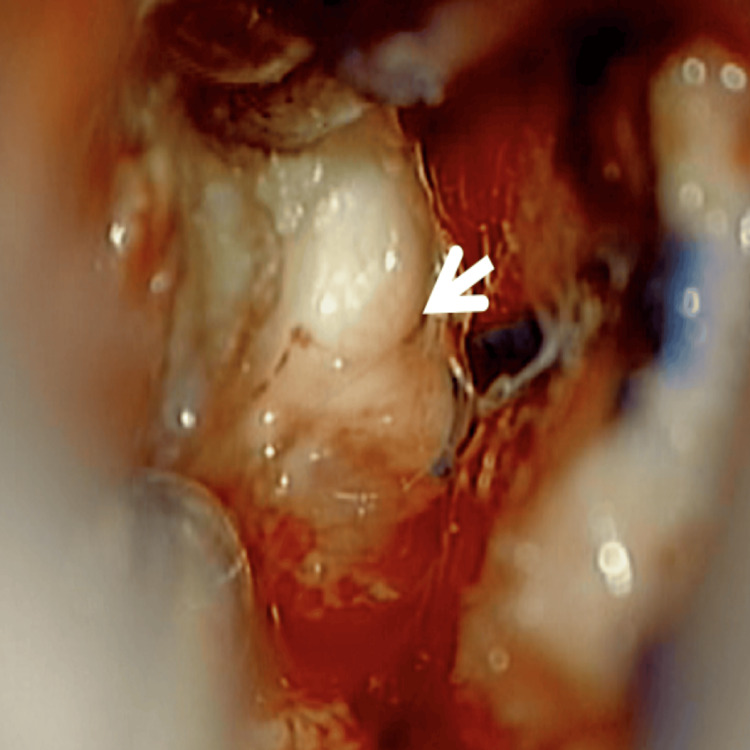 Figure 2
Figure 2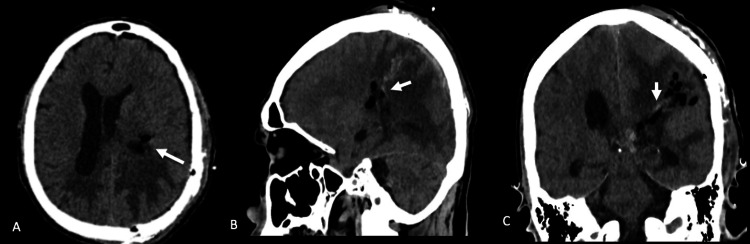 Figure 3
Figure 3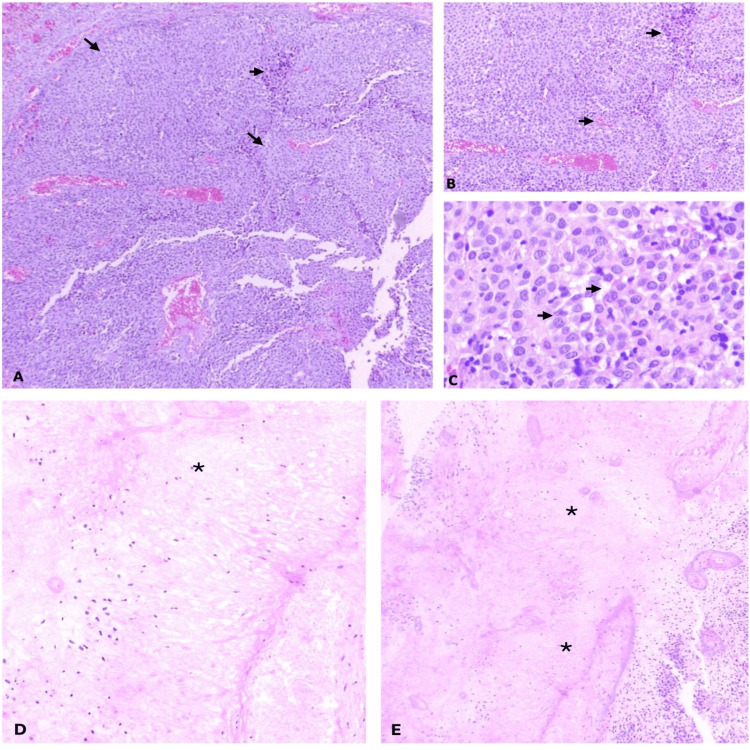 Figure 4
Figure 4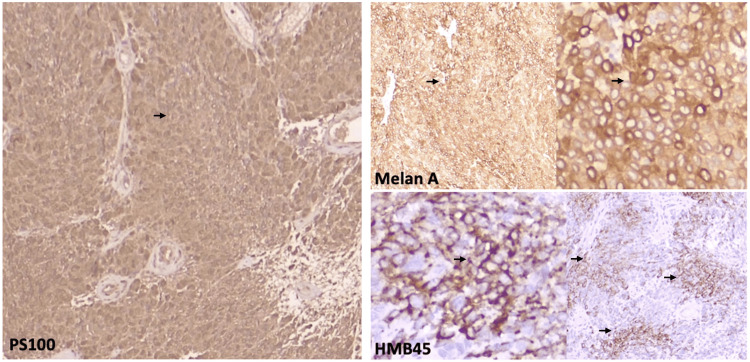 Figure 5
Figure 5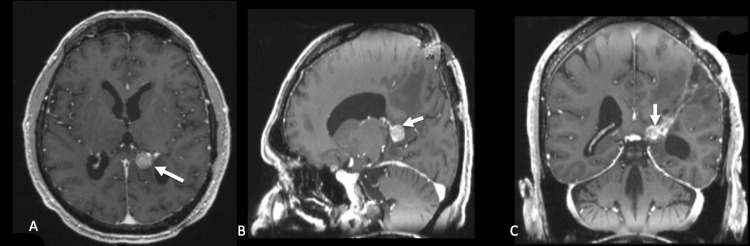 Figure 6
Figure 6| Marker | Result | Diagnostic Significance |
| S-100 | Positive | Highly sensitive marker for melanocytic differentiation; supports the diagnosis of melanoma. |
| Melan-A (MART-1) | Positive | Specific melanocytic marker; indicates melanocytic lineage. |
| HMB-45 | Positive (patchy) | Specific for immature melanosomes; supports melanoma, including metastatic or amelanotic variants. |
| Vimentin | Positive | Mesenchymal marker commonly expressed in melanomas; supportive but non-specific. |
| Ki-67 (7%) | Positive | Indicates proliferative index; low–intermediate proliferation consistent with some metastatic melanomas. |
| Progesterone receptor | Negative | Helps exclude meningioma. |
| EMA | Negative | Further argues against meningioma or epithelial tumors. |
| SSTR2A | Negative | Helps rule out meningioma, which typically shows strong positivity. |
| Pancytokeratin AE1/AE3 | Negative | Excludes carcinoma or epithelial metastases. |
| CK5/6, CK7, CK20 | Negative | Further excludes carcinomas of various origins. |
| p63 | Negative | Helps rule out squamous cell carcinoma. |
| PAGF (placental alkaline phosphatase) | Negative | Argues against germ cell tumors. |
| TTF-1 | Negative | Helps exclude lung or thyroid metastatic carcinoma. |
| Synaptophysin | Negative | Excludes neuroendocrine tumors. |
| Reference | Gender | Age | Location | Clinical symptoms | Histopathology | Treatment | Evolution |
| Shuknecht et al 1990 [ | Male | 53 y | Left parietooccipital meningeal | Seizures and headache, acute bleeding | Polymorphic Vimentin +, HMB45 +++, S100 +++ | Craniotomy and adjuvant radiotherapy. | 5 month recidive, 18 month survival. Reintervention and intrathecal chemotherapy |
| Shuknecht et al 1990 [ | Male | 23 y | Right temporal meningeal | Seizures and headache | Not Specified | Temporal pole lobectomy, radiotherapy and intrathecal chemotherapy | 4 month survival |
| Seki et al 1991 [ | Male | 38 y | Left parietal intraventricular | Headache, memory loss, right hemiparesis, right hemianopsia | Atypical melanosomes in electronic microscopy | Craniotomy and resection | 1 month survival |
| Vanzieleghem et al 1999 [ | Female | 2 y | Right mesencephalic | Hydrocephalus, right ptosis, left eye palsy | Positivity for HMB45, S100 | Ventriculoperitoneal shunt, Biopsy | 1 month survival |
| Li et al 2004 [ | NS | NS | Not Specified | Not Specified | Not Specified | Not Specified | Not Specified |
| Jacob et al 2006 [ | Female | 63 y | Sella and cavernous sinus | Diplopia and bilateral ptosis | Positive for S100, Melan-A and HMB45 | Transsphenoidal hypophysectomy and debulking | Progression to blindness and death |
| Schulz et al 2012 [ | Male | 72 y | Right cerebellar hemispheric, left temporal, thoracic intradural | Headache, nausea, vomit, and gait ataxia | Positivity HMB45, S100 Negativity for Melan A | Craniotomy for cerebellar lesion, resection of spinal lesions | Not Specified |
| Said et al 2014 [ | Male | 60 y | Left frontal | Numbness and dizziness | BRAF V600 mutation | Biopsy and chemotherapy | Not Specified |
| Ma et al 2015 [ | Male | 64 y | Right frontal | Headache, mass in frontal region | Intermediate grade Positivity for HMB45, MelanA, S100, Vimentin, CD99, SMA, CD34 | Right frontal craniotomy | 5 month tumor free |
| Szathmari et al 2016 [ | Female | 5 y | Cystic enlargement of basal cisterns, leptomeningeal, left parietal | Headache, vomiting | Positivity for HMB45, MelanA | Occipitoaxial decompression, endoscopic cystostomy and biopsy, ventriculoperitoneal shunt, chemotherapy | 11 month survival |
| Aslan et al 2018 [ | Female | 44 y | Intracranial and spinal leptomeninges | Nausea, vomiting, weight loss, cognitive deterioration, paraparesis, incontinence | Positivity for S100, HMB45, MelanA | Biopsy, chemotherapy | 4 month survival |
| Mayer et al 2018 [ | Male | 71 y | Cerebellum and spinal metastases (intramedullary T11, epidural L2) | Difficulty for concentration and hand coordination, bilateral dysmetria and unsteady gait | Pleomorphism Positivity for vimentin and HMB45 Negativity for MelanA Ki67 40% | Midline suboccipital approach, radiation | Hydrocephalus, treated with ventriculoperitoneal shunt |
| Zhang et al 2019 [ | Female | 26 y | Posterior fossa meninges, leptomeningeal dissemination | Headache and nausea | Positivity for HMB45, S100, MART1 Ki67 30% BRAF V600E | Right suboccipital craniotomy | 10 month survival |
| Chaharyn et al 2022 [ | Female | 64 y | Cervicomedullary junction | Gait difficulties, dysesthesias | Not Specified | Variant of GNA11 gene | Not Specified |
| Andrés Sanz et al 2022 [ | Female | 63 y | Right frontal | Headache, unstable gait, behavioral changes, right homonymous hemianopia, paraparesis, left facial paralysis | Positivity for HMB45, Vimentin, p53, CD99, S100 Ki 60% Negativity for BRAF V600E | Right frontal craniotomy | Status epilepticus, 3 month survival |
| Polster et al 2023 [ | Male | 62 y | Right frontal | Confusion and left hemiparesis | BRAF V600E mutation | Transorbital transcaruncular | No visual symptoms and good cosmetic outcome at 3 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Cutaneous Melanoma Detection and Management · Glioma Diagnosis and Treatment
Introduction
Primary melanocytic lesions of the central nervous system (CNS) are extremely uncommon, comprising 0.06-0.1% of intracranial tumors and arising from leptomeningeal melanocytes. They range from diffuse entities, such as melanocytosis, to well-circumscribed lesions including melanocytoma, intermediate-grade melanocytic neoplasms, and melanoma [1-5]. Primary CNS melanoma represents a minority within this spectrum, accounting for 1% of all melanomas and 0.07% of brain tumors, with an estimated incidence of 0.005 per 100,000 individuals [6-7]. These tumors may occur anywhere along the neuroaxis, most often in the spinal canal, Meckel’s cave, or posterior fossa [3], and melanocytomas and melanomas collectively represent 0.06-0.1% of meningeal tumors, typically presenting in the fourth or fifth decade of life [6].
Amelanotic melanomas lack significant melanin pigmentation and constitute 0.4-27.5% of cutaneous melanomas, although truly amelanotic variants account for <2% [8,9]. Primary amelanotic melanomas of the CNS are exceptionally rare, with only 16 cases reported [10-23].
Given their rarity and the diagnostic difficulty posed by nonspecific imaging features and variable clinical manifestations, documenting additional cases remains essential. Here, we report a case of primary intraventricular amelanotic melanoma in a 70-year-old man and review current evidence on presentation, anatomical location, histopathology, treatment, and outcomes.
Case presentation
A 70-year-old man with a remote history of resection of a pigmented skin lesion on the left lower back 38 years earlier, without available histopathological documentation, presented for evaluation. Over the previous 15 years, he had developed progressive neuropsychiatric symptoms, including mood instability, irritability, anxiety, self-harming behavior, and memory decline. Two years before admission, he began to exhibit a magnetic gait, followed 18 months later by a stress-exacerbated left-hand tremor. He was recently diagnosed with Parkinson’s disease and initiated on levodopa-carbidopa.
Brain MRI revealed an intraventricular, well-circumscribed lesion with irregular margins, hypointense and heterogeneous on T1, located in the left lateral ventricle atrium, measuring 38×45×29 mm. The lesion showed predominantly peripheral heterogeneous contrast enhancement. On T2-weighted images, the center was hyperintense, and the margins were hypointense, with perilesional edema in the ipsilateral temporal, parietal, and occipital white matter, along with a 15 mm midline shift and leftward dilation of the temporal horns (Figure 1).
Preoperative brain MRI (A, B) Axial and coronal non-contrast T1-weighted images showing a hypointense, heterogeneous intraventricular mass in the left lateral ventricle atrium (white arrows). (C) Axial T2-weighted image demonstrating mixed signal intensity with hypointense and hyperintense components (white arrow) and surrounding vasogenic edema (red arrow). (D–F) Axial, coronal, and sagittal post-contrast T1-weighted images depicting heterogeneous peripheral enhancement (white arrows), consistent with necrotic or hemorrhagic tumor areas.
The patient was admitted and started on steroid therapy with dexamethasone 8 mg every 8hr. On arrival, the patient had hypomimia and was alert, attentive, and oriented with decreased voice tone and memory impairment; however, the rest of the mental functions were intact. The cranial nerve examination was unremarkable. Motor evaluation, the patient demonstrated increased muscle tone in the left upper limb and cervical region, mild right hemiparesis was observed, with proximal muscle strength assessed at 4+/5 and distal strength at 4-/5 according to the Medical Research Council (MRC) muscle strength scale. Additionally, a resting tremor was noted in the left hand.
The patient consented to a surgical intervention initially suspected to address a ventricular atrial meningioma. A horseshoe-shaped incision and centered craniotomy were executed, followed by an intraparietal transsulcal approach to access the ventricular atrium. The surgical excision of a solid tumor, which was firmly adhered to the walls of the ventricular trigone, was successfully completed. Macroscopically, the lesion was non-pigmented (Figure 2).
Intraoperative macroscopic appearance of the lesion.Intraoperative view through a trans-intraparietal sulcus approach showing a non-pigmented, whitish, fibrous, and partially aspiratable intraventricular mass (arrow). The lesion demonstrated a firm consistency with poorly defined margins and absence of melanin pigmentation, consistent with an amelanotic melanoma.
The procedure was conducted without significant intraoperative hemorrhage, and the patient did not require postoperative external ventricular drainage. An immediate postoperative CT scan confirmed complete resection and absence of hemorrhage or hydrocephalus (Figure 3).
Immediate postoperative CT scan(A) Axial, (B) sagittal, and (C) coronal CT images showing small intraventricular air and minimal blood products within the left lateral ventricle atrium (white arrows), without parenchymal hemorrhage or ventricular dilation. No postoperative hydrocephalus is observed.
The patient recovered full muscle strength in the right hemibody within the following week but continued to show symptoms of Parkinsonism.
Intraoperative histopathological evaluation revealed a high-grade, undifferentiated neoplasm. Macroscopically, the specimen consisted of multiple irregular, smooth-surfing tissue fragments with light brown coloration and papillary architecture. Hematoxylin and eosin-stained sections revealed solid neoplastic proliferation arranged in sheets. The tumor cells were ovoid, with moderate eosinophilic cytoplasm and ovoid nuclei exhibiting fine chromatin and mild nuclear pleomorphism (Figure 4).
Histopathological features of a primary intraventricular amelanotic melanoma.(A) Low-power hematoxylin and eosin (H&E)–stained section shows a solid, highly cellular neoplasm with a sheet-like growth pattern and prominent vascularization (arrows). (B) Intermediate magnification demonstrates nests of uniform ovoid tumor cells arranged in perivascular distribution with preserved cohesion and scant intervening stroma (arrows). (C) High-power view reveals polygonal cells with moderate eosinophilic cytoplasm, finely dispersed chromatin, inconspicuous nucleoli, and mild nuclear pleomorphism (arrowheads). No melanin pigment is identified, consistent with an amelanotic phenotype. (D, E) Low-power panoramic views highlight extensive necrotic areas (asterisks) and adjacent viable tumor tissue.
Immunohistochemical analysis showed diffuse positivity for S-100 protein, Melan-A, and HMB-45 in a patchy distribution, vimentin, and a Ki-67 proliferation index of 7% (Figure 5).
Immunohistochemical profile of the primary intraventricular amelanotic melanoma.Immunohistochemistry shows diffuse S-100 positivity (left, arrow), along with strong Melan-A expression (top right, arrows) and focal HMB-45 staining (bottom right, arrows). This melanocytic marker profile, in the absence of melanin pigment on hematoxylin-eosin sections, supports the diagnosis of amelanotic melanoma.
The tumor cells were negative for progesterone receptor, epithelial membrane antigen (EMA), somatostatin receptor 2A (SSTR2A), pancytokeratin AE1/AE3, CK5/6, CK7, CK20, p63, placental alkaline phosphatase (PAGF), thyroid transcription factor-1 (TTF-1), and synaptophysin (Table 1).
Clinical, imaging, and histopathological findings supported the diagnosis of primary amelanotic melanoma. A PET-CT scan was initially planned to evaluate for systemic involvement and to exclude an extracranial melanoma source; however, it could not be performed due to technical failure of the equipment at that time. Instead, a contrast-enhanced thoracoabdominal-pelvic CT scan was obtained, which revealed no suspicious lesions or lymphadenopathy suggestive of another primary melanoma or metastatic disease.
The patient received adjuvant whole-brain radiotherapy (30 Gy in 10 fractions) followed by combined immunotherapy with nivolumab (3 mg/kg every 15 days) and ipilimumab (1 mg/kg every 21 days for four cycles). Five months post-surgery, follow-up MRI revealed local tumor recurrence in the left ventricular atrium, characterized by new nodular enhancement (Figure 6), indicative of aggressive progression. Although treatment was ongoing, the disease continued to advance, and the patient's clinical condition steadily deteriorated. Six months after starting immunotherapy, he experienced immune-related liver damage, indicated by elevated liver function tests: total bilirubin at 6.42 mg/dL (reference: 0.1-1.2 mg/dL), AST at 979 U/L (reference: 5-30 U/L), and ALT at 1273 U/L (reference: 4-36 U/L), which necessitated the cessation of immunotherapy. Ultimately, the patient passed away from the illness one year following surgery.
Follow-up MRI (A) Axial, (B) sagittal, and (C) coronal post-contrast T1-weighted images show a newly developed enhancing nodular lesion in the left lateral ventricle atrium (white arrows), consistent with local tumor recurrence five months after surgery.
Discussion
Central nervous system (CNS) melanocytic tumors are rare neoplasms that may correspond to metastases or, less commonly, to primary lesions [1,24,25]. The latter includes both benign and malignant tumors, which can be either localized or diffuse [1,16,25].
Melanocytic neoplasms originate from melanocytes in the neural crest during early embryogenesis. Melanoblasts migrate dorsolaterally to the skin during the first trimester of gestation. A smaller number of cells travel to mucosal surfaces, such as the aerodigestive and urogenital tracts, inner ear, uvea, and leptomeninges. Therefore, these neoplasms can arise in cutaneous or extracutaneous locations, with the latter being less common [1].
Primary melanomas of the CNS account for less than 1% of all melanomas. Although they can occur anywhere in the nervous system, they are more commonly found in the posterior cranial fossa, spinal cord, and Meckel's cave [3,6,7]. They typically appear between the ages of 15 and 71 years, with a peak incidence in the fifth decade of life [6]. Diagnosis is not straightforward, as it requires the exclusion of systemic melanoma [26].
An unusual variety of melanocytic lesions that seems to defy the nature of this tumor by definition is the amelanotic variant. It lacks melanin pigment or, depending on the definition, may present it in less than 5% of the cells [15]. Reports of amelanotic specimens are rare among melanomas [15]. The clinical features of amelanotic melanoma are similar to those of melanocytic lesions, which are closely related to the tumor's anatomical location and compression of nearby nerves. They commonly present with intracranial hypertension, hydrocephalus, focal neurological deficits, subarachnoid hemorrhage, and seizures [15,27,28].
Magnetic resonance imaging (MRI) is the preferred imaging method for melanoma in the central nervous system; however, its performance is influenced by the amount of melanin and the presence of hemorrhage. Isiklar et al. classified MRI performance into four groups: a) The melanotic group, which shows hyperintensity on T1 and hypointensity on T2; b) Amelanotic group, with iso-/hypointensity on T1 and iso-/hyperintensity on T2. c) Mixed group: does not meet either of the two criteria. d) Hemorrhagic group with features of intra/peritumoral hemorrhage [15,29,30].
In addition to CT and MRI, PET/CT is used as an imaging method for central nervous system melanoma. PET/CT can help MRI clarify the primary lesion and identify metastases [27]. Histologically, primary melanoma cells can present a polygonal or spindle-shaped morphology with marked heterogeneity and abundant mitotic activity. Some tumors may exhibit signs of hemorrhage and necrosis. According to case report findings, the Ki67 proliferation index in primary CNS melanoma ranges from 1% to 30%. HMB-45, Melan-A, and S-100 are specific markers of melanoma. HMB-45 and Melan-A showed limited sensitivity (69%-93% and 75%-92%, respectively), whereas S-100 showed high sensitivity (97%-100%) but low specificity (75%-87%) [27].
In primary CNS melanoma cells, positive expression of HMB45, S-100, and Melan A is observed, while meningeal epithelial membrane antigen, cytokeratin, neuron-specific enolase, and glial fibrillary acidic protein are expressed negatively. This expression pattern is valuable for distinguishing primary CNS melanoma from other tumors. GNAQ and GNA11 mutations are prevalent in primary CNS melanoma but differ from cutaneous melanoma (CM), in which BRAF, NRAS, KIT, and NF-1 mutations are more common [1,8,24,27].
The study of metastatic leptomeningeal melanomas has shown a highly immunosuppressive microenvironment enriched with T-cell populations, with a low percentage of CD4 and NK T-cells but a high percentage of CD8 T-cells. In cases of brain metastatic melanoma, a higher number of activated CD4 cells has been observed [27].
Regarding treatment, resection, radiotherapy, chemotherapy, and biotherapy have shown variable responses as single or combined agents. However, owing to the infrequent and under-researched nature of primary CNS melanomas, an optimal standard treatment has not been defined [3,26].
In a population-based study, Puyana and collaborators analyzed 54 cases of primary malignant CNS melanoma between 1973 and 2015, finding that total macroscopic resection plus radiotherapy and both plus chemotherapy were significantly associated with higher survival rates compared to biopsy [26].
Total macroscopic resection is considered by most authors to be the cornerstone of treatment, as it has significant effects on survival, being especially useful in solitary lesions or large and/or symptomatic metastases with edema [31]. Radiotherapy and chemotherapy have been recommended, whereas partial resection has shown less clear effects on survival [26]. Radiotherapy has shown greater potential as a primary therapy for disseminated CNS melanomas or as an adjuvant post-surgery to prevent progression or recurrence [26]. With single-fraction stereotactic radiosurgery (18 Gy) plus immunotherapy, 12-month control rates for a 7.5 mm lesion were 87.8% compared to 79.8% for radiosurgery alone [32]. Systemic chemotherapy is a treatment for advanced CNS melanoma. The median progression-free survival in patients receiving systemic chemotherapy is approximately five months, and the overall survival is approximately 12.5 months. Currently, chemotherapy regimens for primary CNS melanoma have not been standardized yet. Temozolomide, dacarbazine, platinum-based drugs, and intrathecal methotrexate are commonly used, although most of these chemotherapeutic agents do not cross the blood-brain barrier, with the exception of temozolomide, which has provided survival benefits for some patients [3,27]. Advances in the molecular genetics of tumors have marked the beginning of the era of targeted therapies, which have shown significant clinical benefits in patients with advanced melanoma [27].
Immunotherapy has proven to be promising in improving survival outcomes in advanced melanoma, particularly in cutaneous melanoma. Guo and collaborators collected data on five cases of primary CNS melanoma treated with immunotherapy, who achieved a median overall survival of 58 months (5 to 63 months). These findings indicate the partial efficacy of immunotherapy in treating CNS melanoma and suggest the possibility of greater efficacy when combined with other treatment strategies [27]. Currently, ipilimumab plus nivolumab is the first-line treatment for patients with asymptomatic brain metastases from melanoma. [33]. With a 10-year follow-up, the median overall survival was 71.9 months with this combination treatment. Among patients alive and progression-free at 3 years, the 10-year melanoma-specific survival rate was 96% [34].
Literature review
To better characterize the clinical and pathological features of this rare variant, a literature review was performed, identifying 16 previously reported cases of primary CNS amelanotic melanoma (Table 2). The patients had an average age of 47.3 years. The symptoms varied based on where the tumor was located, with cognitive issues being among the most commonly noted. None of the cases mentioned any preoperative suspicion of the diagnosis. The lesions were reported in various locations, including the brainstem, hemispheric parenchyma, meninges, spine, cerebellum, sella turcica, parasellar region, cranial cavity, and there was one case of a suspected intraventricular lesion.
Pathological findings showed positivity for HMB-45 in 50% of the cases, S-100 positivity in 37.5% of the cases, and MelanA positivity in 31.25% of the cases; we associated these low percentages with the fact that immunochemistry was not performed or mentioned in the case reports. The surgical approach depends on the location and clinical features of the case. The prognosis is generally unfavorable, with an average survival of 6.5 months.
In the present case, an amelanotic melanoma was found in an unusual intraventricular location, initially suspected to be an atrial meningioma. Optimal treatment was achieved with gross total resection and adjuvant radio- and chemotherapy. The patient had a one-year survival but died due to chemotherapy-related complications. Although not widely studied due to the rarity of the amelanotic variant, available evidence suggests that prognosis and survival are worse compared to pigmented melanomas.
Conclusions
Primary intraventricular amelanotic melanoma represents an exceedingly rare and complex central nervous system tumor, necessitating a comprehensive exclusion of extracranial primary sites and relying on immunohistochemical analysis for definitive diagnosis. Despite advancements in therapeutic strategies, the prognosis remains unfavorable due to high recurrence rates and treatment-associated toxicity. This case highlights the tumor's aggressive characteristics and underscores the necessity for thorough evaluation and multidisciplinary management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary melanocytic tumors of the central nervous system: A review with focus on molecular aspects Brain Pathol Küsters-Vandevelde HV Küsters B van Engen-van Grunsven AC Groenen PJ Wesseling P Blokx WA 2092262520152553412810.1111/bpa.12241 PMC 8029366 · doi ↗ · pubmed ↗
- 2Primary melanocytic neoplasms of the central nervous system J Clin Neurosci Liubinas SV Maartens N Drummond KJ 122712321720102055807010.1016/j.jocn.2010.01.017 · doi ↗ · pubmed ↗
- 3Primary meningeal melanocytic tumors of the central nervous system: A review from the ultra-rare brain tumors task force of the European Network for Rare Cancers (Euracan)Cancers (Basel) Pellerino A Verdijk RM Nichelli L Andratschke NH Idbaih A Goldbrunner R 25081620243906114810.3390/cancers 16142508 PMC 11274408 · doi ↗ · pubmed ↗
- 4Primary leptomeningeal melanoma in association with neurocutaneous melanosis: A case report Surg Neurol Int Qazi SS Shah SM Baqai MW Enam SA 5471320223660075610.25259/SNI_856_2022 PMC 9805607 · doi ↗ · pubmed ↗
- 5Primary malignant melanoma of the central nervous system: A diagnostic challenge [Article in Spanish]Cir Cir Quillo-Olvera J Uribe-Olalde JS Alcántara-Gómez LA Rejón-Pérez JD Palomera-Gómez HG 1291348320152598698310.1016/j.circir.2015.04.008 · doi ↗ · pubmed ↗
- 6Primary circumscribed meningeal melanoma involving the Meckel’s cave: A report of a rare case and review of literature Cureus Tajammul SS Rassou SC Munir J Ahmed Z Nadaf AN 016202410.7759/cureus.55427 PMC 1098555638567222 · doi ↗ · pubmed ↗
- 7Primary intracranial malignant melanoma in an adolescent: Case report and literature review Front Surg Golden N Kencana IG Lauren C Saputra A Japardi D 15242041220253999615110.3389/fsurg.2025.1524204 PMC 11849180 · doi ↗ · pubmed ↗
- 8A unique case of intracranial amelanotic melanoma with BRAF V 600E mutation successfully treated via molecular-targeted therapy NMC Case Rep J Fujita J Tomita Y Ichimura K 67731020233706587510.2176/jns-nmc.2022-0227 PMC 10101700 · doi ↗ · pubmed ↗