Salivary fluoride bioavailability after application of fluoride varnishes: A randomized clinical study
Maria Suzi de Sousa Lopes, Lyzia Vitoria Mendes Rezende, Evanildo Canuto Paz, Glauber Campos

TL;DR
This study found that Duraphat® fluoride varnish increases salivary fluoride levels more effectively than Fluorniz, with higher concentrations lasting longer.
Contribution
The study provides new empirical evidence comparing the bioavailability of two fluoride varnishes in different salivary compartments over time.
Findings
Duraphat® increased salivary fluoride concentrations significantly higher than Fluorniz up to 48 hours post-application.
Fluorniz returned to baseline fluoride levels 8 hours after application, while Duraphat® took 24 hours.
Fluoride concentrations in the sediment were higher than in the supernatant for both varnishes.
Abstract
This study aimed to evaluate the bioavailability of F in saliva compartments (sediment and supernatant) after the use of fluoride varnishes (FV) with 5% sodium fluoride. In this randomized two-phase crossover clinical study, 15 participants were allocated into two groups and received application of Duraphat® and Fluorniz on the vestibular surface of the teeth. Unstimulated saliva was collected before the application of the FV, and 5 min, 15 min, 30 min, 1 h, 2 h, 4 h, 8 h, 12 h, 24 h, 48 h, and 96 h after application. For statistical analysis, a t-test was performed to compare the FV in the salivary compartments. The F in saliva at different times was compared with the baseline using analysis of variance, with Dunnett’s post hoc test for multiple comparisons. After application, the F concentration in the salivary compartments increased (p < 0.001) and returned to baseline 24 h after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
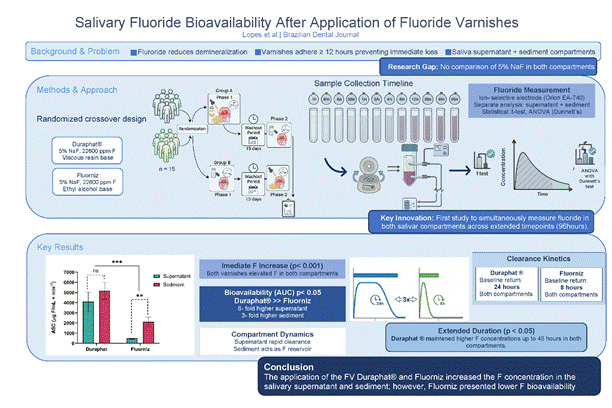 Figure 1
Figure 1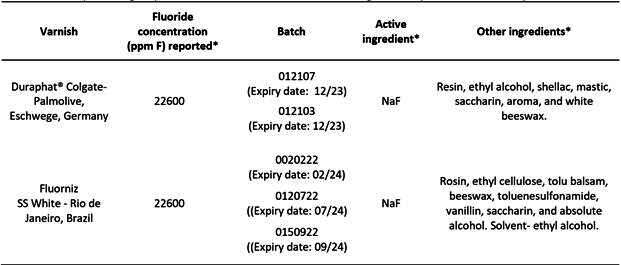 Figure 2
Figure 2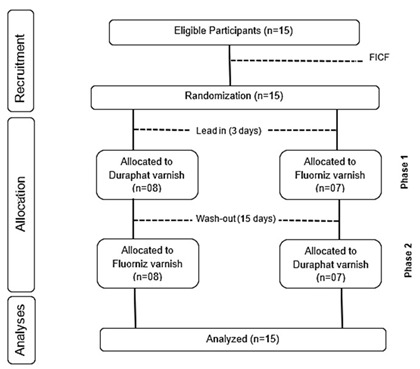 Figure 3
Figure 3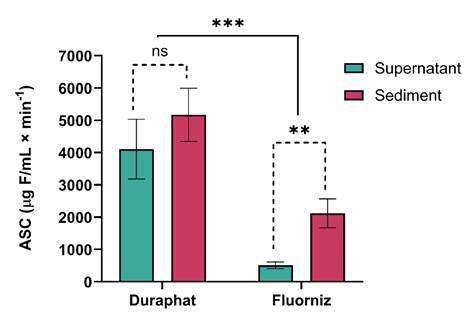 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Fluoride Effects and Removal · Dental Erosion and Treatment
Introduction
The use of fluorides (F) remains the most effective strategy for controlling dental caries at both individual and population levels1. Their action is physicochemical, reducing demineralization and enhancing remineralization of enamel and dentin2. For this, F must be continuously available in the oral environment at low but constant concentrations (0.02-0.05 ppm F)3. Oral reservoirs, such as biofilm, soft tissues, the tongue, calcium fluoride (CaF₂) formed on enamel, and saliva, maintain transient increases in fluoride levels, followed by clearance through swallowing and salivary secretion4. Importantly, fluoride must be free or soluble in the aqueous phase of the oral cavity (biofilm fluid or saliva) to exert its preventive effect5.
Fluoride bioavailability in saliva depends on the mode of administration, formulation solubility, concentration, and salivary flow6 ^,^ 7. Studies with dentifrices demonstrate that higher product concentrations yield proportionally greater fluoride levels in saliva8. Consequently, patients at high caries risk benefit from products that maintain elevated fluoride concentrations, such as professionally applied gels and fluoride varnishes (FV)3. FV were designed to extend the contact time between F and enamel by adhering to the tooth surface as a thin film for more extended periods (≥12 h), preventing immediate loss of fluoride9 ^,^ 10. Interaction with saliva leads to the formation of calcium fluoride (CaF₂) on the enamel surface, stabilized by pellicle proteins and phosphate at neutral pH. Under acidic conditions, CaF₂ dissolves, releasing F and acting as a sustained source11 ^,^ 12. Therefore, the persistence of salivary fluoride depends on product formulation, application method, and elimination rate13.
The use of FV is effective in reducing the prevalence and severity of caries in high-risk populations, in primary and permanent dentitions, and should be applied two to four times a year14. FV are widely accepted due to their ease of application, rapid setting, and high safety, with no reported short-term adverse effects15 ^,^ 16. Previous studies have mainly assessed fluoride concentrations in the salivary supernatant after FV application12 ^,^ 17 ^,^ 18. However, whole saliva comprises two compartments: supernatant and sediment19. The sediment contains organic material (bacteria, epithelial cells, proteins) and inorganic ions, including fluoride20 ^,^ 21, while the supernatant consists primarily of water and electrolytes22 ^,^ 23 ^,^ 24. Although bioavailable fluoride corresponds to the free ions in the supernatant, the sediment may act as a reservoir capable of binding and gradually releasing fluoride, contributing to its long-term availability25.
Several FV formulations are available, including those with added calcium phosphates such as casein phosphopeptide-amorphous (ACP)26 and tricalcium (TCP)27, and others containing only 5% sodium fluoride (NaF), such as Duraphat®28 and Fluorniz29. A 5% NaF FV remains the gold standard for preventing or reversing non-cavitated lesions in both dentitions30. Previous studies compared FV with other topical products and observed higher fluoride concentrations and longer retention in saliva after FV application12. Nevertheless, no studies have simultaneously compared different 5% NaF varnishes, evaluating fluoride release in both salivary compartments (supernatant and sediment) to distinguish free and bound fluoride fractions. Therefore, this study aimed to evaluate the bioavailability of fluoride in the salivary supernatant and sediment following the application of 5% NaF fluoride varnishes.
Materials and methods
Ethical aspects
This study was approved by the Research Ethics Committee of the Federal University of Piauí (opinion 5543818). The participants signed the Free and Informed Consent Form (FICF), in accordance with Resolution No. 466 of the National Health Council, Ministry of Health, Brasília, DF, 12/12/2012, and received verbal and written information with guidelines about the research. This study followed the ethical principles originating from the Declaration of Helsinki and adopted the CONSORT 2010 Statement as a reporting framework for randomized clinical trials. The trial was prospectively registered in the Brazilian Clinical Trials Registry (RBR-8974jb6), and no deviations or amendments occurred between the registered protocol and the final manuscript.
Pilot study
The pilot study was conducted with six participants distinct from those included in the main trial, for the purpose of determining collection times, standardization, and procedural adjustments.
FV and toothpaste
Two commercially available FVs were tested: Duraphat® (Colgate-Palmolive, Eschwege, Germany) and Fluorniz (SS White, Rio de Janeiro, Brazil), both containing 5% NaF or 22,600 ppm F. Condor Baby toothpaste (Condor, SC, Brazil) without F was also used in the study (Box 1).
Box 1Description of groups, fluoride content of varnishes and ingredients present in the composition.*Informed by the manufacturer. NaF = Sodium Fluoride
Recruitment
The participants invited to participate in the study were undergraduate or graduate students in Dentistry at UFPI. After agreeing to participate in the study, they were assessed according to the inclusion criteria, such as having unrestored vestibular surfaces of the teeth, the absence of active carious lesions, and normal salivary flow. To assess salivary flow, a millimeter-sized tube was made available for unstimulated saliva collection, using the spitting technique, and the total sample obtained was assessed. If the participant managed to collect 2 mL of saliva in 2 min, they were included in the study28. Although the inclusion criterion of 2 mL in 2 min may be higher than the average unstimulated flow rate, it was based on pilot data confirming normal flow in our study population (mean 1.1 mL/min), consistent with reference physiological ranges22. In turn, participants who used medications that alter salivary flow, used F supplements, smoked, had periodontal disease, had fixed orthodontic appliances, were allergic or sensitive to the ingredients of the FV used in the study, or had received FV in the last 3 months were excluded from the study. Before the stages were carried out, the participants were seen at a clinic and assessed according to the inclusion criteria and salivary flow rate.
The sample size calculation was performed using G*Power software, version 3.1.9.7 (Heinrich Heine University, Düsseldorf, Germany). It was based on the primary outcome, fluoride concentration (µg F/mL) in the salivary supernatant, derived from pilot data comparing fluoride varnishes at 48 hours post-application, which represented the smallest difference observed between groups. An alpha error of 5% and a beta error of 10% were considered, resulting in a total sample of 15 participants and an actual statistical power of 0.92.
Experimental design
This randomized, crossover, double-blind clinical study was conducted with 15 adults living in a municipality with a fluoridated public water supply. During two experimental phases, the participants were randomly allocated into two groups and received two types of treatments: Duraphat® and Fluorniz. Group A (n=8) received Duraphat® in Phase 1 and Fluorniz in Phase 2, whereas Group B (n=7) received the reverse order. The FV was applied to the vestibular surface of the upper and lower teeth, with the exception of the third molar. The randomization of the subjects, the application of the FV, and preparation of the samples were performed by the same individual who knew the type of FV applied. However, the analyses of the saliva samples were performed by a researcher who was unaware of this information. Before the beginning of the experimental phases, the participants used non-fluoridated toothpaste for 3 days (lead-in), and between phases, they used the same toothpaste for 15 days (washout). The flowchart of the experiment is shown in Figure 1.
Figure 1. Flowchart of the experimental design of the study.
Application of the FV
The FV was applied by a single professional, according to the manufacturer's instructions. The participants underwent dental prophylaxis with a pumice stone (SS White) and a Robinson brush (American Burrs, Santa Catarina, Brazil). Duraphat® is presented in a single package, and 2 mL of the product was separated for application. Fluorniz is available in two bottles, one for the varnish and one for the solvent. For the application, a mixture was obtained with the proportion of 1.5 mL of varnish and 0.5 mL of solvent, totaling 2 mL. The amount of each FV was determined with the aid of a disposable syringe. After performing relative isolation and with the teeth dry, the FV were applied to the vestibular surface of all teeth, except the third molars, using a microbrush (KG Korense, São Paulo, Brazil), using 2 mL of product. The participants were instructed to avoid hard foods, not to brush their teeth for the first 24 h, not to consume foods containing F, such as sardines and green tea, and not to eat or drink, with the exception of water, 1 h before any of the saliva collection times. Twenty-four hours after applying the products, the participants were allowed to brush their teeth with the toothbrush and fluoride-free toothpaste provided by the researcher.
The randomization sequence was generated by an independent researcher using Microsoft Excel and stored in a password-protected file. Allocation concealment was ensured using sealed, opaque, sequentially numbered envelopes, which were opened only at the time of varnish application. The independent researcher who generated the sequence was not involved in participant enrollment or intervention. The participants were blinded regarding the order of FV application and name; however, due to the uniqueness of each varnish (flavor, color, and adhesion), the participants had the potential to discriminate between the FV. However, no participant reported curiosity in discovering the FV that had been applied.
Sample collection
Unstimulated saliva collection, using the spitting technique, was performed before the application of the FV (baseline), and then 5 min, 15 min, 30 min, 1 h, 2 h, 4 h, 8 h, 12 h, 24 h, 48 h, and 96 h after application. The participant collected the saliva in a plastic tube for a maximum of 4 min at each collection time, with an approximate quantity of 3 mL. After collection, each plastic tube was stored at -20 °C until analysis28.
Determination of the salivary F concentration
A specific electrode (model 18AF-001, Analyser Instrumentação Análise, São Paulo, SP, BR) coupled to an ion analyzer (Orion EA-740) was used to measure the salivary F concentration. Aliquots (1 mL) of the thawed samples were collected and centrifuged for 3 min. Then, 0.5 mL of the salivary supernatant was buffered with 0.05 mL of TISAB III (06). The F concentration was calculated by linear regression of two calibration curves, obtained from F concentration standards. The samples collected 5 min, 15 min, 30 min, 1 h, 2 h, and 4 h after application were evaluated with the high-concentration curve using the 0.25-32 ppm F standards. The samples collected at baseline and 8, 12, 24, 48, and 96 h after application were evaluated with the low-concentration curve using the 0.0625-2.0 ppm F standards.
The salivary supernatant remaining after the first analysis was discarded, leaving only the sediment. Aliquots (0.5 mL) of TISAB II were added to the sediment and stirred for 10 s in a vortex mixer (Nova Instrumentos, Piracaba, SP, BR)21. The suspension was analyzed to determine the F concentration using a specific electrode (model 18AF-001, Analyser Instrumentação Análise) coupled to an ion analyzer (Orion EA-740), in a similar manner to that performed for the salivary supernatant.
Statistical analysis
The Shapiro-Wilk test was used to determine whether the data followed a normal distribution. It revealed the non-normal distribution of the data. Thus, the data were log10 transformed and evaluated with the t-test for comparisons of the two FV at each collection time, in the salivary supernatant and sediment. The salivary F concentrations after application of the FV at the different time intervals were compared with the baseline concentration using analysis of variance with Dunnett’s post hoc test for multiple comparisons. The descriptive statistical data are presented as graphs and tables, and GraphPad Prism 9.51 (GraphPad, La Jolla, CA, USA) was used for analysis.
Results
There was no difference in the salivary F concentration at baseline between the two FV (p > 0.05). Table 1 shows the F concentration in the salivary supernatant and sediment at different times after application of the FV. Immediately after the application of both FV, the F concentration in the salivary supernatant and sediment increased significantly (p < 0.001), and decreased at all other times, returning to baseline 24 h after application in the Duraphat® group, and 8 h after application in the Fluorniz group. When comparing the salivary sediment and supernatant between the groups, there was a difference between the Duraphat® and Fluorniz FV up to 48 h after application, with a higher salivary F concentration in the Duraphat® group compared with the Fluorniz group.
Table 1. Salivary fluoride concentration (Mean ± SD, µg F/mL) in the supernatant or salivary sediment after application of the varnishes evaluated.TimeSupernatant p-value Sediment p -valueDuraphat ®Fluorniz Duraphat ®Fluorniz baseline0.02 ± 0.010.03 ± 0.020.0590.14 ± 0.040.12 ± 0.020.1035 min122.63 ± 106.66 ^α^ 13.03 ± 8.82 ^α^ <0.00135.72 ± 17.36 ^α^ 8.97 ± 7.45 ^α^ <0.00115 min28.21 ± 11.61 ^α^ 4.68 ± 4.95 ^α^ <0.00115.26 ± 8.95 ^α^ 5.93 ± 4.18 ^α^ 0.00330 min18.50 ± 10.52 ^α^ 1.90 ± 1.84 ^α^ <0.0019.84 ± 4.99 ^α^ 4.44 ± 3.67 ^α^ 0.0041 h12.40 ± 8.21 ^α^ 0.94 ± 0.81 ^α^ <0.0019.79 ± 4.13 ^α^ 3.75 ± 2.92 ^α^ 0.0032 h7.00 ± 5.22 ^α^ 0.51 ± 0.49 ^α^ <0.0017.85 ± 3.74 ^α^ 1.79 ± 1.79 ^α^ <0.0014 h2.46 ± 2.34 ^α^ 0.29 ± 0.29 ^α^ <0.0014.65 ± 3.21 ^α^ 1.17 ± 1.21 ^α^ <0.0018 h1.14 ± 1.42 ^α^ 0.08 ± 0.06 ^α^ <0.0012.23 ± 1.76 ^α^ 0.58 ± 0.52 ^α^ 0.00112 h0.41 ± 0.65 ^α^ 0.04 ± 0.03<0.0010.83 ± 0.63 ^α^ 0.39 ± 0.22 ^α^ 0.02424 h0.18 ± 0.25 ^α^ 0.04 ± 0.050.0430.54 ± 0.31 ^α^ 0.33 ± 0.300.01648 h0.04 ± 0.040.03 ± 0.010.0160.31 ± 0.200.19 ± 0.130.00296 h0.02 ± 0.010.02 ± 0.010.1950.22 ± 0.190.18 ± 0.120.325indicate a statistical difference between the two varnishes at each collection time in the salivary compartments evaluated. α indicatesthe observation period in which F concentrations are higher than the baseline after Dunnett's multiple comparisons test (p < 0.05)
Comparison of the salivary components of each group (Table 2) revealed that after application of Duraphat®, there was a difference in the F concentration at all times, except for 1 and 2 h (p > 0.05). The salivary F concentration was significantly higher in the supernatant compared with the sediment up to 30 min after application, and from 4 h onwards, the concentrations were higher in the salivary sediment (p < 0.05). With the use of Fluorniz, only 5 and 15 minutes after application did not present differences. The F concentration was higher in the salivary sediment (p < 0.001).
Table 2. Salivary fluoride concentration (Mean ± SD, µg F/mL) after application of Duraphat and Fluorniz varnishes in the salivary compartments evaluated.TimeDuraphat ® p-value Fluorniz p -valueSupernatantSediment SupernatantSediment baseline0.02 ± 0.010.14 ± 0.04<0.0010.03 ± 0.020.12 ± 0.02<0.0015 min122.63 ± 106.6635.72 ± 17.36<0.00113.03 ± 8.828.97 ± 7.450.08215 min28.21 ± 11.6115.26 ± 8.950.0014.68 ± 4.955.93 ± 4.180.07730 min18.50 ± 10.529.84 ± 4.990.0041.90 ± 1.844.44 ± 3.67<0.0011 h12.40 ± 8.219.79 ± 4.130.9960.94 ± 0.813.75 ± 2.92<0.0012 h7.00 ± 5.227.85 ± 3.740.2210.51 ± 0.491.79 ± 1.79<0.0014 h2.46 ± 2.344.65 ± 3.210.0170.29 ± 0.291.17 ± 1.21<0.0018 h1.14 ± 1.422.23 ± 1.760.0120.08 ± 0.060.58 ± 0.52<0.00112 h0.41 ± 0.650.83 ± 0.630.0010.04 ± 0.030.39 ± 0.22<0.00124 h0.18 ± 0.250.54 ± 0.31<0.0010.04 ± 0.050.33 ± 0.30<0.00148 h0.04 ± 0.040.31 ± 0.20<0.0010.03 ± 0.010.19 ± 0.13<0.00196 h0.02 ± 0.010.22 ± 0.19<0.0010.02 ± 0.010.18 ± 0.12<0.001**indicate statistical difference between salivary compartments in each varnish studied (p < 0.05).
Figure 2 shows the area under the curve (AUC) of the salivary F concentration over time. The treatments differed significantly from each other, with higher F bioavailability in the salivary supernatant and sediment after the use of Duraphat® compared with Fluorniz (p < 0.05). The F concentration in the salivary supernatant and sediment after the use of Duraphat® did not present a difference (p > 0.05). However, there was a significant difference between the salivary compartments for Fluorniz, with a higher F concentration in the sediment (p < 0.05).
Table 3 shows the ratio between the average F concentration in the salivary sediment and supernatant after application of the FV. With Duraphat®, only at 5 min, 15 min, 30 min, and 1 h after application was there a higher F concentration in the supernatant compared with the sediment, while in the Fluorniz group, the F concentration was higher in the supernatant only at 5 min after application. At other times, in both groups, the ratio of the salivary compartments showed increasing behavior, even 96 h after application, identifying a higher F concentration in the salivary sediment.
Table 3. Proportion of mean values of fluoride concentration in the sediment to mean fluoride values in the salivary supernatant in the varnishes evaluated.VarnishTime Baseline5 min15 min30 min1 h2 h4 h8 h12 h24 h48 h96 hDuraphat ®8.970.29^^ 0.54^^ 0.53^^ 0.79^^ 1.121.891.952.033.076.959.91Fluorniz4.750.69^^ 1.272.333.983.494.027.158.697.367.299.77 indicate higher fluoride concentration in the supernatant than in the sediment.
Figure 2. Mean area under the curve (AUC) of salivary F concentration as a function of time (μg F/mL.min ^-1^) according to treatments (n = 16). ^ns^ indicates non-significant difference (p > 0.05), **indicates statistical difference between the salivary compartments for Fluorniz varnish (p < 0.05). ***indicates statistical difference between the two varnishes for both salivary compartments (p < 0.05). The vertical bars indicate the standard deviation.
Discussion
This clinical study is the first to evaluate two FVs with similar fluoride concentrations (5% NaF; 22,600 ppm F), Duraphat® and Fluorniz, by monitoring fluoride levels in both salivary supernatant and sediment over time. Although these varnishes share the same nominal fluoride concentration, they differ in formulation and physicochemical properties, which significantly influence fluoride bioavailability. Both products increased fluoride concentrations in saliva; however, Duraphat® maintained markedly higher levels in both compartments throughout the evaluation period. Similar differences among NaF-based varnishes have been reported previously18, reinforcing that formulation characteristics play a critical role in fluoride release and retention.
Previous studies have primarily examined fluoride concentrations in the salivary supernatant, neglecting the sediment fraction12 ^,^ 18. The present results confirm that the fluoride clearance pattern differs between these compartments. The more rapid decline observed in the supernatant may reflect the immediate dilution and swallowing of soluble fluoride, whereas ions bound to components of the salivary sediment are released more slowly21. Consequently, the sediment, in addition to the oral soft tissues, recognized reservoirs of fluoride retention31, appears to act as a slow-release reservoir, extending fluoride availability in the oral environment21.
Duraphat® demonstrated higher fluoride levels in the supernatant up to one hour after application, followed by predominance in the sediment, while Fluorniz showed a brief peak at five minutes before a faster decline. These findings indicate formulation-dependent dynamics: lower-viscosity products, such as Fluorniz, exhibit reduced adhesion to tooth surfaces and greater diffusion away from the site of application, leading to more rapid clearance and possible partial ingestion before complete fluoride release18. Conversely, Duraphat®, with its more viscous resin base, retains fluoride longer, favoring gradual ion diffusion and sustained salivary fluoride concentrations.
In both products, peak fluoride levels occurred five minutes after application, followed by a progressive decrease. Duraphat® maintained concentrations above baseline for up to 24 h, while Fluorniz returned to baseline within 8-12 h in the supernatant and sediment, respectively. These findings are consistent with previous studies showing that fluoride levels increase immediately after FV application but generally return to baseline within 24 h12 ^,^ 18 ^,^ 28 ^,^ 32. This period coincides with the peak formation of calcium fluoride (CaF₂) on enamel surfaces33, suggesting that after 24 h, most fluoride remains bound to enamel rather than freely circulating in saliva.
When comparing overall fluoride bioavailability, Duraphat® exhibited approximately eightfold higher concentrations in the supernatant and threefold higher in the sediment than Fluorniz. These differences are attributed to compositional and rheological variations. Duraphat® contains a natural resin base with a small proportion of alcohol and chitosan, enhancing viscosity and reducing wettability, which promotes prolonged fluoride retention and slower ion diffusion34. In contrast, Fluorniz, supplied in two separate components (varnish and solvent), contains ethyl alcohol that increases fluidity and volatility, facilitating rapid evaporation and fluoride loss29 ^,^ 35. The higher viscosity and cohesive structure of Duraphat® likely explain its superior fluoride bioavailability and clinical effectiveness.
Salivary fluoride levels are directly related to the amount of fluoride available to interact with enamel surfaces36. Continuous exposure to low concentrations of fluoride in saliva and biofilm fluid is critical to counteracting demineralization by promoting fluorapatite formation and facilitating remineralization through calcium and phosphate deposition1. Several studies have confirmed that FV maintains salivary fluoride at effective levels for extended periods, reduces lesion depth, and enhances enamel remineralization compared with other topical fluoride products12 ^,^ 35 ^,^ 37.
As highlighted by Marinho et al. 201314, FV application to either primary or permanent teeth substantially reduces caries progression. This efficacy derives from the ability of varnishes to sustain contact between fluoride and enamel in a thin, adherent film for ≥12 h, minimizing loss through swallowing and acting as a long-term fluoride reservoir9. During this period, fluoride ions from the varnish dissolve into saliva, are absorbed by oral reservoirs, including enamel, plaque, and soft tissues, and are gradually re-released, combining with calcium to form CaF₂. These reservoirs dissolve slowly, releasing fluoride ions that provide ongoing protection against caries38.
The ratio of fluoride concentration between sediment and supernatant increased over time for both varnishes. In Duraphat®, fluoride levels were initially higher in the supernatant (ratio < 1) up to 1 h post-application, shifting to predominance in the sediment thereafter (ratio > 1). For Fluorniz, this shift occurred after only 5 min. These dynamics further support the role of salivary sediment as a retention compartment and the superior persistence of fluoride derived from Duraphat®. Santos et al. 200935 found similar results in vitro, showing that Duraphat® reduced lesion depth by 58%, compared with 35% for Fluorniz, reinforcing the greater potential of more viscous formulations to maintain fluoride in the oral cavity and enhance anticariogenic effects.
The dual-compartment analysis applied in this study reflects the pharmacokinetic behavior of fluoride in a semi-homeostatic system such as saliva, which is influenced by interindividual differences in flow, biochemical composition, and microbial activity6. We acknowledge that variation in sample collection times, particularly those performed at night when salivary flow is reduced39, may have affected fluoride concentration measurements. Nonetheless, this limitation does not alter the overall trends observed. Finally, although cost was not the primary focus of this study, our findings have clinical implications for product selection in public health programs. Despite its lower price, Fluorniz exhibited substantially lower fluoride bioavailability than Duraphat®, emphasizing that formulation characteristics and not only cost should guide the choice of fluoride varnish in preventive protocols40.
Conclusion
The application of the FV Duraphat® and Fluorniz increased the F concentration in the salivary supernatant and sediment; however, Fluorniz presented lower F bioavailability. Therefore, the F concentration in the product is not the only factor influencing salivary fluoride bioavailability. This study introduces a novel approach by evaluating fluoride bioavailability in the salivary sediment, highlighting its role as a potential reservoir for slow fluoride release, contributing to prolonged fluoride presence in the oral cavity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tenuta LM Cury JA Fluoride: its role in dentistry Braz Oral Res 2010249172085707010.1590/s 1806-83242010000500003 · doi ↗ · pubmed ↗
- 2Featherstone JDB Prevention and reversal of dental caries: role of low level fluoride Community Dent Oral Epidemiol[Internet]19992731401008692410.1111/j.1600-0528.1999.tb 01989.x · doi ↗ · pubmed ↗
- 3O'Mullane DM Baez RJ Jones S Lennon MA Petersen PE Rugg-Gunn AJ Whelton H Whitford GM Fluoride and Oral Health Community Dent Health 201633699927352462 · pubmed ↗
- 4Duckworth RM Morgan SN Oral fluoride retention after use of fluoride dentifrices Caries Res 199125123129205997310.1159/000261354 · doi ↗ · pubmed ↗
- 5Issa AI Toumba KJ Oral fluoride retention in saliva following toothbrushing with child and adult dentifrices with and without water rinsing Caries Res 20043815191468497210.1159/000073915 · doi ↗ · pubmed ↗
- 6Naumova EA Kuehnl P Hertenstein P Markovic L Jordan RA Gaengler P Arnold WH Fluoride bioavailability in saliva and plaque BMC Oral Health 201212310.1186/1472-6831-12-3PMC 329567822230722 · doi ↗ · pubmed ↗
- 7Duckworth RM Jones S On the relationship between the rate of salivary flow and salivary fluoride clearance Caries Res 2015491411462563416210.1159/000365949 · doi ↗ · pubmed ↗
- 8Vale GC Cruz PF Bohn AC de Moura MS Salivary fluoride levels after use of high-fluoride dentifrice Scientific World Journal 2015201530271710.1155/2015/302717 PMC 436398325821849 · doi ↗ · pubmed ↗