Palliative Osimertinib Rechallenge Achieving Rapid Improvement in Leptomeningeal Carcinomatosis After Prior Osimertinib‐Induced ILD
Akina Nigi, Keisuke Iwamoto, Hidetoshi Itani, Shigeto Kondou

TL;DR
A patient with lung cancer showed rapid improvement after being treated again with osimertinib, despite a prior allergic reaction.
Contribution
Demonstrates successful osimertinib rechallenge for leptomeningeal carcinomatosis after prior drug-induced lung injury.
Findings
Osimertinib rechallenge led to neurological improvement and radiological response.
No recurrence of osimertinib-induced ILD was observed during rechallenge.
The case suggests potential for reusing EGFR inhibitors in exceptional clinical scenarios.
Abstract
A patient with EGFR‐mutant lung cancer developed leptomeningeal carcinomatosis years after osimertinib‐induced ILD. With no other treatment options, palliative osimertinib rechallenge led to rapid neurological improvement and radiological response, without ILD recurrence. This case highlights the potential of carefully monitored osimertinib rechallenge for symptomatic relief in exceptional cases. This case highlights the potential of carefully monitored osimertinib rechallenge for symptomatic relief in exceptional cases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
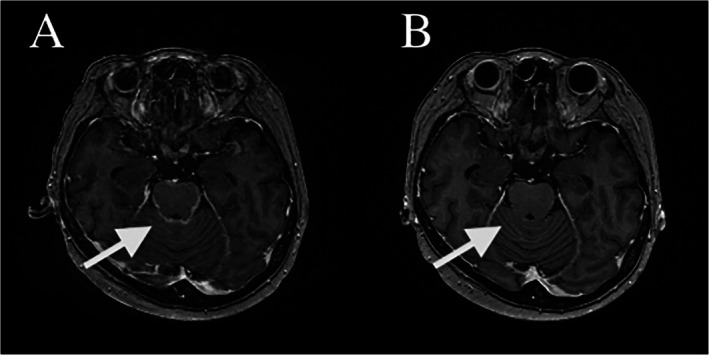 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Brain Metastases and Treatment · Management of metastatic bone disease
A 60‐year‐old woman with stage IVB EGFR‐mutated lung adenocarcinoma and prior brain metastases was initially treated with osimertinib but discontinued therapy after developing CTCAE grade 2 interstitial lung disease (ILD). She subsequently received carboplatin, pemetrexed and bevacizumab, followed by maintenance erlotinib without further ILD. Four and a half years later, she developed multiple brain metastases and cauda equina metastasis, which were treated with radiotherapy; however, neurological symptoms progressed, and MRI later demonstrated advancement to leptomeningeal carcinomatosis (LMC) (Figure 1A). Despite four cycles of docetaxel plus ramucirumab, her dysphagia, dysarthria and gait disturbance worsened.
Although rechallenge with the same class of EGFR‐TKI is generally avoided after ILD, the patient elected palliative re‐introduction of osimertinib. Neurological improvement was observed within 1 week. Follow‐up MRI 14 days after rechallenge showed marked radiologic improvement of LMC (Figure 1B), while parenchymal brain metastases remained unchanged.
Erlotinib efficacy had diminished before progression, yet the superior cerebrospinal fluid penetrance of osimertinib compared with erlotinib may explain the observed clinical response [1]. No ILD recurrence was noted 2 months after restarting therapy.
This case suggests that, in selected patients with rapidly progressive LMC and limited options, carefully considered palliative osimertinib rechallenge may provide meaningful symptomatic and radiologic benefit despite prior EGFR‐TKI–induced ILD.
Funding
The authors have nothing to report.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Park , R. Baldry , H. A. Jung , et al., “Phase II Efficacy and Safety of 80 mg Osimertinib in Patients With Leptomeningeal Metastases Associated With Epidermal Growth Factor Receptor Mutation‐Positive Non‐Small Cell Lung Cancer (BLOSSOM),” Journal of Clinical Oncology 42, no. 23 (2024): 2747–2756, 10.1200/JCO.24.00708.38828959 PMC 11315406 · doi ↗ · pubmed ↗