Beyond the Usual Suspects: Unlocalizable Back Pain After Trauma
Julia Isaacson, Jennifer Frush, Andrew Mittelman

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
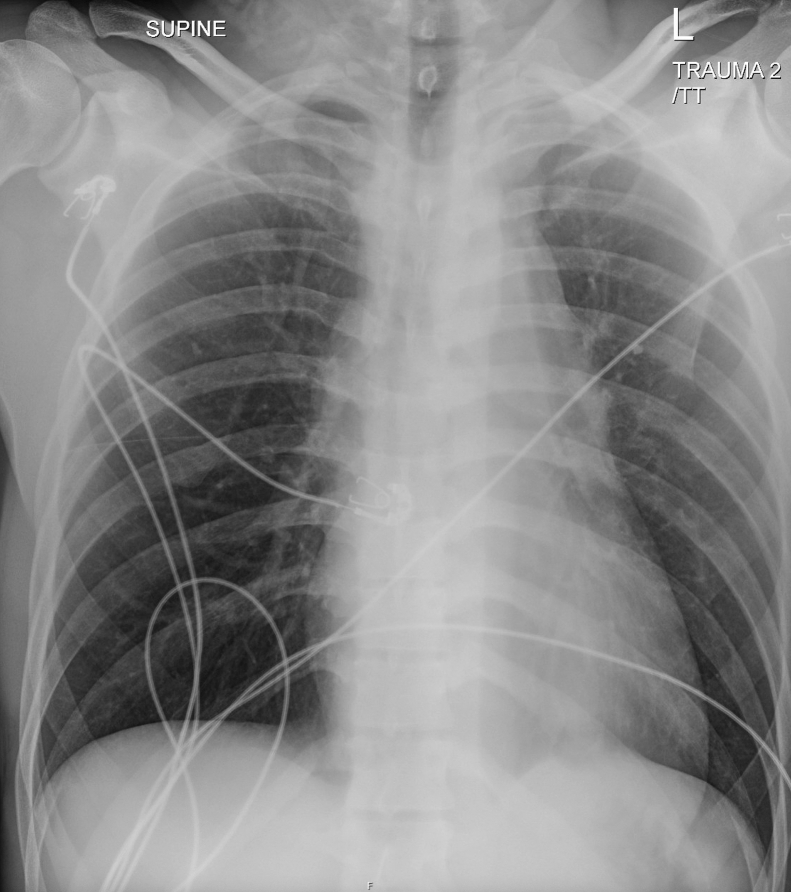 Figure 1
Figure 1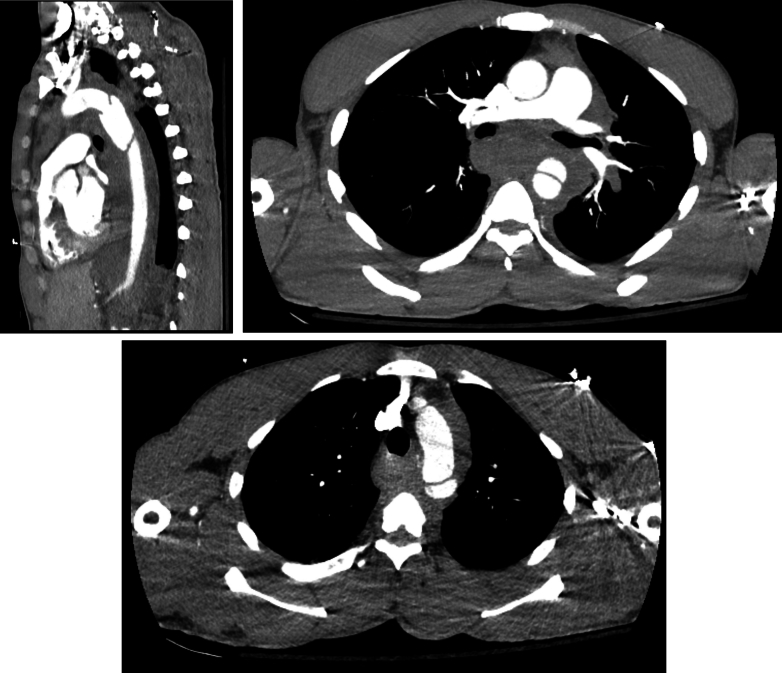 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Pain Management and Treatment · Spine and Intervertebral Disc Pathology
Case Presentation
1
A previously healthy 38-year-old man presented with severe back pain after jumping from a third-story window. He reported a head strike but denied loss of consciousness and was ambulatory at the scene. On arrival, he was alert but uncomfortable. His airway was intact, lungs were clear, and he was hemodynamically stable. A secondary survey revealed minor abrasions and lacerations. No midline spinal tenderness or step offs were noted. Peripheral pulses were intact, and there were no motor or sensory deficits. His eFAST was negative. A portable chest x-ray (Fig 1) and a computed tomography (CT) of the chest, abdomen, and pelvis (Fig 2) were obtained.Figure 1. Chest radiograph demonstrating mediastinal widening and loss of the aortic knob.Figure 2. Contrast-enhanced CT of chest, abdomen, and pelvis revealing descending thoracic aortic pseudoaneurysm with an intimal flap, extensive hemomediastinum, and anterior heart displacement.
Diagnosis
2
Traumatic Aortic Dissection
2.1
An esmolol infusion was started in the emergency department, and the patient underwent emergent thoracic endovascular aortic repair. He was discharged to rehabilitation one week later without any major complications.
Teaching Points
2.2
Traumatic aortic injury is rare, occurring in <1% of blunt trauma cases, but is highly lethal, with up to 85% of patients dying at the scene.1 It is the second leading cause of death in blunt trauma behind traumatic brain injury. CT angiography is the diagnostic modality of choice, with sensitivity and specificity approaching 100%.2 In contrast, chest radiography—used to assess for indirect signs of aortic injury such as mediastinal widening—has low sensitivity (∼40%). Traumatic aortic injury grades II to IV generally require operative repair, and endovascular approaches are typically preferred.3
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harper C.Collier S.A.Slesinger T.L.Traumatic aortic injuries Stat Pearls Published 2024 Stat Pearls Publishinghttps://www.ncbi.nlm.nih.gov/books/NBK 555980/32310440 · pubmed ↗
- 2D’Souza D, Campos A, Elfeky M, et al. Thoracic aortic injury. In: Radiopaedia.org [Internet]. Reference article; revised December 26, 2024. Accessed July 21, 2025. 10.53347/r ID-2171 · doi ↗
- 3Gang Q.Lun Y.Pang L.Traumatic aortic dissection as a unique clinical entity: a single-center retrospective study J Clin Med 12242023753510.3390/jcm 1224753538137605 PMC 10744057 · doi ↗ · pubmed ↗