Occult Endobronchial Foreign Body Presenting as Persistent Lobar Collapse and Severe Pneumonia
Venkatkiran Kanchustambham

TL;DR
A rare case of an adult with persistent lung collapse and pneumonia was caused by an undetected foreign object in the airway.
Contribution
Highlights the importance of considering foreign body aspiration in adults with unexplained lung conditions.
Findings
An occult endobronchial foreign body was identified as the cause of persistent lobar collapse and severe pneumonia.
The case emphasizes the need for bronchoscopy in diagnosing non-resolving lung conditions in adults.
Abstract
Foreign body aspiration is uncommon in adults and may present without a clear aspiration history. We describe an adult patient with persistent lobar collapse and severe pneumonia in whom bronchoscopy revealed an occult endobronchial foreign body causing airway obstruction. An adult patient with persistent lobar collapse and severe pneumonia was found to have an occult endobronchial foreign body on bronchoscopy. This case highlights the importance of considering foreign body aspiration in adults with non‐resolving pneumonia or unexplained lobar collapse.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1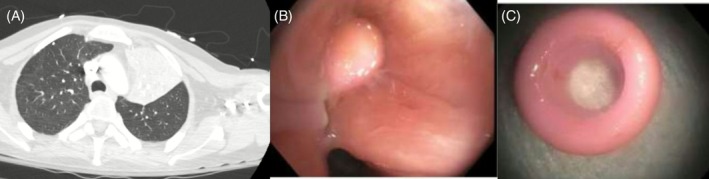 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Traumatic Ocular and Foreign Body Injuries · Trauma Management and Diagnosis
A 50‐year‐old man with intellectual disability, autism spectrum disorder, epilepsy, hypothyroidism and diabetes mellitus presented with altered mental status and severe pneumonia. Chest computed tomography (CT) demonstrated complete left upper lobe collapse with an abrupt cutoff of the left upper lobe bronchus, raising concern for an obstructing endobronchial lesion (Figure 1A). Despite appropriate antibiotic therapy, the patient showed minimal clinical improvement.
Flexible bronchoscopy revealed an impacted endobronchial foreign body completely obstructing the left upper lobe bronchus, with surrounding mucosal inflammation and friability (Figure 1B,C). The foreign material was successfully removed bronchoscopically, resulting in immediate restoration of airway patency and subsequent clinical and radiographic improvement. No active bleeding was identified during bronchoscopy.
Foreign body aspiration in adults is uncommon and frequently occurs without a witnessed aspiration event, particularly in patients with neurologic or cognitive impairment [1]. Persistent lobar collapse or non‐resolving pneumonia should prompt evaluation for endobronchial obstruction even in the absence of choking history. Early bronchoscopy is both diagnostic and therapeutic and can prevent recurrent infection and long‐term pulmonary complications [2].
Author Contributions
Venkatkiran Kanchustambham was responsible for patient care, image selection, literature review and manuscript preparation.
Funding
The author has nothing to report.
Consent
The author declares that written informed consent was obtained for the publication of this manuscript and accompanying images using a consent form that complies with the Journal's requirements as outlined in the author guidelines.
Conflicts of Interest
The author declares no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. H. Limper and U. B. S. Prakash , “Tracheobronchial Foreign Bodies in Adults,” Annals of Internal Medicine 112 (1990): 604–609.2327678 10.7326/0003-4819-112-8-604 · doi ↗ · pubmed ↗
- 2M. Blanco Ramos , M. Botana‐Rial , E. García‐Fontán , A. Fernández‐Villar , and M. Gallas Torreira , “Update in the Extraction of Airway Foreign Bodies in Adults,” Journal of Thoracic Disease 8 (2016): 3452–3456.28066626 10.21037/jtd.2016.11.32PMC 5179474 · doi ↗ · pubmed ↗