Systematic mapping review of applications of extracorporeal shockwave therapy (ESWT) in hand surgery
Ryan Faderani, Zhen Yu Wong, Oluwatobi Adegboye, Muholan Kanapathy, Dariush Nikkhah, Afshin Mosahebi

TL;DR
This review summarizes current research on using shockwave therapy for hand conditions, finding short-term benefits but calling for more standardized studies.
Contribution
A systematic mapping of ESWT applications in hand surgery, identifying gaps in evidence and protocol standardization.
Findings
ESWT shows short-term improvements in conditions like carpal tunnel syndrome and trigger finger.
Treatment protocols vary widely, and most studies have moderate to high risk of bias.
Long-term efficacy and optimal treatment parameters remain unclear.
Abstract
This systematic mapping review aims to consolidate and categorize existing evidence regarding the utilization of extracorporeal shockwave therapy (ESWT) in hand surgery. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline, a comprehensive search was performed to identify studies assessing ESWT in hand conditions. Eligible studies required a minimum of 3 months’ follow-up. Data extraction adhered to predetermined criteria, and outcomes were classified into clinical assessment, patient-reported outcome measures (PROMs), neurophysiological tests, and miscellaneous domains. Thirty studies met inclusion criteria, comprising 18 randomized controlled trials (RCTs), 10 case series, and two cohort studies. Evidence was predominantly centered on carpal tunnel syndrome (CTS), with additional studies addressing trigger finger, Dupuytren’s disease,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
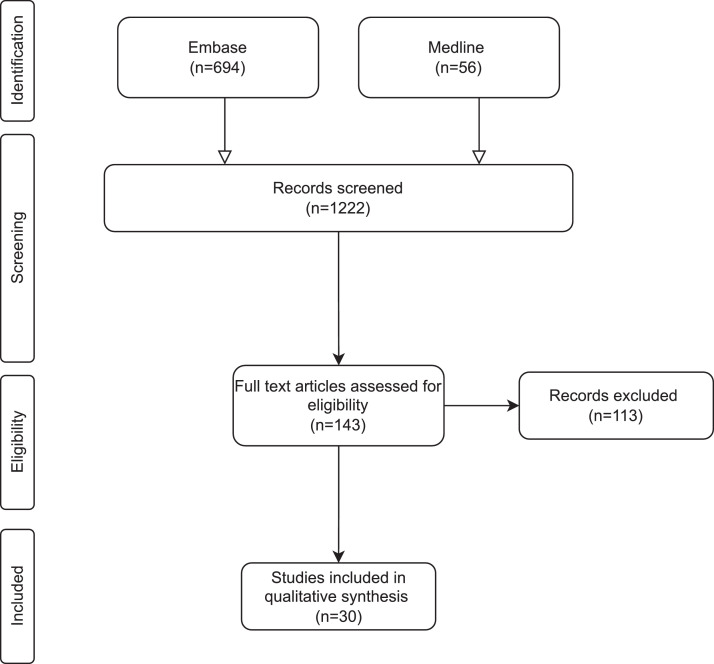 Figure 1
Figure 1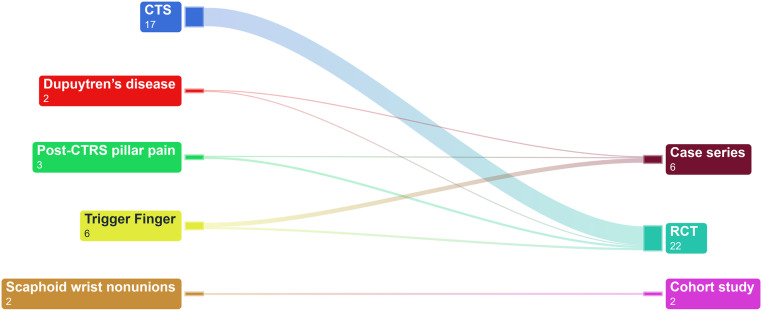 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTendon Structure and Treatment · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
Hand conditions are common presentations to healthcare services globally and if not treated appropriately, they are associated with a significant impact on quality of life and a wider socioeconomic impact.1 Extracorporeal shockwave therapy (ESWT) is a relatively novel non-surgical modality that has increasingly been used to manage musculoskeletal conditions, including those of the hand.2
ESWT is a non-invasive therapy that delivers acoustic pulses to the target area, it was originally designed for lithotripsy to treat renal stones; however there has been growing trend in its use for musculoskeletal conditions. ESWT has shown several potential benefits when managing musculoskeletal conditions, such as alleviating pain and improving function, leading to a notable popularization over the past few years, especially within orthopedics, physiotherapy, and sports medicine3^,^4 supported by various biological studies. It operates through different mechanisms on bone, tendon, and skin as well as pain control.5, 6, 7, 8 For one-related conditions such as scaphoid wrist nonunions and Kienböck’s disease, ESWT appears to promote healing in fractures and tendon-to-bone healing, potentially through mechanotransduction pathways, though evidence for shockwave-induced micro-fractures is limited.9 For tendon pathologies, ESWT may be beneficial in conditions like trigger finger and de Quervain’s tenosynovitis, where its anti-inflammatory effects contribute to reducing fibrosis, improving lubricin production for tendon gliding, and accelerating extracellular matrix biosynthesis.10^,^11 This effect extends to Dupuytren’s disease, where ESWT could potentially modulate fibroblast activity and reduce contracture progression, although further studies are needed. In post-carpal tunnel release (CTRS) pillar pain, ESWT's ability to decrease nerve fiber excitability and modulate pain pathways suggests a role in post-surgical pain management, potentially reducing reliance on prolonged conservative measures.12 Similarly, in hypertrophic hand scars, ESWT has been shown to enhance neocollagenesis and neoangiogenesis, improving collagen organization and skin elasticity, making it a potential adjunct in scar remodeling.
ESWT’s recent growth is attributed to its non-invasive nature and technological advancements that make devices more practical. Moreover, contemporary ESWT studies on musculoskeletal conditions have displayed positive patient outcomes and tolerable side effect profiles.13 Previous research has explored the use of ESWT in individual hand conditions, most notably carpal tunnel syndrome (CTS), however, there is a paucity of agglomerated work on ESWT usage in a spectrum of hand conditions. Current practice in ESWT usage remains largely unregulated, it is heavily dependent on operator preference rather than evidence-based medicine, and there is a notable lack of standardization in delivery protocols. This variability in practice may lead to inconsistencies in treatment outcomes and hinder the ability to compare results across studies. Furthermore, much of the existing literature is restricted to short follow-up periods of less than three months, which are insufficient to determine the durability or true clinical value of ESWT. Identifying and understanding the existing evidence of ESWT usage in hand surgery would enable us to recognize gaps or limitations in the literature and provide valuable insights to design future clinical trials, allowing for more targeted and effective research efforts in this area. This systematic review aims to provide an overview of application of ESWT in hand surgery.
Methods
Search strategy
In accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement,14^,^15 a search was conducted across Medline and Embase databases for studies that fulfilled inclusion criteria. In addition, the references of included articles and previous meta-analysis were also screened manually for a comprehensive search. The search term used was a permutation of ‘shockwave’ and hand surgery conditions. The details of search strategy can be found in Supplementary Material 1.
Inclusion Criteria
Full text English articles including case series, retrospective and prospective cohort studies, cross-sectional studies, and randomized controlled trials which investigated the application of shockwave therapy in hand surgery conditions with at least three months follow up
Exclusion criteria
- 1.Case reports, reviews, commentaries, letter to editors, and editorials
- 2.Non-English language studies
- 3.Conference abstract without full text
Outcome measures
The evaluated outcomes could be categorized into four dimensions: clinical assessment, Patient-Reported Outcome Measures (PROMs), neurophysiological tests, and a miscellaneous category encompassing imaging, patient satisfaction, and Immunohistochemical staining.
Study selection and data management
Preliminary abstract screening was carried out by two authors (ZYW and OA) independently while a senior independent author (RF) resolved any disputes through consensus. Two independent authors (ZYW and OA) extracted the relevant information from the included articles into a designed proforma. Study characteristics including author, year of study, country of origin, protocol for shockwave therapy, conditions, follow up time, adverse events and assessed outcomes were also extracted. PRISMA flowchart for the selection process and systematic mapping of all included studies based on was constructed. Data were analyzed and narratively summarized using descriptive statistics in tables or graphs for each objective of the study. R Studio (version 4.0.3) was used for visualization of spatial data. Quality assessment of included articles was done with either the JBI critical appraisal tools for case series,16 ROBINS-I tools (Risk of Bias in Non-randomized Studies – of Interventions)17 or risk-of-bias tools for randomized trials (RoB2)18 depending on the study design. Extracted data were used to determine the strength of evidence as per the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. The Fragility Index (FI) was calculated using a publicly available free online calculator, using the methods described by Walsh et al.19
Results
Search and selection
The structured searching via search strings returned 1222 studies regarding this topic. Subsequently, 1079 studies were removed during first stage of selection via title and abstract. Further 100 studies were excluded following second stage selection by full text appraisal. Figure 1 summarizes the PRISMA flow diagram for the final 30 reviews for data extraction.Figure 1PRISMA flow chart.Figure 1
Characteristics of included studies
Table 1 provides results of data mapping conducted in this study. This study identified six case series,20, 21, 22, 23, 24, 25 two cohort study26^,^27 and 22 randomized controlled trials (RCT)28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50 (Figure 2). Among the 30 included studies (2143 patients) investigating shockwave therapy in hand surgery conditions, carpal tunnel syndrome was the subject of 17 studies, trigger finger in six, Dupuytren’s disease in two post-CTRS pillar pain in three, and scaphoid wrist nonunions in two. From the 30 reviews, institutions of the main author for the reviews were reported from 12 countries; Turkey (7), Iran (6), Taiwan (4), Italy (3), Austria (3), and one each for Korea, Egypt, Thailand, Germany, China, Poland, and Greece. Most case series were rated as moderate to high quality, whereas the one cohort studies had a moderate risk of bias, and the majority of RCTs showed moderate to high risk of bias (Table 2, Table 3, Table 4). The follow-up time in the included studies ranged from 3 month to 18 months. Eighteen studies had a follow-up of more than 3 months but less than 6 months, while twelve had follow-up durations ranging from 6 months to 1 year. There is variability in shockwave therapy protocol, with the number of sessions ranging from 1 to 18, the total number of shots/pulses ranging from 1000 to 36,000, and energy frequency ranging from 3 to 15, with energy density measured in variable units. About 13% (four out of 30) of studies used shockwave therapy as an adjunct, while 86% (26 out of 30) used it as the primary treatment. Five studies utilized single session ESWT. Eleven studies reported the use of radial extracorporeal shock wave therapy (rESWT), six studies reported the use of focused extracorporeal shock wave therapy (fESWT), and one study used both. The type of shock wave therapy used in the remaining studies was not specified. The most frequently studied clinical assessment was grip and pinch strength, while VAS and BCTQ scores were the most popular patient-reported outcome measures (PROMs) studied. Neurophysiological tests mainly measured sensory nerve conduction velocity (SNCV), distal motor latency (DML), and distal sensory latency (DSL). As shown in Table 5, the overall quality of evidence for the use of shockwave therapy in hand surgery conditions was low to very low, except for carpal tunnel syndrome (CTS), which had high-quality evidence rating. FGI was calculated for all 22 RCTs included, and all trials were found to have an FGI of zero (Table 2, Table 3, Table 4).Table 1. Characteristic of studies.Table 1. YearAuthorStudy designCondition(s)Study detailsComparator groupTotal number of sessionsTotal number of shots/pulsesEnergy frequency (Hz)Energy densityAs primary treatmentAs an adjunct treatmentCountryHospitalFollow up timeNo. of patientsClinical assessmentPROMsNeurophy-siological testOthersAdverse events2011Romeo. P.Case seriesPost-CTRS pillar painESWT3280040.03 mJ/mm2YNMilano, ItalyIstituto Ortopedico Galeazzi4 months40Not reportedVASNot reportedNot reportedNot reported2013Seok, H.RCTCTSESWTLCI1100060.09 - 0.29 mJ/mm2YNBucheon, KoreaSoonchunhyang University,3 months36Not reportedVAS, Levine Selfassessment QuestionnaireDML, SNAP, CMAP, Semmes-Weinstein testingNot reportedN2015Notarnicola, A.RCTCTSESWT + median nerve glide exercises + splintnutraceutical diet + median nerve glide exercises + splint3480040.03 mJ/mm2YNBari, ItalyUniversity of Study of Bari6 months60Not reportedVAS, BCTQ, Roles and Maudsley ScoresSNCV, DMLNot reportedNot reported2015Paoloni, M.RCTCTSESWTUS therapy; cryo-US therapy410,000Not reported0.05 mJ/mm2YNRome, ItalySapienza University of Rome,12 weeks25Not reportedVAS, BCTQNot reportedNot reportedN2016Vahdatpour, BRCTCTSESWT + splint + NSAIDssham ESWT + NSAIDs + Splint + vitamin B14380030.05, 0.07, 0.1, and 0.15 mJ/mm2YNIsfahan, IranIsfahan University of Medical Sciences6 months60Not reportedVAS, LSQDML, SNAP, CMAPNot reportedNot reported2016Ke, M. J.RCTCTSESWT + splintsingle session of ESWT + splint; sham ESWT + splint3600050.003–0.89mJ/mm2YNTaipei, TaiwanTri-Service General Hospital14 weeks69Not reportedBCTQCSA, SNCVNot reportedN2016Wu, Y. T.RCTCTSESWT + splintsham ESWT + splint360005Not reportedYNTaipei, TaiwanTri-Service General Hospital12 weeks34Pinch strengthVAS, BCTQCSA, NCVNot reportedN2016Yildirim, P.RCTTrigger FingerESWTlocal corticosteroid injection3300015Not reportedYNBulvari, TurkeyKocaeli Derince Training and Research Hospital6 months40FT, ST, FITNPRS, DASHNot reportedNot reportedN2016Malliaropoulos, N.Case seriesTrigger FingerESWT120005-6Not reportedYNThessaloniki, GreeceThessalonikiMusculoskeletal Clinic12 months44Not reportedVAS, Roles and Maudsley ScoresNot reportedNot reportedN2017Raissi, G. R.RCTCTSESWT + splintSplint330006low-energyNYArak, IranArak University of Medical Sciences12 weeks40Not reportedNRS, DASHSNAP, CMAP, DML, DSLNot reportedY2018Atthakomol, P.RCTCTSESWTLCI1500015Not reportedYNChiang Mai, ThailandChiang Mai University,24 weeks25Not reportedBCTQDML, SNAP, CMAP, DSLNot reportedY2019Karatas, O.RCTCTSESWT + splintsham ESWT + splint913,500Not reported0.10 mJ/mm2YNAnkara, TurkeyAntalya Training and Research Hospital3 months49Grip strength, paresthesiaVAS, MHQNCV, SNCV, SNAP, CMAP, DSLNot reportedN2019Haghighat, S.RCTPost-CTRS pillar painESWTsham ESWT4280040.03 mJ/mm2YNIsfahan, IranIsfahan University of Medical Sciences3 months40Not reportedVAS, MHQNot reportedNot reportedNot reported2019Quadlbauer, S.Cohort studyScaphoid wrist nonunionsESWT + Splint/castSplint/cast1300040.41 mJ/mm2YNVienna, AustriaAUVA Trauma Hospital Lorenz Böhler - European Hand Trauma and Replantation Center1 year42ROM, Grip strengthVAS, DASH. PRWE, MHQ, MAYONot reportedCT scanNot reported2020Xu, D.RCTCTSESWT + splint + NSAIDsLCI + splint + NSAIDs990006Not reportedYNNingbo, ChinaMedical Treatment Center Lihuili Hospital12 weeks55Not reportedBCTQSNAP, CMAPNot reportedY2020Chang, C. Y.RCTCTSESWT + PRPsham ESWT + PRP120005Not reportedNYTaipei, TaiwanTri-Service General Hospital6 months40Not reportedBCTQCSA, SNCV, DMLNot reportedN2020Vahdatpour, B.Case seriesTrigger FingerESWT3300015Not reportedYNIsfahan, IranIsfahan University of Medical Sciences18 weeks19Quinnell grading systemVAS, DASHNot reportedNot reportedNot reported2020Dogru, M.Case seriesTrigger FingerESWT1020,00010Not reportedYNIzmir, TurkeyDokuz Eylul University3 months18Range of motion, Grip strength, and Pinch strengthNPRS, DASHNot reportedNot reportedNot reported2020Zyluk, A.Case seriesTrigger FingerESWT360008Not reportedYNSzczecin, PolandPomeranian Medical University3 months32Grade of triggering in Froimson scaleNPRS, Froimson ScaleNot reportedNot reportedN2021Ulucakoy, R.RCTCTSESWTESWT+splint; splint; splint+sham ESWT3300050.05 mJ/mm2YNAnkara, TurkeyAnkara Numune Training and Research Hospital3 months189Not reportedVAS, BCTQ, LANSSSNCV, DML, DSLNot reportedN2021Elrazik, R. K. A.RCTCTSESWTiontophoresis therapy.1836,000Not reported0.03 mJ/mm2YNCairo, EgyptModern University for Technology and Information18 weeks30Not reportedVASDSLNot reportedNot reported2021Gesslbauer, C.RCTCTSESWT + splintsham ESWT + splint3150040.05 mJ/mm2YNVienna, AustriaMedical University of Vienna12 weeks30Grip strengthVAS, BCTQ, SF-36SNCV, DMLNot reportedN2021Turgut, M. C.RCTPost-CTRS pillar painESWTsham ESWT3600050.03 mJ/mm2, 400 kPaYNTrabzon, TurkeyKaradeniz Technical University Medical Faculty,6 months60Pillar pain, Grip strengthVAS, MHQNot reportedNot reportedNot reported2021Chen, Y. P.RCTTrigger Fingerhigh energy ESWTlow energy ESWT; sham ESWT46000Not reported0.01 mJ/mm2, 580 kPaYNTaipei, TaiwanTaipei Medical University6 months60FT, ST, FITVAS. DASHNot reportedNot reportedN2022Ozturk Durmaz, H.RCTCTSESWT + splintLCI + splint ; splint360005Not reportedYNAnkara, TurkeyAhi Evran University Physical Medicine and Rehabilitation Outpatient Clinic12 weeks72Grip strengthVAS, BCTQDML, DSLNot reportedY2022Saglam, G.RCTCTSESWT + median nerve glide exercises + splintMedian nerve glide exercises + splint; Median nerve glide exercises + splint + TENS + US360005Not reportedYNErzurum, TürkiyeErzurum Regional Training and Research Hospital3 months95Not reportedVAS, BCTQ, LANSSDML, DSLNot reportedN2022Knobloch, K.RCTDupuytren’s diseaseESWTsham ESWT36000Not reported0.35 mJ/mm2YNHannover ,GermanyHannover Medical School18 months52Grip strength and Dupuytren’s disease progressionVAS, DASH, MHQ, URAMNot reportedPatient’s satisfactionN2022Taheri, P.Case seriesDupuytren’s diseaseESWT612,00031.24 mJ/mm2YNIsfahan, IranIsfahan University of Medical Sciences14 weeks20Contracture angleVAS, DASHNot reportedNot reportedY2023Gholipour, M.RCTCTSESWT + LCIsham ESWT + LCI410,40040.03 mJ/mm2NYTehran, IranAkhtar Hospital6 months40Not reportedVAS, GSSNCVProportion of participants referred for surgeryN2023Quadlbauer, S.Cohort studyScaphoid wrist nonunionstwo headless compression screws (HCS) vs angular stable scaphoid plate1300040.41 mJ/mm2NYVienna, AustriaAUVA Trauma Hospital Lorenz Böhler - European Hand Trauma and Replantation Center1 year38Grip strength, ROMVAS, DASH. PRWE, MHQ, MAYONot reportedCT scanNot reportedRCT, Randomized controlled trial; CTS, Carpal tunnel syndrome; ESWT, extracorporeal shockwave therapy; PRP, Platelet rich plasma; LCI, Local corticosteroid injection; US, Ultrasound; BCTQ, Boston Carpal Tunnel Questionnaire; VAS, Visual Analog Scale; MHQ, Michigan Hand Outcomes Questionnaire; NRS, Numeric Pain Rating Scale; Quick-DASH, Quick disabilities of the Arm, Shoulder, and Hand Questionnaire; GSS, Global symptom score; ADL, Activities of daily living; LANSS, Leeds Assessment of Neuropathic Symptoms and Signs; LSQ, Levine Self-Assessment Questionnaire; SF-36, 36-item Short Form Health Survey Questionnaire; CSA, Cross-sectional area; SNCV, Sensory conduction velocity; DML, Distal motor latency; NCV, Nerve conduction velocity; SNAP, Sensory nerve action potential; CMAP, Compound motor action potential; DSL, Distal sensory latency.Figure 2. Sankey diagram by study design.Figure 2. Table 2Risk of bias of case series using Joanna Briggs Institute (JBI) critical appraisal checklist.Table 2:Image, table 2Table 3Risk of Bias using the Risk of Bias for Randomized trials (ROBINS-II) tool.Table 3:Image, table 3Image, table 3Table 4Risk of Bias using Risk of Bias in Non-randomized studies – of Interventions (ROBINS-I) tool.Table 4:Image, table 4Table 5Assessment of quality using the GRADE system.Table 5. DiseasesNo. of studies (no. of participants)Risk of biasInconsistencyIndirectnessImprecisionPublication biasFactorQualityCTS17 (949)Serious (-1)----Large effect (+1)HighTrigger Finger6 (213)Serious (-1)--Serious (-1)Likely (-1)-LowDupuytren’s disease2 (72)---Very serious (-2)Very likely (-2)-Very lowPost-CTRS pillar pain3 (134)Very serious (-2)--Very serious (-2)Likely (-1)-Very lowScaphoid wrist nonunions2 (80)--Serious (-1)Very serious (-2)Very likely (-2)-Very low
CTS (n = 17,949 patients)
The included studies comprised one study of moderate carpal tunnel syndrome (CTS),31 ten studies of mild to moderate CTS30^,^33, 34, 35, 36^,^38^,^40^,^42, 43, 44, one study of mild to severe CTS,28 and three studies where the severity of CTS was not specified.29^,^32^,^39 Eight studies (546 patients) compared ESWT with sham treatments, physiotherapy, median nerve gliding exercises, or splinting. Seven out of eight studies superior results for ESWT. Particularly there is a trial comparing three-session versus one-session ESWT, which indicated that higher frequency resulted in better outcomes.33
All nine studies (403 patients) comparing ESWT with various treatment modalities, including, iontophoresis therapy, local corticosteroid injection (LCI), nutraceutical diet, ultrasound, and cryo-ultrasound therapy, demonstrated clinical benefit. Among these, five studies specifically compared ESWT to LCI. ESWT provided longer-lasting pain relief, with comparable outcomes to LCI at later time points, while LCI offered better short-term pain relief. Similarly, ESWT showed longer-lasting functional improvements, with studies reporting either sustained benefits for ESWT or comparable outcomes after LCI's initial short-term advantage diminished. In contrast, Paoloni et al. demonstrated that ESWT offered superior long-term pain relief at 12 weeks compared to ultrasound or cryo-ultrasound therapy. Chang et al. noted slight improvements in functional scores and nerve conduction when ESWT was combined with platelet-rich plasma (PRP) compared to PRP alone, though the differences were not significant. Notarnicola et al. compared ESWT with a nutraceutical regimen composed of Echinacea, alpha lipoic acid, and conjugated linoleic acid and found comparable improvements in pain and function with no significant differences between the two. Additionally, ESWT was found to be more effective than iontophoresis, as demonstrated by Elrazik et al., showing greater improvements in pain reduction and sensory nerve conduction velocity.
Trigger finger (n = 6,2132 patients)
The seven included studies (two RCTs, four case series)21^,^22^,^24^,^48, 49, 50 predominantly employed the Quinnell classification and Froimson Scale for categorizing trigger finger, with a primary emphasis on Grade 2 or more severe stages of the condition. In all studies, there was demonstrated superiority in in disease grading, pain, and PROMs. Yildirim et al. conducted a direct comparison, finding that both ESWT and corticosteroid injection led to significant improvements in pain, functional scores, and disease severity over a 6-month period Interestingly, one study demonstrated that high-frequency ESWT resulted in a superior outcome compared to low-frequency ESWT.50 The study by Malliaropoulos et al. also found a correlation between symptom duration and the number of sessions required.
Other hand surgical conditions
Among the four studies included on Dupuytren’s disease (72 patients), although all indicated clinical benefit, only one was an RCT.20^,^45^,^51^,^52 Knobloch et al.'s RCT showed significant pain reduction but non-significant changes in PROMs like DASH and MHQ scores and Taheri et al. reporting significant gains in grip strength, DASH scores, and MCP joint angles.
All three studies on CTRS pillar pain demonstrated benefits in pain reduction, with only one study employing PROMs to assess functional outcomes. In the investigation of scaphoid wrist non-union, ESWT was employed as an adjunct for both arms, making it difficult to ascertain superiority and clinical benefit.26 In another study by Quadlbauer et al, ESWT as an adjunct therapy resulted in 81% union rates compared to 75% in the non-ESWT group, though the difference was not statistically significant.27 However, patients in the ESWT group experienced significantly better pain reduction and Mayo scores, while significant difference improvements in other PROMs were not observed.
Adverse events
Most studies reported no adverse events, and in those where adverse events were documented, they were typically minor, transient, and self-limiting, often manifesting as temporary pain, erythema, swelling, bruising, tingling, or numbness at the treatment site, all of which resolved without intervention and with no reports of serious complications. While no adverse events were reported in studies utilizing fESWT, 4 out of 11 studies involving rESWT reported adverse events.
Discussion
Our review on the application of ESWT in hand surgery highlighted that the majority of published research focused on carpal tunnel syndrome (CTS). Most studies reported short-term benefits in clinical and PROMs, with minimal complications. However, there was considerable heterogeneity in shockwave therapy delivery protocols, particularly in intensity and frequency. The administration of shockwave therapy has been suggested to exhibit a dose-dependent effect without major complications, but this was reported in only a few studies. Although numerous studies, particularly those focusing on CTS, have investigated the use of ESWT, uncertainty persists due to the low quality of the available evidence.
The clinical benefit of ESWT in CTS appears to be influenced by disease severity and its comparison with other treatment modalities. Rashad et al. highlighted that ESWT might not be effective in severe CTS, making it the only study specifically evaluating its impact at this stage. While previous studies have demonstrated that ESWT promotes axonal regeneration, potentially accelerating Wallerian degeneration and enhancing axonal recovery, specific data on its efficacy in severe CTS remain lacking.
When compared to conservative management, ESWT showed superiority in-most studies. The lack of demonstrated superiority of ESWT in Ulucaköy et al and Karataş et al, likely stems from methodological limitations and study design factors. Ulucaköy et al showed improvements across all groups, including sham ESWT, suggesting a strong placebo effect or natural symptom resolution, particularly in mild-to-moderate CTS. Additionally, the lack of significant electrophysiological improvements raises questions about the true physiological impact of ESWT in this cohort. Karataş et al, despite using multiple ESWT sessions, failed to show superiority over sham ESWT, potentially due to high variability in baseline characteristics, insufficient standardization of ESWT parameters (intensity, frequency, and number of sessions), and a small sample size, limiting statistical power. These findings suggest that placebo effects, variability in ESWT protocols, short follow-up durations, and effective control interventions likely contributed to the lack of observed superiority in these studies, in contrast to trials with longer follow-ups, optimized treatment protocols, and larger sample sizes, which have generally reported better outcomes with ESWT. Based on the available evidence, ESWT is strongly supported as an effective treatment for mild-to-moderate CTS, either as a standalone therapy or in combination with conservative management, demonstrating superior outcomes.
When compared to other treatment modalities, ESWT was generally superior, except in phonophoresis, which demonstrated comparable outcomes. While phonophoresis may be a potential alternative, the current evidence remains unclear, whereas ESWT has more robust supporting data, reinforcing its role as an effective treatment for CTS. Chang et al. which demonstrated that combination of ESWT didn’t provide additional benefit with PRP used a single ESWT session with a small sample size, which may have contributed to its non-significant findings. Although the GRADE assessment suggested strong evidence, the FGI for all RCTs was zero, indicating that even a minor change in outcomes could nullify the significance of the findings. This contradictory result highlights the need for a large-scale, multinational clinical trial with an adequately powered sample to validate these conclusions.
The range of ESWT energy influx varies, with previous studies categorizing treatment intensity into three levels: low intensity (EFD, <0.08 mJ/mm^2^), medium intensity (EFD, 0.08-0.28 mJ/mm^2^), and high intensity (EFD, >0.28 mJ/mm^2^).5 In hand conditions, the majority of studies in this analysis utilized low intensity shockwave therapy. However, three included studies, one focusing on CTS and the other two on trigger finger, investigated the dose dependent effect of ESWT.33^,^48 All three studies reported a dose-dependent relationship with response, favoring high intensity, as evidenced by significant improvements in patient-reported outcomes and pain reduction. Ke et al. and Chen et al. that higher energy levels resulted in superior symptom relief, functional gains, and longer-lasting effects compared to lower-intensity ESWT. Malliaropoulos et al. further highlighted the importance of treatment frequency, noting that multiple ESWT sessions enhanced outcomes, suggesting that dose dependency may extend beyond energy levels to the number of sessions delivered. Moreover, a study conducted on endothelial progenitor cells of rats in vitro has demonstrated that high-energy shock waves resulted in a decrease in the expression of most cytokines, except for apoptotic factors and fibroblast growth factor 2, ultimately leading to cellular apoptosis.53 Nonetheless, the dose-dependent relationship remains associational and is only observed in certain conditions.54, 55, 56 While high intensity energy may yield superior treatment effects with single sessions, it often accompanies increased pain and local swelling, necessitating local anesthesia, which may compromise efficacy. Further studies are needed to evaluate the optimal energy level for ESWT in various clinical settings.
ESWT can be categorized into two types: focused-ESWT and radial-ESWT, which differ in their physical properties and patterns of acoustic wave propagation. Many included studies have not specified which type was utilized, overlooking this distinction, even though comparisons of the two types have been widely explored in other conditions.57, 58, 59, 60 Each modality has shown different advantages for various diseases, resulting in inconclusive outcomes. Importantly, no study has directly compared f-ESWT and r-ESWT in hand surgical conditions.
Future directions for ESWT research should prioritize standardizing treatment protocols to enhance patient experience and cost-effectiveness, as current practices vary widely based on physician preference.61 One key limitation across the included studies is the lack of follow-up data on subsequent treatments following ESWT. There is little to no mention in most studies regarding whether patients eventually required surgery or alternative interventions, making it difficult to assess the long-term effectiveness of ESWT in preventing disease progression or reducing the need for invasive management. This is particularly relevant for CTS and trigger finger, where some patients may experience only temporary relief with ESWT before progressing to more definitive treatments. Additionally, there is a pressing need for standardization in reporting shockwave parameters to improve reproducibility and interpretation of study findings in musculoskeletal disorders.62 Treatment guidelines should differentiate between various forms of therapy, systems, and protocols, rather than treating shockwave therapy as a universal approach.
The application of ESWT in several hand surgical conditions remains understudied, with a notable absence of high-quality research in areas such as flexor tendon injury, de Quervain’s tenosynovitis, Dupuytren’s disease, and hypertrophic hand scars. In flexor tendon injuries, which are typically managed surgically, ESWT may serve as an adjunct to enhance tendon healing, reduce adhesions, and improve tendon gliding. Similarly, its anti-fibrotic and regenerative properties could offer therapeutic benefit in Dupuytren’s disease and hypertrophic scars, while its analgesic and anti-inflammatory effects may be valuable in de Quervain’s tenosynovitis.63^,^64 Future studies should therefore prioritize well-designed, multicenter randomized controlled trials with adequate power and a minimum of 12 months’ follow-up, incorporating both clinical and patient-reported outcomes. In addition, direct comparisons of radial versus focused ESWT are warranted to clarify their relative safety and efficacy in hand surgery applications, as this distinction remains unexplored in the current literature.
Acknowledging the inherent limitations, this systematic review is faced with several notable challenges. Primarily, the included studies exhibit a considerable risk of bias and present their findings in a heterogeneous manner, thereby hindering the establishment of robust and directly comparable conclusions. Furthermore, the predominant focus on western and developed nations within the reviewed literature restricts the extrapolation of results to low-resource settings. Moreover, the variability in delivery protocols poses a significant obstacle to the feasibility of conducting comprehensive comparative or network meta-analyses. The significance of this review lies in consolidating an otherwise fragmented body of literature and outlining a clear research agenda. Our synthesis demonstrates that, although ESWT shows encouraging short-term benefits in soft tissue conditions of the hand, its definitive role within management pathways remains unresolved. Notably, evidence with follow-up beyond three months is limited to only five conditions: scaphoid wrist nonunions, carpal tunnel syndrome (CTS), Dupuytren’s disease, trigger finger, and post-CTRS pillar pain, leaving its long-term efficacy in other hand pathologies unknown. For ESWT to progress beyond an experimental adjunct and achieve recognition as a validated component of evidence-based hand surgery, future research must address the methodological limitations we have identified.
Conclusion
Standardization of shockwave therapy frequency and intensity is essential. Although there is an abundance of evidence supporting the use of ESWT in CTS, the overall quality of that evidence remains questionable. Dose-dependent effect remains a possibility but requires further investigation. ESWT demonstrates noteworthy short-term efficacy and is primarily used as an adjunct treatment. Although the literature on CTS is well-developed, meticulously designed RCTs are necessary to further evaluate its efficacy in other hand surgical conditions.
Funding
No funding was required for this study.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki. The study was exempt from IRB review was no confidential patient information was involved.
Authors’ contributions
All authors approve the final version of the manuscript, including the authorship list and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted. No writing assistance was obtained in the preparation of the manuscript. The manuscript, including related data, figures and tables has not been previously published and that the manuscript is not under consideration elsewhere.
Declaration of competing interest
All authors have no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Geoghegan L.Carolina M.French J.Harrison C.J.Rodrigues J.N.Health-related quality of life in patients with conditions affecting the hand: meta-analysis Br J Surg 1114202410.1093/bjs/znae 067PMC 1100352738593043 · doi ↗ · pubmed ↗
- 2Chaudhary R.Khanna J.Bansal S.Bansal N.Current insights into carpal tunnel syndrome: clinical strategies for prevention and treatment Curr Drug Targets 202410.2174/011389450128033124021306333338385490 · doi ↗ · pubmed ↗
- 3Mani-Babu S.Morrissey D.Waugh C.Screen H.Barton C.The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review Am J Sports Med.433201575276110.1177/036354651453191124817008 · doi ↗ · pubmed ↗
- 4Weninger P.Thallinger C.Chytilek M.Extracorporeal shockwave therapy improves outcome after primary anterior cruciate ligament reconstruction with hamstring tendons J Clin Med 1210202310.3390/jcm 12103350 PMC 1021904337240456 · doi ↗ · pubmed ↗
- 5Auersperg V.Trieb K.Extracorporeal shock wave therapy: an update EFORT Open Rev 510202058459210.1302/2058-5241.5.19006733204500 PMC 7608508 · doi ↗ · pubmed ↗
- 6Ryskalin L.Morucci G.Natale G.Soldani P.Gesi M.Molecular mechanisms underlying the pain-relieving effects of extracorporeal shock wave therapy: a focus on fascia nociceptors Life (Basel)125202210.3390/life 12050743 PMC 914651935629410 · doi ↗ · pubmed ↗
- 7de Lima Morais T.M.Meyer P.F.de Vasconcellos L.S.Effects of the extracorporeal shock wave therapy on the skin: an experimental study Lasers Med Sci 342201938939610.1007/s 10103-018-2612-830109536 · doi ↗ · pubmed ↗
- 8Simplicio C.L.Purita J.Murrell W.Santos G.S.Dos Santos R.G.Lana J.Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine J Clin Orthop Trauma 11Suppl 32020 S 309s 31810.1016/j.jcot.2020.02.00432523286 PMC 7275282 · doi ↗ · pubmed ↗