Sustained efficacy of spesolimab following flare-up dose in achieving long-term skin clearance in generalized pustular psoriasis: A case report and review of literature
Abdullah Faisal Albadri, Abdullah Ayman Aman, Abdulrahman Esam Azhar, Saif Yaseer Ashram

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1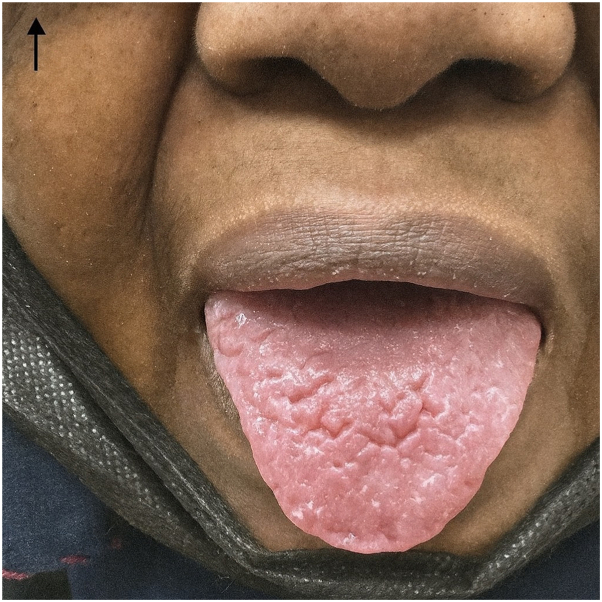 Figure 2
Figure 2 Figure 3
Figure 3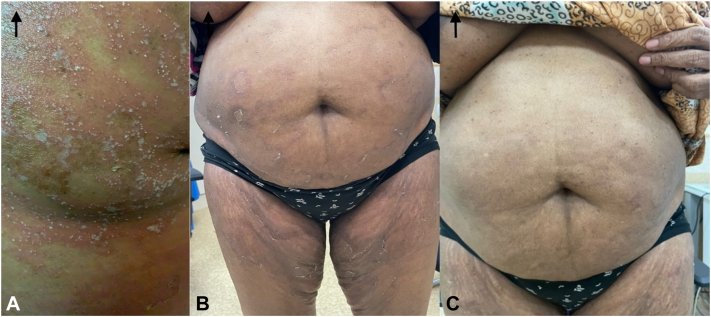 Figure 4
Figure 4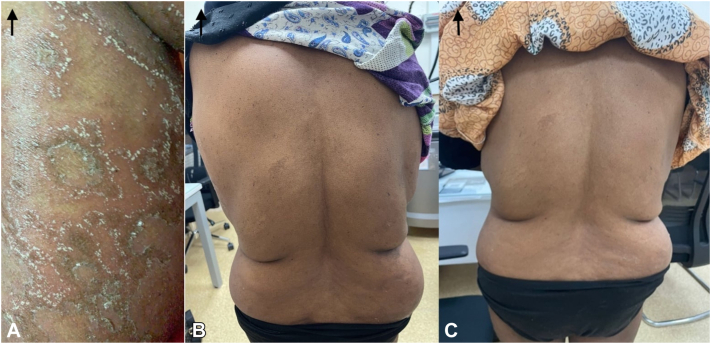 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis · Dermatology and Skin Diseases · Hidradenitis Suppurativa and Treatments
Introduction
Generalized pustular psoriasis (GPP) is a rare and potentially life-threatening form of psoriasis characterized by the sudden onset of sterile pustules on erythematous skin, often accompanied by systemic symptoms such as fever, malaise, and fatigue.1^,^2 Unlike plaque psoriasis, GPP is driven primarily by dysfunction of the interleukin-36 (IL-36) pathway.3 Traditional systemic therapies have often provided limited efficacy, underscoring the need for more targeted treatment strategies.1
Spesolimab, an IL-36 receptor inhibitor, has recently emerged as a promising therapy, demonstrating rapid resolution of GPP flares.4 We present the case of a 59-year-old woman with long-standing psoriatic arthritis (PsA) and GPP who experienced marked improvement and sustained remission following a single intravenous infusion of spesolimab.
Case presentation
A 59-year-old female, known to have psoriatic arthritis (PsA) for the past 20 years and type 2 diabetes mellitus for 1 year, presented as a follow-up case of GPP. She was seen in the dermatology clinic on the 8th and 29th of December 2024, corresponding to 10- and 31-days following administration of a flare-up dose of Spesolimab (900 mg IV). The patient has a history of recurrent, episodic, annular, and pruritic skin lesions that began in 2019, which were often associated with vesicle formation. The eruptions were distributed across the entire body, primarily involving the abdomen, back, and thighs, with sparing of the face, palms, and soles. The skin lesions were temporarily alleviated by topical treatments, including mometasone and Fucidin creams. No specific aggravating factors were identified, and she reported multiple similar episodes over the years.
Her past medical history was notable for PsA and diabetes, for which she was on oral hypoglycemic therapy (metformin 500 mg once daily). She had no known allergies and no history of prior hospitalizations. Family history was unremarkable for dermatological conditions. Socially, she was a non-smoker, of low socioeconomic background, with no recent travel history. Her Dermatology Life Quality Index (DLQI) score was 21, reflecting a significant impact on her quality of life.
Laboratory investigations at baseline were unremarkable, with normal complete blood count, liver function tests, renal function tests, and negative serology. C-reactive protein was elevated at 17 mg/L, indicating systemic inflammation. Screening for tuberculosis, including purified protein derivative and chest X-ray, was negative. A prior skin biopsy taken from the right side of the abdomen during an earlier follow-up visit confirmed the diagnosis of GPP (Fig 1, A and B).Fig 1A, (hematoxylin and eosin, 10×) and (B) (hematoxylin and eosin, 4×). Histopathology showing regular acanthosis with a prominent sub-corneal neutrophilic collection and patchy parakeratosis.
She reported systemic symptoms of fatigue and malaise, though there were no signs of fever, headache, or anorexia. On mucosal examination, a fissured tongue was noted (Fig 2), while there was no ocular or gastrointestinal involvement, and the nails appeared normal.Fig 2. Fissured tongue as presented on oral cavity physical exam.
Prior to the administration of Spesolimab, on the 28th of November, physical examination revealed the presence of sterile, non-follicular pustules ranging between 2 and 3 mm in size. These pustules showed a tendency to coalesce, forming “lakes” of pus, particularly over the lower limbs and abdomen. As the lesions evolved, they dried and left behind residual erythema and desquamation, which was especially evident on the back and right arm. A Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) score was calculated based on erythema, pustulation, and scaling, with each component scored 3 out of 4, giving a mean severity score of 3.3.
Ten days after receiving Spesolimab (on the 8th of December), the patient reported marked clinical improvement. She denied any recurrence of pustules, erythema, or itchiness. Furthermore, systemic symptoms such as fever and chills—commonly observed during GPP flare-ups—were absent. Physical examination corroborated her report, with no evidence of pustules or erythema and only minor residual desquamation. The GPPGA score had significantly improved to a mean of 0.33 (erythema: 0, pustules: 0, scaling: 1) (Fig 3, Fig 4, Fig 5 to 6).Fig 3A-C, Pre- and post-treatment (day 10 and day 31): Right arm images.Fig 4A-C, Pre- and post-treatment (day 10 and day 31): Abdomen images.Fig 5A-C, Pre- and post-treatment (day 10 and day 31): Back images.Fig 6A-D, Pre- and post-treatment (day 10 and day 31): Lower limb images.
At the 31-day follow-up on the 29th of December, the patient's skin was completely clear, with no residual pustules, erythema, or scaling. Systemic symptoms remained absent. A repeat GPPGA assessment showed a perfect score of 0 across all domains (mean score: 0), indicating complete clinical remission of the GPP flare-up following a single intravenous dose of Spesolimab (Fig 3, Fig 4, Fig 5 to 6). Furthermore, the patient reported sustained clearance of skin lesions and complete absence of pruritus from the time of the flare-up dose until June 2025, mirroring the results observed at the 31-day follow-up.
Discussion
GPP is a rare and severe form of psoriasis characterized by widespread pustules and systemic symptoms. Traditional therapies, including corticosteroids, retinoids, cyclosporine, and tumor necrosis factor alpha inhibitors, often yield inconsistent results and may not be well tolerated.5 Increasing evidence implicates the IL-36 pathway in GPP pathogenesis, making IL-36 inhibition an attractive therapeutic target.3 Spesolimab, a monoclonal antibody against the IL-36 receptor, has recently demonstrated rapid efficacy in GPP flares.4
Two pivotal trials have shaped our understanding of spesolimab. In Effisayil-1, a single intravenous dose produced significant short-term improvements, with rapid pustular clearance observed within 1 week.6 However, durability beyond the acute flare was limited, and many patients required additional therapy. In contrast, Effisayil-2 demonstrated that long-term disease control typically required maintenance infusions every 4 weeks.10 These findings suggest that while a single dose is highly effective for acute flares, sustained remission usually depends on repeated dosing.
Our patient’s course differs from these results. After a single 900 mg infusion of spesolimab, she achieved complete clearance within 1 month and, notably, maintained remission for over 6 months without any maintenance therapy. This outcome highlights potential variability in patient responses. Similar long-lasting responses have occasionally been reported. Brigenti et al described a woman with refractory GPP who achieved 12 months of remission after a single dose.7 Morita et al and Elewski et al also observed substantial improvements in subsets of patients without early retreatment.8^,^9 These findings, together with our case, suggest that for some patients, durable disease control may be achievable with a single infusion.
The clinical implications are important. If certain patients can maintain remission without repeated dosing, this approach could reduce treatment burden, lower healthcare costs, and minimize risks associated with prolonged immunosuppression. At the same time, most trial data indicate that regular maintenance is required, and vigilance regarding safety—particularly infections—remains necessary. Larger prospective studies are needed to identify predictors of durable response and to clarify which patients may benefit from a single-dose strategy versus those requiring ongoing therapy.
Conflicts of interest
None disclosed. The preparation, writing, and conclusions presented in this case report on the use of Spesolimab for a GPP flare were conducted independently and without external influence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rivera-Díaz R.Daudén E.Carrascosa J.M.De La Cueva P.Puig L.Generalized pustular psoriasis: a review on clinical characteristics, diagnosis, and treatment Dermatol Ther 133202367368810.1007/s 13555-022-00881-0PMC 983692436635445 · doi ↗ · pubmed ↗
- 2Choon S.E.Navarini A.A.Pinter A.Clinical course and characteristics of generalized pustular psoriasis Am J Clin Dermatol 23S 12022212910.1007/s 40257-021-00654-z 35061227 PMC 8801409 · doi ↗ · pubmed ↗
- 3Sachen K.L.Greving C.N.A.Towne J.E.Role of IL-36 cytokines in psoriasis and other inflammatory skin conditions Cytokine 156202215589710.1016/j.cyto.2022.15589735679693 · doi ↗ · pubmed ↗
- 4Bernardo D.Thaçi D.Torres T.Spesolimab for the treatment of generalized pustular psoriasis Drugs 8412023455810.1007/s 40265-023-01988-038114719 PMC 10789831 · doi ↗ · pubmed ↗
- 5Krueger J.Puig L.Thaçi D.Treatment options and goals for patients with generalized pustular psoriasis Am J Clin Dermatol 23S 12022516410.1007/s 40257-021-00658-9PMC 880140835061230 · doi ↗ · pubmed ↗
- 6Bachelez H.Choon S.E.Marrakchi S.Trial of spesolimab for generalized pustular psoriasis New Engl J Med 3852620212431244010.1056/nejmoa 211156334936739 · doi ↗ · pubmed ↗
- 7Brigenti N.Gisondi P.Bellinato F.Girolomoni G.Generalized pustular psoriasis successfully treated with spesolimab: a case report SAGE Open Med Case Rep 1220242050313 X 24123545110.1177/2050313 x 241235451 PMC 1090106338419797 · doi ↗ · pubmed ↗
- 8Morita A.Tsai T.Yee E.Y.W.Efficacy and safety of spesolimab in Asian patients with a generalized pustular psoriasis flare: results from the randomized, double-blind, placebo-controlled Effisayil TM 1 study J Dermatol 502202218319410.1111/1346-8138.1660936282833 PMC 10092680 · doi ↗ · pubmed ↗