Inter-clinician diagnostic agreement of shock etiology: a multicenter observational study
Lauren M. Janczewski, Carolyn J. Hu, Tiannan Zhan, Ravi Garg, John Slocum, Al’ona Furmanchuk, Andrew Berry, Nandita Nadig, Jeff Huml, Laeeq Shamshuddin, Yuriy Moklyak, Laura J. Davidson, Sherry Chou, Abbas AlQamari, Emilie Powell, Bruce Ankenman, Jane L. Holl, Anne Stey

TL;DR
This study found that clinicians often disagree on the cause of shock in ICU patients, and machine learning can predict these disagreements.
Contribution
The study introduces a novel method to quantify diagnostic disagreement using cosine similarity and machine learning prediction models.
Findings
18.2% of patients had no complete inter-clinician diagnostic agreement for shock etiology.
Machine learning models achieved high accuracy in predicting patients with diagnostic disagreement.
Patients without agreement had higher mortality and fewer comorbidities.
Abstract
We sought to (1) quantify lack of inter-clinician diagnostic agreement of shock etiology and (2) predict patients without complete inter-clinician diagnostic agreement of shock etiology. This multicenter retrospective, cohort study identified patients evaluated by two or more clinicians who documented a shock diagnosis from 2018 to 2023 across intensive care units (ICU) at 9 acute care hospitals. Shock etiology was abstracted using regular expression from clinician notes in the electronic health record then was made into a 9-dimensional vector representing 9 different shock etiologies. Inter-clinician diagnostic agreement of these vectors was calculated for each patient using Cosine Similarity Scores. Measure of agreement was based on cosine similarity of etiology vectors, not clinical adjudication. Patients without complete inter-clinician diagnostic agreement (Cosine Similarity Score…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
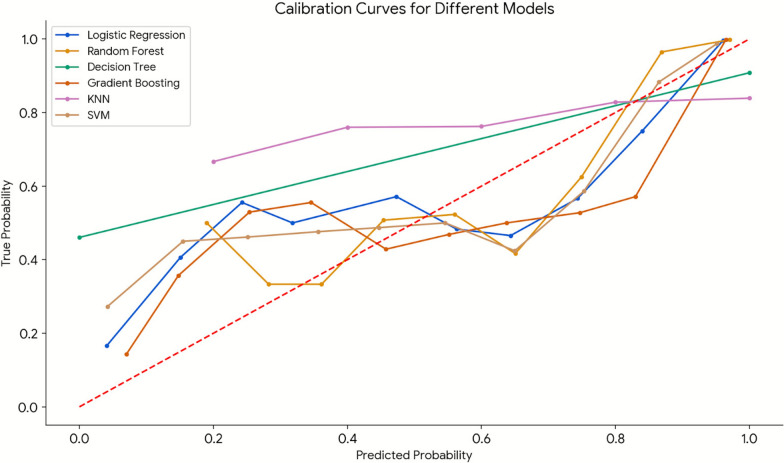 Figure 1
Figure 1- —http://dx.doi.org/10.13039/100000133Agency for Healthcare Research and Quality
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Clinical Reasoning and Diagnostic Skills · Patient Safety and Medication Errors
Introduction
Shock is a prevalent, lethal condition triggering the hospitalization of 1.3 million patients annually in the United States [1]. The underlying cause, or shock etiology is never identified in an estimated 70,000 cases annually [2]. Patient diagnosis commonly requires input from many clinicians of different disciplines to determine the primary shock etiology and best treatment plan [3, 4]. Mortality rates range between 30 and 50% and depend largely on the shock etiology diagnosis as well as treatment timeliness [2, 3, 5–7]. Shock is one of the costliest conditions to treat costing 68,000 per admission [8].
Prior research has focused on identifying whether shock was present [1], especially for common specific shock etiologies, such as septic shock. There is little literature on establishing the underlying shock etiology diagnosis. Many clinicians are involved in the diagnosis and treatment of shock. Inter-clinician diagnostic agreement may help drive more timely treatment, and lower mortality [9]. The rate of inter-clinician diagnostic agreement of shock etiology, and whether patients without inter-clinician diagnostic agreement of shock etiology can be predicted have not been studied.
The study objective was to characterize inter-clinician diagnostic agreement of shock etiology. The first aim sought to quantify the frequency of patients without inter-clinician diagnostic agreement of shock etiology. The second aim was to build a machine learning model to predict which patients would not have inter-clinician diagnostic agreement of shock etiology. We hypothesized that patients without inter-clinician diagnostic agreement would experience higher in-hospital mortality, and that machine learning models could successfully predict which patients would not have complete inter-clinician diagnostic agreement of shock etiology.
Methods
Study design and setting
This multicenter observational, retrospective, cohort study identified patients with shock between January 1st, 2018, and December 31st, 2023, within an integrated academic urban healthcare system located in the Midwestern United States comprised of 9 acute care hospitals. These hospitals included one academic medical center, seven community hospitals, and one critical access hospital. This study was approved by the Northwestern University Institutional Review Board under study number STU00218401. The transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) reporting guidelines was followed. All procedures were followed in accordance with the Helsinki Declaration of 1975.
Data source
Electronic Health Record (EHR) structured and unstructured data were obtained from the healthcare system Enterprise Data Warehouse (EDW). The systemwide integrated EDW captured all inpatient encounters across all hospitals in the healthcare system from 2018 until 2023. This data source has been used to successfully identify the presence of shock as well as the shock phenotype among injured patients in a variety of geographic context (urban, suburban and rural) and hospital settings (academic medical center, community hospitals and critical access hospitals) [10].
Study population
Eligibility criteria were adult patients greater than or equal to 18 years of age, hospitalized in an intensive care unit (ICU) at any one of the 9 acute care hospitals between 2018 and 2023 with shock. Shock was defined using both structured (vitals and labs) and unstructured (notes) data. Shock patient encounters were first identified with structured data, specifically a systolic blood pressure measurement of less than 90 mmHg, AND with at least one new organ failure as measured by a new elevation in the Sequential Organ Failure Assessment (SOFA) score from the last recorded measurement [11, 12]. Among these patient encounters, the shock cohort was further narrowed to include only patient encounters with “shock” documented in history and physical, progress, or consult notes using regular expression from the same day (day 0) as systolic blood pressure measurement of less than 90 mmHg and new elevation in the SOFA score. Patient encounters with notes only using negation terms were excluded. Patient encounters with less than two clinician notes documenting “shock” were excluded (eFig. 1) as two or more notes on any one day were needed to determine inter-clinician diagnostic agreement.
Shock etiology diagnosis
Shock etiology diagnosis was a priori collapsed into nine different shock etiologies Septic, Cardiogenic, Hypovolemic, Adrenal, Neurogenic, Undifferentiated, Obstructive, Anaphylactic, Post-procedural) based on clinical experience and prior literature.[13] Regular expressions were applied to all unstructured data documented in clinician history and physical, progress, or consult notes from the first day of the systolic blood pressure measurement of less than 90 mmHg and new elevation in the SOFA score (called day 0) through day four. A daily clinician-specific shock etiology diagnosis variable was created for each clinician note [14]. Septic shock was identified by presence of the string value “Sepsis”, “Septic”, and “Septic Shock” without negation statements. Cardiogenic shock was identified by presence of the string value “Cardiac Shock”, “Cardiogenic”, “Cardiogenic Shock” without negation statement. Hypovolemic shock was identified by presence of the string value “hypovolemic”, “hypovolemia”, “hypovolemic shock”, “hemorrhage”, “hemorrhagic shock” and “traumatic shock” without negation statement. Adrenal shock was identified by presence of the string value “adrenal shock”, and “adrenal insufficiency” without negation statement. Neurogenic shock was identified by presence of the string value “spinal shock”, and “neurogenic shock” without negation statement. Undifferentiated shock was identified by the presence of the string value “undifferentiated shock”, “shock NOS”, and “multifactorial shock” without negation statement. Obstructive shock was identified by presence of the string value “obstructive shock”, “cardiac tamponade”, “tamponade”, “tension pneumothorax” and “tension pneumo” without negation statement. Anaphylactic shock was identified by the presence of the string value “anaphylaxis”, “anaphylactic” and “anaphylactic shock” without negation statement. Post-procedural shock was identified by presence of the string value “post-procedure shock”, and “post-procedural shock” without negation statement. Shock etiology diagnosis was abstracted from each clinician note in the electronic health record, for each patient, on each day 0 through day 4. We manually reviewed all occurrences to identify if ambiguous or overlapping terms were present. “Undifferentiated Shock” was the ambiguous term most frequently used, and we created a separate vector (of the nine) labeled as such. Overlapping terms, such as the different shock diagnoses, in the same note or by the same clinician in a later note each day were treated as discrete observations generating an additional vector for each separate shock diagnosis. Additionally, we manually reviewed all observations and ensured that context-sensitive language was not playing any role here. A total of 395 patients were reviewed with ambiguous phrases adjudicated by two clinicians (LJ, AMS). Ambiguous or mixed phrases (e.g., “distributive shock,” “shock of unclear etiology”) were mapped onto the unknown category. When two different forms of shock were hypothesized then (e.g., “mixed septic and cardiogenic shock,”), the clinician note was annotated for both Septic and Cardiogenic shock.
Outcome of interest
The primary outcome of interest was inter-clinician diagnostic agreement of shock etiology diagnosis. Each clinician note, each dayfor each patient was interpreted as a nine-dimensional vector of binary values (i.e., 0 = not mentioned, 1 = mentioned) indicating mention of each of the nine shock etiologies above. Each clinicians’ daily diagnosis documented in their notes were compared to every other clinician’s daily diagnosis from days 0 to 4. The agreement between the clinicians’ shock etiology diagnoses was quantified using cosine similarity scores for nine-dimensional vectors from days 0 to 4. Cosine similarly measures the alignment of two vectors, with scores ranging from 0 to 1; a score of 1 indicates complete alignment, representing complete inter-clinician diagnostic agreement [15]. Patients were categorized based on whether they ever achieved a daily average cosine similarity score of 1 during the first four days of shock. Two near-perfect cosign similarity scores thresholds (≥ 0.95; ≥ 0.90) were also tested in sensitivity analyses. The measure of agreement was based on cosine similarity of etiology vectors, not on direct clinical adjudication. This study sought to understand the patient and clinician characteristics associated with not having complete inter-clinician diagnostic agreement of shock etiology, and to evaluate the ability of machine learning methods to predict which patients would never achieve inter-clinician agreement.
Independent variables
Independent variables were patient demographics, clinical factors, clinical course, and clinician characteristics. Patient demographics included age in years which was categorized into five groups, 50 and under, 51–60, 61–70, 71–80 and 81 and older. Sex was categorized as male and female. Race was categorized into seven groups as White, Black/African American, Asian, Native Hawaiian/Pacific Islander, American Indian/Alaska Native, Other and Unknown. Ethnicity was categorized into three groups as Hispanic, not Hispanic, and Unknown. Insurance was categorized into four groups as Medicare, Medicaid, Private and Self-pay. Area deprivation index (ADI) rank was calculated based on the patients address [16]. A larger number suggested patient lived in a neighborhood with greater socioeconomic deprivation. The ADI rank at the state was categorized into four groups as 1–2, 3–5, 6–10 and unknown, as well as categorized by the national rank into five groups as < 25, 25–49, 50–74, 75–100 and unknown.
Clinical features were SOFA score, Sepsis Score, Shock Index, shock etiology, Elixhauser comorbidity index, and Body Mass Index. Contextual clinical features were whether the first shock diagnosis occurred during the weekday or weekend, whether the ICU admission was on the weekday or weekend, and number of unique clinicians who wrote a note on the patient in the first 4 days of shock. The first recorded SOFA score was calculated from laboratory and clinical data for each patient upon shock presentation and was categorized into five groups as 0–6, 7–12, 13–15, 16–24, no SOFA score [17]. The sepsis score was categorized into six groups as 0, 1, 2, 3, > = 4, not applicable [18]. The shock index was calculated by dividing heart rate by systolic blood pressure then categorized in five groups as < 0.5, 0.5–0.7, 0.7–1.0, > 1.0, unknown [19]. The nine shock etiologies were described above. Elixhauser comorbidity index was calculated from the International Classification of Disease Codes and categorized into four groups: 0–5, 5–6, 7–10 and > 10. Body mass index (BMI) was calculated as weight (kg) divided by height (m^2^) and categorized into six groups: < 18.5, 18.5–24.9, 25.0–29.9, 30.0–34.9, ≥ 35, and unknown. ICU admission day and first diagnosis of shock day were each categorized as weekday or weekend. The daily note count, and unique clinician count per patient were calculated and treated as continuous variables.
Clinical course characteristics were SOFA score changes, treatments administered, ICU mortality and discharge disposition. SOFA score change was calculated as the difference between day 0 and day 4 then was categorized into four groups: improved, no change/worse, no SOFA score, and only one value recorded. Treatments included time to first intravenous bolus fluids (normal saline, lactated ringers or plasmalyte) and was categorized as < 24, 24–48, 49–72, 73–96, and > 96 h. The administration of intravenous fluids was recorded dichotomously by the day of shock presentation (days 0–4). Antifungal administration (micafungin, fluconazole, amphotericin) was categorzied as a dichotomous variable. Time to first antibiotics (eTable 1) was categorized similarly to intravenous fluids. Anticoagulation infusions (heparin, bivalirudin, argatroban) and diuretics (furosemide, bumetanide) were categorized dichotomously. Time to first lab draw, echocardiogram, and surgical procedure were categorized into six group variable: < 24, 24–48, 49–72, 73–96, and > 96 h. Procedures such as arterial line placement, cardiac catheterization, central venous catheter placement, and continuous renal replacement therapy were recorded as dichotomous variable . ICU mortality was a dichotomous outcome Discharge disposition was categorized as transfer to another acute care hospital, acute inpatient rehabilitation, long-term care facility, home, death, or unknown. Clinician characteristics included clinician type (e.g., physician, advanced practice provider) and specialty (e.g., cardiology).
Statistical analysis
The rate of patients which never had complete inter-clinician diagnostic agreement on any of the four days was calculated. Differences in patient demographics, clinical features, and clinical course between patients with complete inter-clinician diagnostic agreement and without were compared using chi-squared tests of independence. Clinician characteristics were compared between notes with and without complete diagnostic agreement using chi-squared tests, with statistical significance set at p-value < 0.05. Unadjusted analyses were performed in R version 4.3.0.
Machine learning models were developed to predict patients without complete inter-clinician diagnostic agreement on shock etiology. Data were split into 80% training and 20% validation cohorts. On the 80% training data, we performed fivefold cross-validation to tune the parameters of each of the six machine learning models. The six machine learning models tuned were logistic regression, Random Forest, Decision Trees, Gradient Boosting, K-Nearest Neighbor (KNN), and Support Vector Machine (SVM) algorithms. The best-performing parameters from cross-validation were used to train on all 80% of data to obtain the final models. These models aimed to predict patients without complete inter-clinician diagnostic agreement. Model performance was assessed using accuracy, F1 score, and the receiver operating characteristic (AUC-ROC) on the validation cohort, with metrics ranging from 0.0 to 1.0, where values closer to 1.0 indicate higher performance [20]. Calibration plots were created to compare predicted and observed probabilities for each of the six models. A perfectly calibrated model’s curve should align closely with the diagonal, indicating accurate predictions. The hyperparameters that were tuned were the AUC-ROC and F1 score using the fivefold cross-validation on the 80% training set only. The reported performance metrics (accuracy, F1, AUC-ROC) and calibration curves were all based on the 20% held-out validation cohort. Two sensitivity analyses were conducted to evaluate overly stringent threshold for inter-clinician agreement and model evaluation was performed for near-perfect cosign similarity scores thresholds (≥ 0.95; ≥ 0.90).
Feature importance was calculated using Random Forest algorithm to identify patient, clinical, and clinician features predictive of inter-clinician diagnostic agreement on shock etiology. Random Forest algorithm ranks feature importance in decision tree regression [21]. Analyses were performed in Python version 3.10.9.
Results
There were 7302 unique patients admitted to the ICU with shock with documented shock by at least two different clinicians on one day in a total of 35,411 notes. In total, 5975 (81.8%) patients had complete inter-clinician diagnostic agreement of the shock etiology at any time during the first four days of shock presentation. Conversely, 1327 (18.2%) never had complete inter-clinician diagnostic agreement of shock etiology.
Patients without complete inter-clinician diagnostic agreement were more often Black (20.5 vs 16.2%, p = 0.011), compared to patients with complete inter-clinician diagnostic agreement (Table 1). Patients without complete inter-clinician diagnostic agreement more often had a SOFA score greater than 15 (12.1 vs 7.6%, p < 0.001) (Table 2). Patients without complete inter-clinician diagnostic agreement more often had an Elixhauser Comorbidity Index greater than 10 (39.1 vs 31.6%, p < 0.001).Table 1. Shock patient demographics by whether there was complete inter-clinician diagnostic agreement of shock etiology captured in electronic health record clinician notes in 9 acute care hospitals from 2018 to 2023Never had total agreement, N (%)Evidence of total agreement, N (%)p-valueN = 1327 (18.2)N = 5975 (81.8)Age (years) 50 and under171 (12.9)833 (14.0)0.634 51 to 60169 (12.7)820 (13.8) 61 to 70337 (25.4)1454 (24.4) 71 to 80357 (26.9)1576 (26.5) 81 and older293 (22.1)1273 (21.4)Sex Male756 (57.0)3348 (56.0)0.554 Female571 (43.0)2627 (44.0)Race White872 (65.7)4181 (70.0)0.011 Black or African American272 (20.5)970 (16.2) Asian43 (3.2)222 (3.7) Native Hawaiian or Other Pacific Islander3 (0.2)13 (0.2) American Indian or Alaska Native5 (0.4)14 (0.2) Other90 (6.8)410 (6.9) Unknown, declined, unable to answer42 (3.2)165 (2.8)Ethnicity Hispanic, Latino, or Spanish origin113 (8.5)544 (9.1)0.159 Not Hispanic, Latino, or Spanish origin1158 (87.3)5239 (87.7) Unknown, declined, unable to answer56 (4.2)192 (3.2)Insurance Medicare843 (63.5)3664 (61.3)0.152 Medicaid166 (12.5)719 (12.0) Private302 (22.8)1484 (24.8) Self-Pay16 (1.2)108 (1.8)ADI national rank < 25209 (27.4)875 (25.0)0.235 25–49260 (34.0)1307 (37.3) 50–74206 (27.0)943 (26.9) 75–10080 (10.5)357 (10.2) Unknown9 (1.2)23 (0.7)ADI state rank 1–2275 (36.0)1219 (34.8)0.04 3–5269 (35.2)1399 (39.9) 6–10211 (27.6)864 (24.7) Unknown9 (1.2)23 (0.7)BMI body mass index, ICU intensive care unit, ADI area deprivation indexTable 2Shock patient clinical features by whether there was complete inter-clinician diagnostic agreement of shock etiology captured in electronic health record clinician notes in 9 acute care hospitals from 2018 to 2023Never had total agreement, N (%)Evidence of total agreement, N (%)p-value1327 (18.2)5975 (81.8)First SOFA score 0–6 (< 2%)509 (38.4)2439 (40.8) < 0.001 7–12 (0–30%)451 (34.0)2219 (37.1) 13–15 (40–90%)152 (11.5)624 (10.4) 16–24 (> 90%)161 (12.1)452 (7.6) No SOFA score54 (4.1)241 (4.0)Sepsis Score 072 (5.4)370 (6.2)0.011 155 (4.1)279 (4.7) 269 (5.2)358 (6.0) 398 (7.4)605 (10.1) > = 4752 (56.7)3191 (53.4) Unknown281 (21.2)1172 (19.6)Shock index < 0.553 (4.0)222 (3.7) < 0.001 0.5–0.7 (normal)306 (23.1)1646 (27.5) 0.7–1.0609 (45.9)2820 (47.2) > 1.0359 (27.1)1286 (21.5) Unknown0 (0.0)1 (0.0)Shock Etiology* Septic Shock1107 (83.4)3860 (64.6) < 0.001 Cardiogenic Shock698 (52.6)1389 (23.2) < 0.001 Hypovolemic Shock433 (32.6)755 (12.6) < 0.001 Adrenal Insufficiency Shock366 (27.6)448 (7.5) < 0.001 Neurogenic Shock13 (1.0)22 (0.4)0.007 Undifferentiated202 (15.2)139 (2.3) < 0.001 Obstructive Shock305 (23.0)539 (9.0) < 0.001 Anaphylactic Shock9 (0.7)36 (0.6)0.901 Post-procedural Shock2 (0.2)0 (0.0)0.033Elixhauser comorbidity index 0–592 (6.9)830 (13.9) < 0.001 5–6201 (15.1)1121 (18.8) 7–10515 (38.8)2136 (35.7) > 10519 (39.1)1888 (31.6)BMI < 18.585 (6.4)314 (5.3)0.399 18.5–24.9360 (27.1)1539 (25.8) 25.0–29.9291 (21.9)1370 (22.9) 30.0–34.9185 (13.9)827 (13.8) 35 and above171 (12.9)842 (14.1) Unknown235 (17.7)1083 (18.1)ICU Admission day Weekday1019 (76.8)4491 (75.2)0.226 Weekend308 (23.2)1484 (24.8)First Diagnosis of Shock day Weekday978 (73.7)4429 (74.1)0.775 Weekend349 (26.3)1546 (25.9)Number of unique clinicians per patient (mean (SD))4.82 (2.79)4.86 (2.62)0.670*****Each row represents a separate statistical comparison. Only the number (and percent) of patients who had a diagnosis of each type of shock are presented in the rowsSOFA sequential organ failure assessment, NOS not otherwise specified, SD standard deviation
Patients without complete inter-clinician diagnostic agreement less frequently had improvements in SOFA scores between days 0 and 4 (34.7 vs 41.9%, p < 0.001) compared to patients with complete inter-clinician diagnostic agreement. Patients without complete inter-clinician diagnostic agreement more frequently had procedures such as arterial line placement (40.4 vs. 34.5%, p < 0.0001), central venous catheter placement (49.0 vs.41.9%, p < 0.0001), and continuous renal replacement therapy (21.5 vs. 12.5%, p < 0.0001) (Table 3). However, patients without complete inter-clinician diagnostic agreement more frequently received first antibiotic at > 96 h, (9.3 vs 11.6%, p = 0.002). Patients without complete inter-clinician diagnostic agreement more often died in the ICU (39.7 vs. 26.8%, p < 0.001) and more often died in-hospital (41.5 vs. 27.6%, p < 0.001). Clinician characteristics demonstrated that resident/fellow clinical notes more frequently never had complete inter-clinician diagnostic agreement (37.8 vs. 29.3%, p < 0.001) (Table 4).Table 3. Shock patients clinical course by whether there was complete inter-clinician diagnostic agreement of shock etiology captured in electronic health record clinician notes in 9 acute care hospitals from 2018 to 2023Never had total agreement, N (%)Evidence of total agreement, N (%)p-value1327 (18.2)5975 (81.8)SOFA score last-first change Improvement460 (34.7)2503 (41.9) < 0.001 No change/Worse score503 (37.9)1848 (30.9) No score reported54 (4.1)241 (4.0) Only one value310 (23.4)1383 (23.1)Time To First IV Fluid Bolus < 24 h1251 (94.3)5668 (94.9)0.566 25–48 h44 (3.3)161 (2.7) 49–72 h18 (1.4)75 (1.3) 73–96 h5 (0.4)37 (0.6) > 96 h9 (0.7)34 (0.6)Fluids Administered Day 01252 (94.3)5442 (91.1) < 0.001Fluids Administered Day 11018 (76.7)4412 (73.8)0.033Fluids Administered Day 2830 (62.5)3583 (60.0)0.088Fluids Administered Day 3708 (53.4)3134 (52.5)0.572Fluids Administered Day 4634 (47.8)2728 (45.7)0.170Antifungals Administered53 (4.8)266 (5.4)0.453Time To First Antibiotic < 24 h763 (57.5)3597 (60.2)0.002 25–48 h40 (3.0)173 (2.9) 49–72 h41 (3.1)100 (1.7) 73–96 h19 (1.4)97 (1.6) > 96 h154 (11.6)553 (9.3) N/A310 (23.4)1455 (24.4)Anticoagulation Administered817 (61.6)3410 (57.1)0.003Diuretic Administered* Furosemide401 (30.2)1784 (29.9)0.821 Bumetanide358 (27.0)1182 (19.8) < 0.001Time To First Lab Draw < 24 h699 (52.7)3198 (53.5) < 0.001 25–48 h105 (7.9)417 (7.0) 49–72 h65 (4.9)288 (4.8) 73–96 h57 (4.3)214 (3.6) > 96 h342 (25.8)1256 (21.0) NA59 (4.4)602 (10.1)Time To First Echo < 24 h21 (1.6)64 (1.1)0.176 25–48 h27 (2.0)88 (1.5) 49–72 h12 (0.9)36 (0.6) 73–96 h6 (0.5)24 (0.4) > 96 h20 (1.5)69 (1.2) N/A1241 (93.5)5694 (95.3)Time To First Surgery < 24 h100 (7.5)580 (9.7)0.107 25–48 h52 (3.9)264 (4.4) 49–72 h39 (2.9)199 (3.3) 73–96 h36 (2.7)129 (2.2) > 96 h91 (6.9)384 (6.4) N/A1009 (76.0)4419 (74.0)Arterial line placement536 (40.4)2062 (34.5) < 0.001Cardiac catheterization108 (8.1)405 (6.8)0.090Central venous catheter placement650 (49.0)2504 (41.9) < 0.001Continuous renal replacement therapy285 (21.5)746 (12.5) < 0.001Interventional radiology procedure1 (0.1)5 (0.1)1.000**ICU Mortality527 (39.7)1601 (26.8) < 0.001Discharge Disposition Acute Care Hospital17 (1.3)123 (2.1) < 0.001 Acute Inpatient Rehabilitation117 (8.8)581 (9.7) Long-term Facility273 (20.6)1397 (23.4) Home368 (27.7)2198 (36.8) Death551 (41.5)1648 (27.6) Unknown1 (0.1)28 (0.5)Each row represents a separate statistical comparison. Only the number (and percent) of patients who received the respective procedure or medication are presented in the rowsFisher’s Exact testHrs hours, IV intravenous, ICU intensive care unitTable 4Shock patient clinicians’ characteristics by whether there was complete inter-clinician diagnostic agreement of shock etiology captured in electronic health record clinician notes in 9 acute care hospitals from 2018 to 2023Never had total agreement, N (%)Evidence of total agreement, N (%)p-valueN* = 6398N = 29,013Clinician type Physician2691 (42.1)13,665 (47.1) < 0.001 Resident/Resident Fellow2417 (37.8)8498 (29.3) Advanced Practice Provider (PA/NP)794 (12.4)4200 (14.5) Nurse91 (1.4)521 (1.8) Medical Student68 (1.1)334 (1.2) Non-shock Clinician25 (0.4)120 (0.4) Other258 (4.0)1414 (4.9) Other student/trainee9 (0.1)52 (0.2) Unknown45 (0.7)209 (0.7)Clinician Specialty Critical Care Medicine364 (5.7)2248 (7.7) < 0.001 Internal Medicine2764 (43.2)12,681 (43.7) Cardiology627 (9.8)2593 (8.9) Surgery575 (9.0)2660 (9.2) Neurology/Neurological Surgery428 (6.7)1421 (4.9) Infectious Disease248 (3.9)1419 (4.9) Anesthesiology269 (4.2)903 (3.1) Emergency Medicine268 (4.2)794 (2.7) Gastroenterology164 (2.6)646 (2.2) Obstetrics and Gynecology42 (0.7)271 (0.9) Non-shock Specialty178 (2.8)871 (3.0) Other232 (3.6)1197 (4.1) Unknown239 (3.7)1309 (4.5)PA physician assistant, NP nurse practitioner
Six models were constructed to predict which patients never had complete inter-clinician diagnostic agreement of shock etiology and all were highly predictive (eTable 2). Logistic regression (Accuracy: 0.8597, F1 Score: 0.9117, AUC-ROC: 0.9257), Random Forest (Accuracy: 0.8658, F1 Score: 0.9201, AUC-ROC: 0.9255), and gradient boosting (Accuracy: 0.8515, F1 Score: 0.9138, AUC-ROC: 0.9227) were the three highest performing models. Model calibration curves for logistic regression, gradient boosting, and SVM were closest to the diagonal line suggesting that these models provide more reliable probability estimates (Fig. 1). The KNN model showed poor calibration, with its curve deviating significantly from the diagonal, indicating the model’s predicted probabilities were misaligned with the observed probabilities. The most important features in the Random Forest model predicting patients lacking inter-clinician diagnostic agreement on shock etiology were variations in shock etiology diagnoses (eFig. 2).Fig. 1. Calibration plots of machine learning model predicting never having complete inter-clinician diagnostic agreement of shock etiology within 9 acute care hospitals from 2018 to 2023
More lenient similarity cosign similarity thresholds (e.g., ≥ 0.95, ≥ 0.90) were tested to reflect real-world diagnostic convergence. A cosign similarity threshold of 0.95 demonstrated 16.3% of patients never had inter-clinician diagnostic agreement (eTables 3–6). A cosign similarity threshold of 0.90 demonstrated 16.1% of patients never had inter-clinician diagnosis agreement (eTables 7–10). These relaxed threshold sensitivity analyses demonstrated association stability and comparative model performance with a stringent threshold.
Discussion
This study sought to characterize inter-clinician diagnostic agreement of shock etiology. Using a novel application of cosine similarity score we quantified 18.2% of shock patients never had complete inter-clinician diagnostic agreement. Furthermore, logistic regression and gradient boosting best predicted which patients would never have complete inter-clinician diagnostic agreement of shock etiology and were well calibrated. The findings of the current study fill a knowledge gap in quantifying rate of inter-clinician diagnostic agreement of shock etiology in actual clinical care never previously investigated.
This study builds upon previous literature which demonstrates that diagnostic agreement between different clinicians is poor [9, 22]. One study demonstrated that different specialty clinicians reached different conclusions, even when presented with the same clinical information, as a result of their discipline-specific frame of reference [23]. Furthermore, that patients without inter-clinician diagnostic agreement were more often Black was concerning. Racial difference in agreement was based on unadjusted comparisons and should be interpreted alongside social or contextual variables. Differences in diagnostic agreement may reflect a combination of illness severity, comorbidity burden, neighborhood environment and social determinants of health, as well as clinician documentation or communication patterns, rather than race alone. Currently, there is no standardized way for clinicians to share real-time diagnostic assessments, develop a shared understanding of shock etiology, or reach consensus on treatment [23–27]. The lack of consensus may delay diagnosis, and treatment, or as we saw lead to aggressive possibly unnecessary treatment ultimately thus increasing mortality.
The implications of this study underscore the critical need to design a systematic process to share information regarding clinicians' specialty-specific assessments to build a shared understanding of the shock etiology among all clinicians who care for shock patients. The association between diagnostic disagreement, more aggressive treatments and adverse clinical outcomes (e.g., reduced improvement in SOFA scores, increased mortality) was a significant finding that underscores the clinical consequences of fragmented diagnostic processes. Potential mechanisms include clinician-patient discordance, documentation variability, differential access from neighborhood deprivation, and heuristic bias. Although causal inference is limited by the design, the consistent associations and sensitivity analyses highlight a target group of patients where timely, structured inter-professional communication for reconciliation of the diagnosis may offer benefit to offer more narrow, targeted earlier treatment. The National Academy of Science has recognized that inter-professional communication is an essential component to the diagnostic process for patients with complex and highly lethal conditions, such as shock [28]. Identifying the patients more likely to experience clinician diagnostic disagreement,such as with our machine learning model, could be used in clinical practice to prompt inter-clinician communication mechanisms, to improve diagnostic agreement , optimize timely treatment, and ultimately reduce mortality. Prospective evaluation of this clinician decision support system is our next step.
This study has several limitations that are largely mitigated by a thorough study design. First, sampling bias was present as the study population encompassed patients from nine hospitals in a single integrated health system. However, the study population included thousands of patient encounters from many different ICUs across nine very different acute care hospitals in a geographically varied state. Thus, the results are likely generalizable to a wide range of ICUs and hospitals. Second, selection bias may have been introduced as the study excluded patients where only one clinician note mentioned a diagnosis of shock because inter-clinician diagnostic agreement could only be calculated when at least two different clinicians documented a shock diagnosis. Therefore, the patients included in this study may be biased towards the most complex patients requiring many clinicians with high illness severity. This limits generalizability of our findings to less complex shock patients. The broader goal of this ongoing project is to identify patients who benefit from a real-time inter-professional communication intervention to enhance shock etiology diagnosis. One of the major concerns in our follow-up qualitative analysis and user-centered design study, were clinician alert fatigue. Excluding more straightforward cases of shock where only one clinician was involved therefore is a relative strength . External validation in other health systems to demonstrate generalizability to predict patients without inter-clinician diagnostic agreement is needed. Third, this study quantitatively analyzed inter-clinician diagnostic agreement among shock etiology but did not capture qualitative data regarding inter-clinician diagnostic agreement. A qualitative study investigating the barriers and facilitators of inter-professional communication in shock diagnosis is beyond the scope of this study and is forthcoming. Fourth, our approach has limitations inherent to regular expressions applied on clinical notes. Terminology varies by author, and documentation may lag behind clinical judgment. We mitigated this by: (1) using a strict lexicon with explicit string matches for each shock etiology and excluding negated statements; (2) requiring ≥ 2 independent clinician notes per patient-day to compute agreement; and (3) analyzing agreement over the first five hospital days rather than at a single time point. For septic shock, we used exact terms (“sepsis,” “septic,” “septic shock”) without negation and manually reviewed all occurrences to ensure context-sensitive language did not drive misclassification. A separate expert-consensus adjudication would be ideal, but our primary endpoint was agreement between clinicians as documented, not the correctness of any single diagnosis. Because the our pipeline captured the explicit labels clinicians recorded, consistent extraction across notes allowed valid estimation of relative agreement even if some absolute labels were imperfect. Construct validity supports this: patients without complete agreement had higher severity (SOFA > 15), more aggressive treatment (e.g., central venous access, Ccontinuous renal replacement, anticoagulation, bumetanide administration), slower antibiotic initiation, and higher ICU and in-hospital mortality—patterns expected when diagnostic consensus is difficult. These convergent findings suggest the regular expression labels reflected clinically meaningful discordance. Future work will include external validation in other health systems, expanded lexicons and abbreviation handling, and a sampled chart-review adjudication to quantify precision/recall across etiologies. Nonetheless, given our focus on measured agreement, system-wide scale (35,411 notes across nine hospitals), and the targeted manual review for septic shock, we believe the present findings are robust and informative.
Lastly, the study period overlapped with the COVID-19 pandemic which had a significant impact on outcomes for critically ill patients. However, the COVID-19 pandemic period was distributed evenly between patients with and without complete inter-clinician diagnostic agreement.
Conclusion
This study is one of the first to quantify inter-clinician diagnostic agreement of shock etiology in clinical care. Patients without complete inter-clinician diagnostic agreement of shock etiology can be successfully predicted. These results highlight an opportunity to identify and improve the diagnostic process for shock patients. We believe this can be achieved through optimizing the inter-professional communication in the diagnostic process to improve the inter-clinician diagnostic agreement, treatment, and mortality of shock patients.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 37 KB)