Hemolytic anemia induced by malpositioned covered stent following acute type A aortic dissection repair
Shanliang Chen, Xiaozhou Zheng, Huimin Cui

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
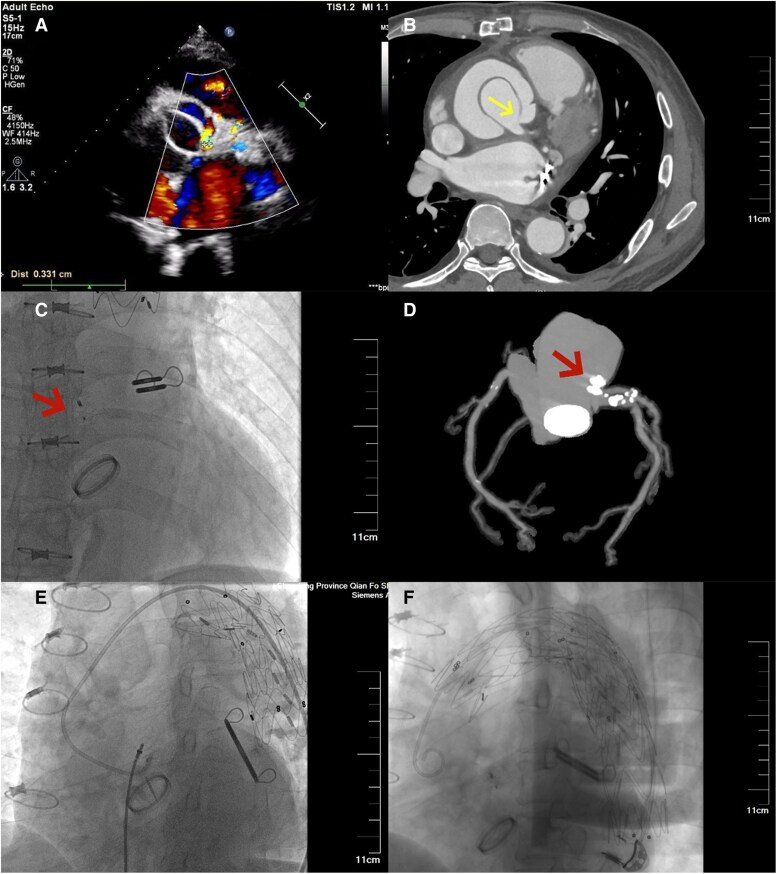 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Blood transfusion and management · Blood properties and coagulation
Case description
A 57-year-old male with a history of Bentall, Sun's procedure and left atrial appendage clip occlusion performed 3 months prior was admitted for haemolytic anaemia. Aortic computed tomography angiography (CTA) and transthoracic echocardiography (TTE) revealed coronary anastomotic leaks via the aortic wrap to the right atrium: one left-sided (3.3 mm) and two right-sided (2.9 and 1.2 mm) (Panels A and B).
**
Digital subtraction angiography (DSA)-guided leak occlusion was performed. A 5-mm ventricular septal defect occlude (Lifetech Scientific, Inc. Shenzhen, China) successfully sealed the primary left leak (Panels C and D); however, intra-operative DSA fluoroscopy demonstrated a retrograde placed stent silhouette at the distal aortic arch, which swung continuously in the distal aortic arch throughout the cardiac cycle (Panel E), causing mechanical destruction of blood, suggesting a causal relationship with haemolytic anaemia. Further history review revealed that the initial frozen elephant trunk (FET) procedure was performed using a 30-30-080 covered stent (Weiqiang Medical Tech, Co., Ltd, Hangzhou, China). However, it was retrograde placed with its morphological distal end anchored within a 28-mm Four-Branched artificial vascular graft at the distal aortic arch. One month later, thoracic endovascular aortic repair (TEVAR) was performed to deploy a covered stent (Medtroni, 30-30-150) to secure the swinging stent to prevent any further movement (Panel F). A compliant balloon was then advanced to the malpositioned stent segment and inflated to remodel the stent-graft. At 1-month follow-up, haemoglobin levels trended from 56 g/L (second admission) to 50 g/L (third admission), rising to 102 g/L recently.
Haemolytic anaemia is a catastrophic complication following acute type A aortic dissection repair. Severe anaemia may necessitate transfusion, and its management remains clinically challenging.