COVID‐19‐Related Hematological Abnormalities Among Adults; A Cross‐Sectional Study in a Resource‐Limited Setting
Charles Nkansah, Felix Osei‐Boakye, Samuel K. Appiah

TL;DR
This study found that many adults with COVID-19 in a resource-limited setting had blood-related issues like anemia and low platelet counts, which are linked to more severe disease.
Contribution
The study provides insights into hematological abnormalities in a resource-limited setting, emphasizing their clinical relevance for managing severe COVID-19.
Findings
Anemia was present in 60.4% of patients, with normocytic and macrocytic types being most common.
Thrombocytopenia was detected in 56.2% of patients, and blood cell counts predicted severe disease.
Older adults and rural residents were more likely to experience anemia.
Abstract
Alterations in hematological parameters in SARS‐CoV‐2 infection may contribute to disease severity and poor outcomes. This study reports the hematological profile of COVID‐19 patients. This was a cross‐sectional study involving 169 confirmed COVID‐19 patients conducted at Sunyani Teaching Hospital between January and August, 2022. Sociodemographic, clinical, and laboratory data were obtained. Full blood count was performed using an automated hematology analyzer, and systemic inflammatory indices were calculated. Participants were mostly young adults (51.5%), females (53.8%), resided in urban settings (41.4%), and aged 20‐81 years with a median age of 35.0 (29.0–47.0) years. Overall, anemia was present in 60.4% of the COVID‐19 patients (56.4% in males and 63.7% in females), with 23.7%, 23.7%, and 13.0% experiencing mild, moderate, and severe anemia, respectively. The COVID‐19 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
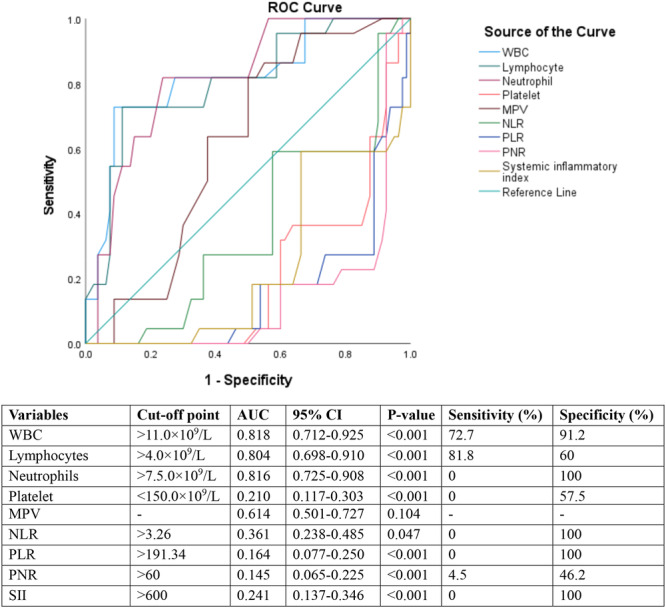 Figure 1
Figure 1| Variables | Frequency | Percentage (%) |
|---|---|---|
| Age (years) | ||
| Median (25th–75th percentiles) | 35.0 (29.0–47.0) | |
| Adolescents (≤ 24) | 21 | 12.4 |
| Young adults (25–40) | 87 | 51.5 |
| Middle‐aged adults (41–60) | 40 | 23.7 |
| Old adults (> 60) | 21 | 12.4 |
| Sex | ||
| Males | 78 | 46.2 |
| Females | 91 | 53.8 |
| Residence | ||
| Urban | 70 | 41.4 |
| Peri‐urban | 49 | 29.0 |
| Rural | 50 | 29.6 |
| Variables | Frequency | Percentage (%) |
|---|---|---|
| Signs and symptoms | ||
| Headache | ||
| Present | 67 | 39.6 |
| Absent | 102 | 60.4 |
| Cough | ||
| Present | 104 | 61.5 |
| Absent | 65 | 38.5 |
| Nausea | ||
| Present | 44 | 26.0 |
| Absent | 125 | 74.0 |
| Loss of smell | ||
| Present | 95 | 56.2 |
| Absent | 74 | 43.8 |
| Loss of taste | ||
| Present | 97 | 57.4 |
| Absent | 72 | 42.6 |
| Fatigue | ||
| Present | 87 | 51.5 |
| Absent | 82 | 48.5 |
| Fever | ||
| Present | 101 | 59.8 |
| Absent | 68 | 40.2 |
| Disease severity | ||
| Severe COVID‐19 | 53 | 31.4 |
| Mild/Moderate COVID‐19 | 116 | 68.6 |
| Vital signs | ||
| Temperature (°C) | 37.6 ± 1.3 | |
| Systolic BP (mmHg) | 132.0 (123.0–147.0) | |
| Diastolic BP (mmHg) | 81.0 (72.0–88.0) | |
| SpO2 (%) | 94.0 (90.0–97.0) | |
| Pulse (bpm) | 90.0 (84.0–97.0) |
| Blood cell parameters | COVID‐19 Patients |
| ||
|---|---|---|---|---|
| Total | Males ( | Females ( | ||
| RBC (/L) | 3.5 ± 0.8 | 3.7 ± 0.8 | 3.3 ± 0.8 | < 0.001 |
| Hb (g/dL) | 11.1 ± 2.4 | 11.6 ± 2.4 | 10.6 ± 2.2 | 0.004 |
| HCT (%) | 33.0 ± 7.3 | 35.7 ± 7.3 | 30.7 ± 6.4 | < 0.001 |
| MCV (fL) | 95.7 ± 11.7 | 95.1 ± 13.2 | 96.3 ± 10.3 | 0.526 |
| MCH (pg) | 33.3 ± 4.9 | 32.8 ± 5.0 | 33.7 ± 4.8 | 0.267 |
| MCHC (g/dL) | 34.6 ± 2.0 | 34.3 ± 1.4 | 35.0 ± 2.4 | 0.026 |
| RDW‐CV (%) | 14.6 (13.6–15.5) | 14.5 (13.6–15.0) | 14.8 (13.5–15.8) | 0.133 |
| WBC (×/L) | 6.1 (4.2–9.7) | 5.3 (3.9–9.7) | 6.4 (5.4–9.7) | 0.062 |
| Neutrophil (×/L) | 2.1 (1.6–2.9) | 2.0 (1.4–2.7) | 2.1 (1.8–3.1) | 0.058 |
| Lymphocyte (×/L) | 3.3 (2.1–6.2) | 3.0 (1.9–6.5) | 3.6 (2.8–6.2) | 0.184 |
| MID (×/L) | 0.4 (0.3–0.6) | 0.4 (0.3–0.6) | 0.4 (0.3–0.7) | 0.210 |
| Platelet (×/L) | 132.0 (105.4–182.9) | 132.0 (108.0–179.8) | 135.0 (103.0–212.0) | 0.514 |
| MPV (fL) | 8.3 (7.6–8.8) | 8.3 (7.7–9.4) | 8.4 (7.5–8.8) | 0.375 |
| PDW (%) | 15.4 (11.7–15.9) | 15.4 (11.9–15.9) | 15.3 (7.1–15.8) | 0.085 |
| NLR | 0.6 (0.4–0.8) | 0.5 (0.4–0.8) | 0.6 (0.5–0.8) | 0.668 |
| PLR | 53.1 (17.3–75.4) | 52.9 (17.3–75.4) | 53.1 (16.3–77.5) | 0.707 |
| PNR | 66.3 (44.1–121.2) | 65.3 (46.7–111.0) | 69.6 (41.2–121.2) | 0.635 |
| SII | 91.0 (45.9–142.1) | 80.5 (49.6) | 92.4 (45.9–150.4) | 0.201 |
| Variables | Mild/moderate COVID‐19 ( | Severe COVID‐19 ( |
|
|---|---|---|---|
| Age (years) | 33 (28.0–43.50) | 44 (31.5–55.5) | < 0.001 |
| Vital signs | |||
| Temperature (°C) | 37.3 ± 1.5 | 38.3 ± 0.6 | < 0.001 |
| Systolic BP (mmHg) | 130.0 (116.5–142.0) | 153.0 (128.0–159.0) | < 0.001 |
| Diastolic BP (mmHg) | 79.0 (72.0–86.0) | 84.0 (74.5–91.0) | 0.117 |
| SpO2 (%) | 95.0 (92.0–97.0) | 88.0 (87.0–94.0) | < 0.001 |
| Pulse (bpm) | 86.5 (83.0–94.0) | 97.0 (87.5–104.5) | < 0.001 |
| Full blood count | |||
| RBC (/L) | 3.7 ± 0.8 | 2.9 ± 0.7 | < 0.001 |
| Hb (g/dL) | 12.3 ± 1.5 | 8.5 ± 1.8 | < 0.001 |
| HCT (%) | 36.0 ± 5.6 | 26.4 ± 6.0 | < 0.001 |
| MCV (fL) | 97.6 ± 11.2 | 91.6 ± 11.9 | 0.002 |
| MCH (pg) | 33.8 ± 4.7 | 32.1 ± 5.2 | 0.039 |
| MCHC (g/dL) | 34.5 ± 1.8 | 34.9 ± 2.5 | 0.351 |
| RDW‐CV (%) | 14.4 (13.2–15.1) | 14.9 (14.5–16.4) | < 0.001 |
| WBC (×/L) | 5.3 (3.7–6.8) | 9.9 (8.3–13.1) | < 0.001 |
| Neutrophil (×/L) | 1.9 (1.2–2.4) | 3.0 (2.6–3.9) | < 0.001 |
| Lymphocyte (×/L) | 2.8 (1.9–3.8) | 6.5 (5.1–9.3) | < 0.001 |
| MID (×/L) | 0.4 (0.3–0.6) | 0.6 (0.3–0.8) | 0.024 |
| Platelet (×/L) | 162.5 (117.4–210.3) | 91.8 (76.3–116.0) | < 0.001 |
| MPV (fL) | 8.3 (7.4–9.1) | 8.3 (8.2–8.5) | 0.962 |
| PDW (%) | 15.4 (12.0–15.9) | 15.5 (8.7–15.9) | 0.392 |
| NLR | 0.5 (0.3–0.7) | 0.6 (0.5–0.8) | < 0.001 |
| PLR | 14.1 (7.9–36.3) | 58.4 (49.3–83.5) | < 0.001 |
| PNR | 32.0 (22.3–48.1) | 95.7 (59.7–145.3) | < 0.001 |
| SII | 38.3 (30.6–67.9) | 108 (80.5–152.0) | < 0.001 |
| Variables | Comments | Reference interval | Frequency | Percentages | |
|---|---|---|---|---|---|
| Hemoglobin (g/dL) | Males | Normal | ≥ 13.0 | 34 | 43.6 |
| Mild anemia | 11.0–12.9 | 19 | 24.4 | ||
| Moderate anemia | 8.0–10.9 | 19 | 24.4 | ||
| Severe anemia | < 8.0 | 6 | 7.7 | ||
| Females | Normal | ≥ 12.0 | 33 | 36.3 | |
| Mild anemia | 11.0–11.9 | 21 | 23.1 | ||
| Moderate anemia | 8.0–10.9 | 21 | 23.1 | ||
| Severe anemia | < 8.0 | 16 | 17.6 | ||
| MCV (fL) | Normal | 80.0–100.0 | 92 | 54.4 | |
| Microcytosis | < 80.0 | 13 | 7.7 | ||
| Macrocytosis | > 100.0 | 64 | 37.9 | ||
| MCH (pg) | Normal | 27.0–31.0 | 156 | 92.3 | |
| Hypochromasia | < 27.0 | 13 | 7.7 | ||
| RDW‐CV (%) | Normal | 11.0–14.5 | 62 | 36.7 | |
| Low | < 11.0 | 19 | 11.2 | ||
| High | > 14.5 | 88 | 52.1 | ||
| Leucocytes (×109/L) | Normal | 4.0–11.0 | 102 | 60.4 | |
| Leucopenia | < 4.0 | 38 | 22.5 | ||
| Leucocytosis | > 11.0 | 29 | 17.2 | ||
| Neutrophils (×/L) | Normal | 2.0–7.5 | 100 | 59.2 | |
| Neutropenia | < 2.0 | 69 | 40.8 | ||
| Lymphocytes (×/L) | Normal | 1.0–4.0 | 102 | 60.4 | |
| Lymphocytosis | > 4.0 | 67 | 39.6 | ||
| Platelet (×/L) | Normal | 150–450 | 74 | 43.8 | |
| Mild thrombocytopenia | 101–149 | 62 | 36.7 | ||
| Moderate thrombocytopenia | 51–100 | 27 | 16.0 | ||
| Severe thrombocytopenia | ≤ 50 | 4 | 2.4 | ||
| MPV (fL) | Normal | 8.0–12.5 | 114 | 67.5 | |
| Low | < 8.0 | 55 | 32.5 | ||
| PDW (%) | Normal | 10.0–17.9 | 141 | 83.4 | |
| Low | < 10.0 | 25 | 14.8 | ||
| High | > 17.9 | 3 | 1.8 | ||
| Multiple abnormalities | No abnormality | — | 30 | 17.8 | |
| Single abnormality | — | 46 | 27.2 | ||
| Bicytopenia | — | 63 | 37.3 | ||
| Pancytopenia | — | 30 | 17.8 | ||
| Variables | Anemic COVID‐19 patients | ||||
|---|---|---|---|---|---|
| Mild/moderate anemia ( | Severe anemia ( |
| aOR (95% CI) |
| |
| Age group | < 0.001 | ||||
| Adolescents | 9 (100) | 0 (0) | 1 | — | |
| Young adults | 48 (94.1) | 3 (5.9) | 2.031 | 0.291 | |
| Middle‐aged adults | 18 (69.2) | 8 (30.8) | 4.435 | 0.034 | |
| Old adults | 5 (31.3) | 11 (68.8) | 6.600 | 0.004 | |
| Sex | 0.09 | ||||
| Males | 38 (86.4) | 6 (13.6) | — | — | |
| Females | 42 (72.4) | 16 (27.6) | — | — | |
| Residence | < 0.001 | ||||
| Urban | 39 (95.1) | 2 (4.9) | 1 | — | |
| Peri‐urban | 26 (100) | 0 (0) | 1.888 | 0.189 | |
| Rural | 15 (42.9) | 20 (57.1) | 3.759 | 0.012 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Dermatological and COVID-19 studies · COVID-19 Impact on Reproduction
Introduction
1
The advent of Coronavirus disease 2019 (COVID‐19), caused by severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2), has posed a devastating threat to global health claiming numerous lives and negatively influencing economic stabilities especially in underserved countries [1]. Following the first detection of the beta‐coronavirus in Wuhan, China, in late 2019, approximately 800 million individuals have been infected with over seven million mortalities reported globally. In Africa, the magnitude of COVID‐19 has been substantial, where almost 13 million cases and 258,892 SARS‐CoV‐2‐related deaths have occurred. Since Ghana detected its first two cases of COVID‐19 on March 12, 2020 in samples from two immigrants who had lately returned from Turkey and Norway, the country has suffered approximately 200,000 cases and 1462 deaths [2, 3]. SARS‐CoV‐2 is principally transmitted via respiratory droplets and aerosols during close proximity with infected people, and this promotes the virus' interactions with its primary receptor angiotensin‐converting enzyme‐2 (ACE‐2) especially in the pulmonary region. Owing to the general distribution of ACE‐2 in the body, SARS‐CoV‐2 eventually affects other parts triggering both pulmonary and systemic problems [4]. COVID‐19 presents with a broad spectrum of clinical manifestations, from subclinical cases to severe respiratory failure and multi‐organ dysfunction. Although the respiratory tract is the prime target, COVID‐19 also causes systemic inflammation that induces a massive cytokine storm and eventually affects multiple organs, including the cardiovascular, gastrointestinal, renal, and hemopoietic systems [5].
A notable systemic manifestation of COVID‐19 is the modification of hematological parameters. The direct interaction of SARS‐CoV‐2 with the bone marrow suppresses its hemopoietic activities, and this affects the production, morphology, and function of blood cells, and such hematological disorders are linked with disease progression and severity [5, 6]. Anemia remains one of the most popular hematological abnormalities observed in COVID‐19 patients. Complex mechanisms such as inflammation‐induced suppression of erythropoiesis, direct interaction of SARS‐CoV‐2 with hemopoietic stem cells, dysregulated iron metabolism, haemolysis, and the implication of cytokine storms that retard red blood cell survival and production, are associated with the development of anemia in COVID‐19 [7, 8, 9]. The significant association between anemia and adverse outcomes in SARS‐CoV‐2 infection, including augmented hospitalization, oxygen requirement, and mortality is reported in both low‐ and high‐income countries [10]. In Ghana, where anemia is endemic and still a major “enemy” to public health due to factors such as nutritional deficiencies, parasitic, and chronic conditions, COVID‐19 may aggravate anemia burden among infected persons [6, 11].
Exposure to SARS‐CoV‐2 disrupts immune‐regulatory markers which predispose patients to coagulopathies and other severe complications. Among COVID‐19 patients, thrombocytopenia has been commonly reported, and this may arise from bone marrow suppression, amplified platelet consumption from disseminated intravascular coagulation, and immunologically‐driven platelet lysis. The SARS‐CoV‐2‐induced thrombocytopenia has been linked with poor prognosis and is prominently observed in critically ill COVID‐19 patients [12, 13, 14, 15]. Likewise, leucocyte abnormalities are generally reported in COVID‐19 and this indicates the dynamic immune response to the SARS‐CoV‐2. The initial phase of COVID‐19 may present with leucopenia or lymphopenia, while severe illness mostly results in leucocytosis, neutrophilia, and monocytosis, influenced by systemic inflammation [12, 16, 17, 18].
In addition, immune‐inflammatory ratios such as neutrophil‐to‐lymphocyte ratio (NLR), platelet‐to‐lymphocyte ratio (PLR), platelet‐to‐neutrophil ratio (PNR), and the systemic immune‐inflammation index (SII) have been recognized as surrogate markers for disease severity in COVID‐19. These indices, obtained from basic full blood count parameters, are easier to estimate and show insights into the equilibrium between inflammation and immune proficiency. The unique association between high inflammatory indices with enhanced risk of severe COVID‐19 and death have been recognized. The utility of the inflammatory indices in SARS‐CoV‐2 lies in their ability to recognize high‐risk patients quickly, even before the appearance of explicit clinical deterioration [19, 20, 21, 22, 23].
Regardless of the detected COVID‐19‐induced hematological abnormalities globally, there are few studies from sub‐Saharan Africa, particularly Ghana. Most studies on COVID‐19 in Ghana have prioritized epidemiology, vaccine uptake, and clinical presentations, with limited attention to laboratory and hematological parameters [3, 24]. Given the endemicity of other infections that autonomously alter hematological indices, such as malaria and HIV [6, 11], it is imperative to describe the exclusive hematological profile of COVID‐19 in this setting. Hence, this study assessed the hematological profile of SARS‐CoV‐2‐infected adults. Exploring these alterations is central for guiding suitable interventions, especially in under‐resourced setting where cutting‐edge diagnostic and monitoring techniques may not be readily accessible.
Materials and Methods
2
Study Participants
2.1
One hundred and sixty‐nine reverse transcriptase‐polymerase chain reaction (RT‐PCR)‐confirmed COVID‐19 adults were recruited for this cross‐sectional study at Sunyani Teaching Hospital between January and August, 2022. The teaching hospital is the main referral and treatment facility situated in the Bono Region, Ghana, and designated as a laboratory confirmation site and COVID‐19 case management center in the region. Sunyani is the administrative capital of the Bono Region and the municipality houses over 100,000 population [25]. The appropriate sample size was estimated using Cochran's formula at a 95% confidence level, 0.05 margin of error, and 13.2% prevalence of COVID‐19 in Ghana [24]. Patients with identified chronic hematological disorders, malignancies, chronic kidney or liver disease, and acute infections unrelated to COVID‐19 were excluded to lessen confounding effects on hematological parameters. Additionally, persons with incomplete clinical records were not enrolled. Participants' socio‐demographics (age, sex and place of residence), vital signs (temperature, blood pressure, pulse and oxygen saturation [SpO_2_]), and other clinical manifestations were retrieved from the medical records.
Sampling and Laboratory Assays
2.2
Nasopharyngeal swabs were obtained and mixed with virus transport medium for the diagnosis of COVID‐19 using RT‐PCR technique. The swabs were taken before initiating COVID‐19 medication. The clinical severity was described using the standards categorized by the World Health Organization. Mild/moderate COVID‐19 participants had no or lower evidence of pneumonia or hypoxia, while severe patients experienced respiratory frequency with SpO_2_ < 90% on room air or requires supplemental oxygen [26]. Three milliliters of blood was collected from the COVID‐19 patients for full blood count (Mindray BC3000 Plus, China). The following operational definitions of hematological abnormalities were considered [27, 28]:
-
Anemia: Hb < 13.0 g/dL in males (Mild anemia: 11.0–12.9 g/dL, Moderate anemia: 8.0–10.9 g/dL, Severe anemia: < 8.0 g/dL); and < 12.0 g/dL in females (Mild anemia: 11.0–11.9 g/dL, Moderate anemia: 8.0–10.9 g/dL, Severe anemia: < 8.0 g/dL)
-
Macrocytosis: MCV > 100 fL
-
Microcytosis: MCV < 80 fL
-
Hypochromasia: MCH < 27.0 pg
-
Thrombocytopenia: Platelet count < 150 × 10⁹/L (Mild thrombocytopenia: 101–149 × 10^9^/L, Moderate thrombocytopenia: 51–100 × 10^9^/L, Severe thrombocytopenia: ≤ 50 × 10^9^/L)
-
Leucopenia: WBC count < 4.0 × 10⁹/L
-
Leucocytosis: WBC count > 11.0 × 10^9^/L
-
Neutropenia: Absolute neutrophil count < 2.0 × 10⁹/L
-
Lymphocytosis: Absolute lymphocyte count > 4.0 × 10⁹/L
-
Bicytopenia: Reduction in any two of the three cell lines (RBC, WBC, Platelets)
-
Pancytopenia: Reduction in all three cell lines
-
Morphological forms of anemia were described using standard MCV and MCH cut‐offs:
-
◦Microcytic hypochromic: MCV < 80 fL and MCH < 27 pg
-
◦Normocytic normochromic: MCV 80–100 fL and MCH 27–33 pg
-
◦Macrocytic normochromic: MCV > 100 fL and MCH 27–33 pg
Both the COVID‐19 confirmation and full blood count tests were performed at the Clinical Laboratory of Sunyani Teaching Hospital.
Statistical Analysis
2.3
SPSS v.27.0 (Armonk, USA) was used for data analysis. Numerical data were expressed as mean ± SD or median (25^th^–75^th^ percentiles) and comparisons were made using independent samples T‐test or Mann–Whitney U‐test. Nominal variables were expressed as proportions and compared using χ ^2^ test or Fisher's exact test. The receiver operating characteristic (ROC) was performed to evaluate the predictive performance of systemic inflammatory markers for severe COVID‐19. Statistical significance was considered when p < 0.05.
Ethics and Informed Consent
2.4
All protocols were in line with the Declaration of Helsinki. Ethical clearance was obtained from the Committee on Human Research, Publication and Ethics of Kwame Nkrumah University of Science and Technology, Kumasi, (CHRPE/AP/012/22). Participants provided written informed consent to be part of this study.
Results
3
Age, Sex and Residence of the Participants
3.1
This study comprised 169 SARS‐CoV‐2‐infected adults aged 20–81 years with a median age of 35.0 (29.0–47.0) years. About 54% were females, and participants were mostly young adults (51.5%), and resided in an urban setting (41.4%) (Table 1).
Clinical Manifestations of the Participants
3.2
The clinical manifestations experienced by the SARS‐CoV‐2 patients included headache (39.6%), cough (61.5%), nausea (26.0%), loss of smell (56.2%), loss of taste (57.4%), fatigue (51.5%), and fever (59.8%). Almost one‐third of the 269 participants had severe COVID‐19 and required immediate care. Averagely, the participants had moderately increased temperature (37.6°C ± 1.3°C), systolic blood pressure (132.0 [123.0–147.0] mmHg) and diastolic blood pressure (81.0 [72.0–88.0] mmHg). While participants' SpO2 was at a borderline (94.0 [90.0–97.0] %), their pulse rate was normal 90.0 [84.0–97.0] bpm) (Table 2).
Blood Cell Parameters of COVID‐19 Patients
3.3
Overall, the COVID‐19 adults were mildly anemic (Hb = 11.1 ± 2.4 g/dL) and thrombocytopenic (platelet count = 132.0 [105.4–182.9] × 109/L), but leucocyte count was within the normal range. Red blood cells, Hb, and HCT were lower in SARS‐CoV‐2‐infected females than their male counterparts. Platelet and leucocyte parameters, and systemic inflammatory ratios (NLR, PLR, PNR, and SII) were comparable between male and female COVID‐19 patients (Table 3).
Age, Vital Signs and Blood Cell Parameters Based on COVID‐19 Severity
3.4
The severe COVID‐19 adults were relatively older than those in the mild/moderate group. With the exception of diastolic blood pressure which was similar between the two groups, adults with severe COVID‐19 had elevated axillary temperature, SBP, and pulse rate than the mild/moderate COVID‐19 adults. On the contrary, severe COVID‐19 patients had lower SpO_2_ (p < 0.001) compared to the mild/moderate adults.
RBC count, hemoglobin, hematocrit, and platelet count were lower in the severe than mild/moderate COVID‐19 patients. Adults with severe COVID‐19 had lower red cell indices (MCV and MCH), but higher red cell distribution‐width than the mild/moderate group. Leucocyte parameters: white blood cell count, absolute neutrophil count, absolute lymphocyte count, and MID (monocytes, eosinophils and basophils) were elevated in patients with severe COVID‐19 than those with mild/moderate disease. Also, systemic inflammatory ratios: NLR, PLR, PNR, and SII were elevated among the severely ill adults than the mildly/moderately ill COVID‐19 patients (Table 4).
Blood Cell Abnormalities of COVID‐19 Patients
3.5
Anemia was present in about two‐third of the COVID‐19 patients, and mild, moderate and severe anemia occurred among 40 (23.7%), 40 (23.7%), and 22 (13.0%), respectively among the participants. The prevalence of anemia in males was 56.4%, whereas 63.7% of the female participants were anemic. In males, 24.4%, 24.4%, and 7.7% had mild, moderate and severe anemia, and the proportion of females with mild, moderate and severe were 23.1%, 23.1%, and 17.6%, respectively. Other erythrocyte abnormalities identified among COVID‐19 adults were macrocytosis (37.9%), microcytosis (7.7%), and hypochromasia (7.7%). Red blood cell distribution width was high in 52.1%, but decreased in 11.2% of the participants. With regards to the forms of anemia, normocytic normochromic anemia was the most dominant (50.3%) found among the COVID‐19 patients, followed by macrocytic normochromic anemia (37.9%). Only few of the COVID‐19 patients had microcytic normochromic (4.1%), normochromic hypochromic (4.1%), and microcytic hypochromic anemia (3.6%). About 60% of the COVID‐19 patients had normal white blood cell count, while 22.5% and 17.2% presented with leucopenia and leucocytosis, respectively. Neutropenia was present in 40.8% of the participants, and 39.6% had lymphocytosis. Moreover, 56.2% of the COVID‐19 patients were thrombocytopenic, and the proportion of participants with mild, moderate and severe thrombocytopenia found were 36.7%, 16.0%, and 2.4%, respectively. Platelet microcytosis was seen in about one‐third of the COVID‐19 adults, and 14.8% had low platelet distribution width. About one‐fifth of the participants had normal blood cells, and single cell abnormality, bicytopenia and pancytopenia was observed in 27.2%, 37.3%, and 17.8%, respectively (Table 5).
Relationship Between Socio‐Demographics and Anemia Severity Among the COVID‐19 Patients
3.6
Severe anemia was more common among the older (68.8%) and middle‐aged (30.8%) adults than the adolescents and the young adults with COVID‐19. There was an association between anemia severity, and participants' ages and residence. Older adults with COVID‐19 were 6.600 times (p = 0.004), and middle‐aged adults were 4.435 times (p = 0.034) more likely to experience severe anemia than the adolescents. Again, the chances of participants who resided in rural settings were 3.759 times (p = 0.012) higher than those living in the urban areas in getting anemia (Table 6).
ROC Analysis to Predict the Diagnostic Performance of Immune‐Inflammatory Markers for Severe COVID‐19
3.7
Total leucocyte count (AUC: 0.818, p < 0.001), absolute neutrophil count (AUC: 0.816, p < 0.001), and absolute lymphocyte count (AUC: 0.804, p < 0.001) were good predictors of severe COVID‐19 among the participants. Other immune‐inflammatory markers were poorly associated with severe COVID‐19 in adults (Figure 1).
ROC analysis to predict the diagnostic performance of immune‐inflammatory markers for severe COVID‐19.
Discussion
4
The advent of COVID‐19 has changed public health landscapes worldwide, with its consequences principally felt in developing countries including Ghana, where healthcare resources are limited [1]. SARS‐CoV‐2 mainly colonizes the respiratory system; however, the virus interacts with other organs through ACE‐2 causing systemic damages and disrupting physiological processes including hemopoietic activities [4, 5, 6]. In this study, we profiled hematological abnormalities associated with SARS‐CoV‐2‐infected adults.
The COVID‐19‐infected patients included in this study were mostly young adults between 25 and 40 years, and had median age of 35.0 (29.0–47.0) years. This age group represents an energetic period in life where people actively engage in several activities, work assiduously to meet the needs of themselves and their associates. This adventure increases chances of such youthful adults of being exposed to SARS‐CoV‐2 as the virus is transmitted through respiratory droplets and aerosols during close contact with infected persons. The observation of high risk of young adults' exposure to COVID‐19 observed in this study is similar to findings from previous studies [29, 30, 31]. Ghanaian women interact more at well‐populated places such as market areas, funeral grounds and other social gatherings than men. This makes females a social conduit to facilitate the communication of SARS‐CoV‐2 among themselves, and accounts for the higher proportion of COVID‐19 detected among females than males in this study, as has been observed in other jurisdictions [8, 24, 32]. Other studies posit that males are more susceptible to COVID‐19 and its related severity and deaths due to the existence of excessive amount of ACE‐2 and transmembrane serine protease‐2 which facilitate disease progression [33, 34]. This study reports a higher proportion of SARS‐CoV‐2 infection among inhabitants living in urban settings than those in rural or peri‐urban areas, and this agrees with earlier concept [35]. Environmental factors such as high population density, crowded living and public spaces, greater mobility and travel, increased person‐to‐person contact, and higher exposure in congested hospitals may account for the observation of higher occurrence of COVID‐19 in urban settings.
Fever, cough, fatigue, headache, nausea, and loss of smell and taste were frequently reported symptoms among COVID‐19‐infected adults in this study. These findings corroborate other observations from earlier studies [4, 5, 33], and this highlights the diverse clinical manifestations of the disease. The presence of fever in 59.8% of patients coupled with the relative increase in body temperature in patients with severe COVID‐19 emphasizes the hyperinflammatory nature of SARS‐CoV‐2 infection, with the systemic release of inflammatory cytokines such as interferon gamma, IL‐1, IL‐6, and TNF‐α contributing extensively to fever pathogenesis [9, 31, 33]. Severe COVID‐19 patients experienced high systolic blood pressure and pulse rate, but lower oxygen saturation than adults with mild‐to‐moderate infection in this study. The decreased SpO_2_ could arise from the related enhanced lung damage and respiratory failure‐related hypoxia, whereas the direct effects of SARS‐CoV‐2 on renin‐angiotensin‐aldosterone system explains the elevated blood pressure in the patients [36, 37].
Anemia was the most common blood cell abnormality detected among the SARS‐CoV‐2 patients in this study, occurring in 60.4% of the patients. The anemia ranged from mild to severe, with a greater burden found among adults with severe COVID‐19 infection. The magnitude of anemia observed in SARS‐CoV‐2‐infected adults indicates the systemic involvement of the virus, which potentially suppresses erythropoiesis either directly via bone marrow suppression or indirectly through impaired nutrients metabolism, chronic inflammation, and renal dysfunction. Similar findings have been reported in previous studies in Ghana [6, 11, 12], and other settings [7, 8, 9]. The substantial relationship between anemia and adverse complications in COVID‐19 infection, including increased hospitalization, oxygen need, and mortality is reported in both developing and high‐income countries [10]. The prevalence of anemia was disproportionally higher in females than in males with COVID‐19, and this may be due to the positive androgenic effects on erythropoiesis which favors males and the periodic menstrual flow of females especially for those who had borderline hemoglobin prior to exposure to SARS‐CoV‐2 [8, 38]. Severe anemia was more common among the older (68.8%) and middle‐aged (30.8%) adults than the adolescents and the young adults with COVID‐19, which is similar to earlier reports [38, 39]. Also, older adults with COVID‐19 were 6.600 times, and middle‐aged adults were 4.435 times more likely to experience severe anemia than the adolescents. The higher susceptibility of the aged to anemia could be explained by the fact that with ageing only few bone marrows are hemopoietically active and more than half of such active bone marrows are occupied by fat, coupled with a significant drop of androgen especially in males after four decades in life and this has negative effect on blood cell production. Other probable etiology of anemia at older age could arise from bone marrow failure syndromes, presence of chronic kidney disease, and nutritional deficits [38, 40]. Similarly, COVID‐19 adults who resided in rural settings were 3.759 times higher than those living in the urban areas to experience anemia. This may be attributed to pre‐existing comorbidities and reduced access to healthcare. This finding suggests the need for targeted screening and intervention measures for susceptible populations, particularly in areas with limited diagnostic capacity.
The dominant forms of anemia in this study were normocytic normochromic and macrocytic normochromic; a distribution that reflects the multifactorial pathogenesis of COVID‐19‐associated anemia. Normocytic normochromic anemia is characteristically related to chronic inflammatory states, where cytokine‐triggered retardation of erythropoietin release and iron‐restricted erythropoiesis lead to reduced erythrocyte production but do not affect red cell sizes and hemoglobinization [39, 41]. On the contrary, macrocytosis may indicate impaired DNA synthesis in erythroblats, probably due to nutritional deficits, medications, or direct viral attack to the bone marrow [42, 43]. This spectrum of anemia forms highlight the relevance of a comprehensive diagnostic approach, mainly in settings where iron, folate, and B_12_ deficiencies are common.
In addition to anemia, a substantial proportion of COVID‐19 patients presented with thrombocytopenia (56.2%), largely of mild‐to‐moderate severity in this study. Thrombocytopenia in SARS‐CoV‐2 infection is multifactorial, involving direct immune‐mediated destruction of platelets, enhanced peripheral consumption in microthrombi, bone marrow suppression, and increased splenic sequestration [12, 13, 14, 15]. Platelet abnormalities, including microcytosis and altered platelet distribution width, were also found, suggesting compensatory marrow responses or disturbed megakaryopoiesis. These platelet abnormalities have been connected with poor outcomes in COVID‐19, and could serve as vital biomarkers for monitoring disease progression [13, 14]. Interestingly, while leucocytes count remained within normal for most COVID‐19 patients, specific leucocyte abnormalities were detected in this study. This study observed leucopenia and leucocytosis in 22.5% and 17.2% of the patients, respectively, demonstrating differing immune responses probably influenced by SARS‐CoV‐2 viral load, disease duration, and host factors. Neutropenia was observed in 40.8% of patients, while 39.6% demonstrated lymphocytosis among COVID‐19 adults. These findings are consistent with previous studies, where lymphocytosis was found in COVID‐19 patients with prolonged or severe infection, possibly indicating a delayed but overwhelmed adaptive immune response. Also, neutropenia, on the other hand, may occur through peripheral neutrophils consumption or bone marrow suppression due to the impact of inflammatory cytokines or direct SARS‐CoV‐2 invasion [16, 17, 18].
Systemic inflammatory ratios such as NLR, PLR, PNR, and SII were noticeably high in severe COVID‐19 patients in this study. These indices serve as surrogate markers of immune dysregulation and have been linked with worse clinical outcomes in various viral infections, including COVID‐19 [19, 20]. Although the predictive performance of these systemic inflammatory indices for severe COVID‐19 was poor in this study, this may be due to the population‐specific variances in immune response.
Surprisingly, only about one‐fourth of the COVID‐19 patients had normal blood cell parameters, and the rest exhibited either single‐cell abnormality, bicytopenia, or pancytopenia. The detection of bicytopenia (37.3%) and pancytopenia (17.8%) accentuates the systemic nature of COVID‐19 infection, which can affect multiple hemopoietic lineages. Pancytopenia has been associated with cytokine‐induced bone marrow dysfunction, viral tropism for hemopoietic progenitor cells, and consumptive coagulopathy—all of which can thwart clinical management and facilitate mortality risk [44].
Strength and Limitations
4.1
This study offers essential data on hematological abnormalities among adult COVID‐19 patients in Ghana. However, this study has some limitations. First, the cross‐sectional design restricts causal inference. Second, the study did not include healthy controls, preventing comparison with uninfected individuals. Third, the nutritional status of the participants was not evaluated. Lastly, participants were not screened for parasitic infections such as malaria and helminths. Regardless of these limitations, the study pinpoints vital hematological patterns that may support clinical management of COVID‐19.
Conclusion
5
Adults infected with SARS‐CoV‐2 experience diverse and clinically important hematological abnormalities. Anemia, thrombocytopenia, and leucocyte alterations are predominantly observed in COVID‐19, and often associate with disease severity. Increased inflammatory indices and multiple cytopenias are especially common in severely ill patients. Routine blood cell analysis is essential in the management of COVID‐19, particularly in resource‐limited settings. Future studies should investigate the longitudinal changes in hematological parameters and their relationship with COVID‐19 outcomes in different geographical areas and populations.
Author Contributions
Charles Nkansah: conceptualization, investigation, writing – original draft, writing – review and editing, methodology, visualization, formal analysis, data curation, resources. Felix Osei‐Boakye: writing – original draft, writing – review and editing, visualization, formal analysis, methodology. Samuel K. Appiah: investigation, writing – original draft, writing – review and editing, methodology, data curation.
Funding
The authors received no specific funding for this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
STROBE Statement—checklist of items that should be included in reports of observational studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. Dhama , S. Khan , R. Tiwari , et al., “Coronavirus Disease 2019‐COVID‐19,” Clinical Microbiology Reviews 33 (2020): e 00028‐20, 10.1128/CMR.00028-20.32580969 PMC 7405836 · doi ↗ · pubmed ↗
- 2W.H.O . WHO COVID‐19 dashboard. 2025.
- 3E. Kenu , J. Frimpong , and K. Koram , “Responding to the COVID‐19 Pandemic in Ghana,” Ghana Medical Journal 54 (2020): 72–73, 10.4314/gmj.v 54i 2.1.33536675 PMC 7829051 · doi ↗ · pubmed ↗
- 4C. B. Beggs , R. Abid , F. Motallebi , A. Samad , N. Venkatesan , and E. J. Avital , “Airborne Transmission of SARS‐Co V‐2: The Contrast Between Indoors and Outdoors,” Fluids 9 (2024): 54, 10.3390/fluids 9030054. · doi ↗
- 5P. Bhadoria and H. Rathore , “Multi‐Organ System Dysfunction in Covid‐19—A Review,” Journal of Evolution of Medical and Dental Sciences 10 (2021): 632–637, 10.14260/jemds/2021/135. · doi ↗
- 6E. B. Ackah , M. Owusu , B. Sackey , et al., “Hematological Profile and ACE 2 Levels of COVID‐19 Patients in a Metropolis in Ghana,” COVID 4 (2024): 117–129, 10.3390/covid 4020011. · doi ↗
- 7J. L. Benoit , S. W. Benoit , M. H. S. de Oliveira , G. Lippi , and B. M. Henry , “Anemia and COVID‐19: A Prospective Perspective,” Journal of Medical Virology 93 (2021): 708–711, 10.1002/jmv.26530.32949170 PMC 7536957 · doi ↗ · pubmed ↗
- 8G. Bergamaschi , F. Borrelli de Andreis , N. Aronico , et al., “Anemia in Patients With Covid‐19: Pathogenesis and Clinical Significance,” Clinical and Experimental Medicine 21 (2021): 239–246, 10.1007/s 10238-020-00679-4.33417082 PMC 7790728 · doi ↗ · pubmed ↗