Cohort profile: The Bristol IVF Study- A longitudinal study of women, their partners and treatment outcomes following assisted reproductive technologies
Amy E. Taylor, Taemi Kawahara, Jennifer Provis, Karema Al Rashid, Sophie Fitzgibbon, Alix Groom, Amanda Jefferys, Paul Wilson, Scott M. Nelson, Valentine Akande, Deborah A. Lawlor

TL;DR
The Bristol IVF Study tracks couples undergoing assisted reproductive technologies to understand factors affecting successful pregnancies and birth outcomes.
Contribution
The study provides a comprehensive dataset linking ART treatment with longitudinal health and lifestyle data, enabling novel comparisons with naturally conceived pregnancies.
Findings
The cohort includes 502 couples with detailed data collected before, during, and after ART treatment.
Biological samples and NHS record linkage allow in-depth analysis of ART outcomes and comparisons with natural conception.
Pregnancy and birth data collection followed standardized protocols similar to the ALSPAC-G2 cohort.
Abstract
The Bristol IVF Study (BRIST-IVF) is a longitudinal clinical cohort, established to determine factors related to successful live birth and other outcomes following conception by assisted reproductive technologies (ART). This cohort profile describes recruitment, data collection and planned research. The study gathered comprehensive sociodemographic, lifestyle, anthropometric, and clinical data from women and their partners before and during treatment, as well as during pregnancy and after birth. Biological samples, including blood, urine, and saliva, were collected at initial recruitment and at pregnancy clinics, with cord blood and placental tissue obtained at birth. Participants consented to NHS record linkage, allowing access to pregnancy and birth outcomes from obstetric notes. Data collection during pregnancy and after birth followed the same protocols as a naturally conceived…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
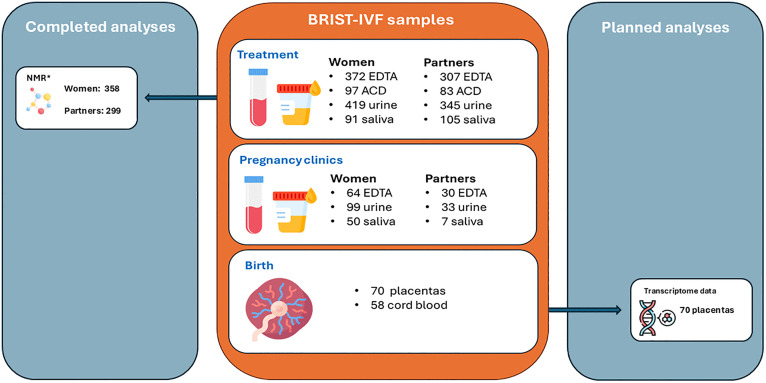 Fig 1
Fig 1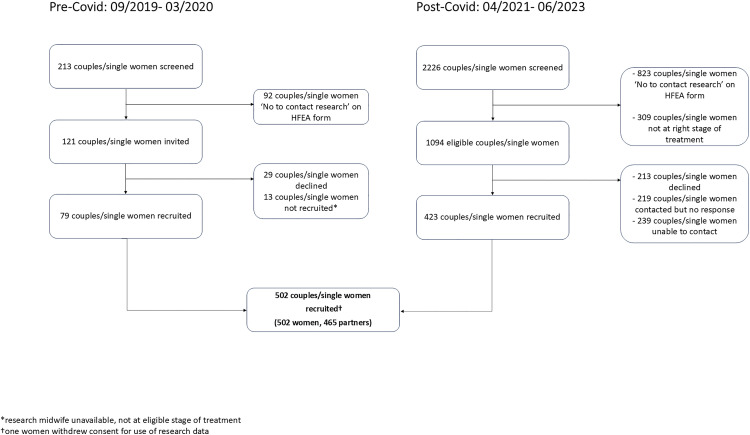 Fig 2
Fig 2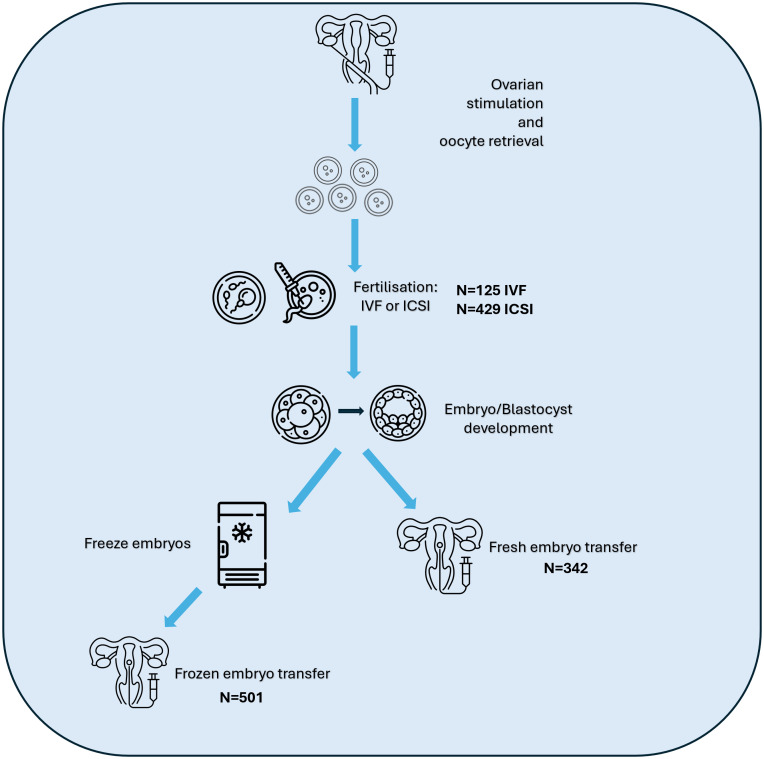 Fig 3
Fig 3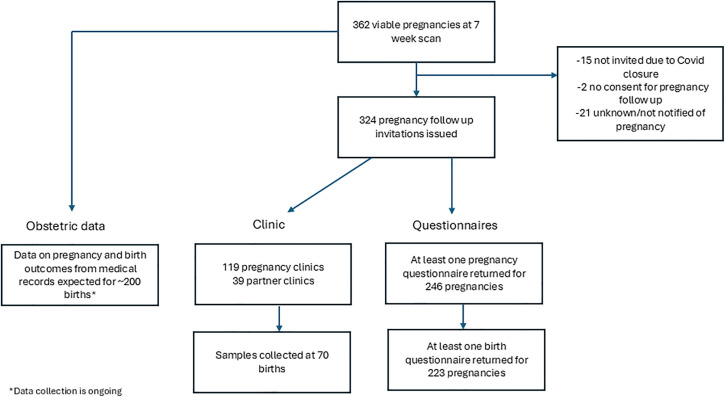 Fig 4
Fig 4- —European Union’s Horizon 2020 research and innovation program
- —NIHR Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust
- —University of Bristol
- —Wellcome Trust and UK Medical Research Council
- —UK Medical Research Council
- —UK Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAssisted Reproductive Technology and Twin Pregnancy · Prenatal Screening and Diagnostics · Reproductive Health and Technologies
Background
Infertility, as defined by the World Health Organization (WHO), is the inability to achieve pregnancy after 12 months or more of regular, unprotected sexual intercourse. It affects roughly one in six couples globally, with lifetime prevalence estimates ranging from 4% to 40%, depending on regional and methodological variations [1]. Although most prevalence data comes from high income countries, estimates from low- to middle-income countries appear broadly comparable [1]. Beyond its biological implications, infertility has profound psychological and social effects, often leading to emotional distress, mental health challenges, and reduced productivity [2].
Assisted reproductive technologies (ART) are effective medical interventions for treatment of infertility. ART refers to all interventions that include the in vitro handling of both human oocytes and sperm or embryos for the purpose of reproduction [3]. The most commonly used forms of ART are in-vitro fertilization (IVF) and IVF with Intracytoplasmic sperm injection (ICSI). Plans for developing the BRIST-IVF cohort began prior to international glossaries clarifying terms for infertility and its treatment. We have retained the study name (BRIST-IVF) and use ART as a general term for IVF and ICSI in this paper.
Globally, ART has resulted in the birth of over 8 million individuals, with the number of ART cycles continuing to rise in high income countries and increasing use in low- and middle- income countries [4]. Identifying modifiable risk factors that influence live birth success and offspring and parental health post conception is essential for improving treatment efficacy. Historically, research on factors associated with ART outcomes has focused on clinical factors that are routinely collected during IVF treatment including maternal age, reproductive history and type of IVF treatment [5,6]. However, increasing evidence suggests that ART outcomes are also influenced by maternal and paternal health and lifestyle characteristics. For example, studies have demonstrated that both maternal and paternal smoking are associated with reduced live birth rates following ART [7,8]. In addition, overweight or obesity in both the females and male partners is associated with reduced likelihood of success in IVF treatment [9,10].
Higher body mass index (BMI) may influence success of IVF treatment via metabolic alterations that affect both oocyte and sperm quality. Advancements in high throughput nuclear magnetic resonance (NMR) spectroscopy now allow profiling of over 200 circulating metabolites in blood serum or plasma [11]. Assessing pre-treatment and/or in treatment metabolite profiles may help identify biomarkers predictive of IVF success and uncover potential pathways for intervention. A recent study of 400 women and their male partners undergoing IVF treatment in Glasgow, UK, identified several novel associations between serum metabolites and markers of ovarian reserve and sperm parameters [12, 13] . These findings highlight the need for further replication and prospective studies to establish metabolic predictors of success.
As live-birth success rates following ART continue to improve, greater attention has been placed on potential perinatal outcomes of ART-conceived offspring. Many studies examining these outcomes have been descriptive, focusing exclusively on ART-conceived individuals without comparison groups or using selective peer-based comparisons. Recent analyses incorporating both conventional population and within sibling comparisons, support a causal effect of fresh-embryo ART transfer compared to natural conception on an increased risk of small for gestational age, while frozen embryo transfer increased the risk of large for gestational age compared to natural conception [14]. Placental tissue DNA methylation and gene expression analyses are also starting to provide critical insights into how ART may influence early developmental programming. DNA methylation regulates gene expression during placental development, which is essential for fetal growth and pregnancy maintenance [15]. ART-conceived pregnancies have been linked to altered placental DNA methylation patterns and gene expression profiles [15,16]. However, more data are required to better understand the specific molecular pathways affected by these expression changes and their potential long-term consequences for offspring health.
While birth cohort and electronic health record studies provide valuable insights into potential effects of any ART compared with natural conception on perinatal and later life offspring and maternal outcomes and increasingly compare different types of ART (e.g., IVF or ICSI, fresh or frozen embryo transfer) they have limited ability to evaluate more detailed treatment variables, such as ovarian stimulation protocols [17–19]. Furthermore, individual birth cohorts often have low numbers of ART pregnancies and electronic health record studies are often not well suited to explore potential molecular mechanisms underlying ART-related outcomes.
To address these gaps, the Bristol IVF Study (BRIST-IVF) was established as a clinical ART cohort to investigate the predictors and causes of live birth success, pregnancy complications, and perinatal outcomes. The initial recruitment target was 1,200 couples or single women and the initial objectives (proposed in 2019) were to**:**
Improve the accuracy of prediction of live birth success with ART;Identify modifiable risk factors and mechanisms that might be targets for developing interventions (lifestyle or clinical) that could improve rates of live birth success;Determine the associations of ART and different ART treatment protocols on fetal epigenetic signals (specifically cord-blood DNA Methylation and potentially histone marks);Determine the impact of ART and different ART treatment protocols on cardio-metabolic risk factors (and their trajectories) in mothers, and partners during the first 5 years after treatment;Determine the impact of ART and different ART treatment protocols on maternal, partner and offspring mental health.
Due to the Covid-19 pandemic, BRIST-IVF was closed for a period of 13 months. After reopening, the shift to initial online clinic visits rather than in-person appointments made it unlikely that the initial recruitment target would be met. As a result, the study was closed earlier than planned as part of the NIHR research and recovery reset programme [20]. The specific impacts of the pandemic on study operations are summarised in Box 1.
The objectives have been revised to reflect the number of participants recruited and the duration of follow-up and we will now focus on two broad objectives:
To investigate determinants of live birth rates following ART, including treatment factors (e.g., protocols) and biological measures (e.g., NMR metabolite measures). This will include replication and/or meta-analysis of findings from the Glasgow IVF Study [13] to validate results and improve generalisability.To compare pregnancy and perinatal outcomes between ART pregnancies and non-ART pregnancies using the Avon Longitudinal Study of Parents and Children (ALSPAC) G2 cohort [21] as a comparison group, and explore the extent to which any of these differences are mediated by NMR metabolites, placental tissue DNA methylation or transcriptomic data.
Box 1. The impact of the Covid-19 pandemic on the BRIST-IVF StudyBRIST-IVF was suspended for 13 months between March 2020 and April 2021 due to Covid 19 restrictions and staff redeployment. As a result, the study was unable to meet its the initial recruitment target and was closed earlier than planned as part of the NIHR Research and Recovery Reset Programme.Planned data collection was affected in the following ways
- During the closure period it was not possible to track the treatment outcomes of all recruited participants in real time and invite participants to pregnancy follow up. However, we have still been able to collect information on pregnancy outcomes from BCRM medical notes and from obstetric notes where participants have consented to access to NHS medical records.
- Reduction in the number of face-to-face consultations at the BCRM during and after the pandemic meant that the consent process moved from face-to-face to telephone appointments and that study measures visits were no longer carried out on the date of recruitment. This meant that:
- Biological samples were mostly collected after treatment protocols had been initiated.
- Fewer study measures visits were completed, and more study measures were self- reported or information was collected from fertility centre notes.
- Pregnancy clinics moved from face-to-face to virtual visits for several months after the study reopened meaning that a more limited set of measures were collected for some participants.
- Collection of blood samples for the purpose of making immortal cell lines was stopped as it was unclear whether these could be processed following Covid.
Materials and methods
Participants
Women and their partners were recruited from the Bristol Centre for Reproductive Medicine (BCRM), with recruitment occurring in two phases due to the COVID-19 pandemic. The first phase of recruitment at BCRM ran from 3^rd^ September 2019–27^th^ March 2020. The study reopened on 1 April 2021 and concluded on 30^th^ June 2023.
To be eligible to take part in the study, participants had to be aged 18 or over and to be undergoing or planning to undergo ART (IVF or ICSI) treatment. Treatment could involve use of own or donor gametes (eggs or sperm). Where treatment involved a partner, both the woman and her partner were required to enroll together to provide consent for access to BCRM medical notes. Only patients who had consented to contact research via the Human Fertilization and Embryology Authority (HFEA) consent to disclosure form were eligible to participate (cd-form-v10-16-october-2019.pdf (hfea.gov.uk)).
Recruitment
Participants were recruited prior to egg collection or frozen embryo transfer as part of ART treatment or following a scan at 7 weeks gestation confirming a viable pregnancy. Before the COVID-19 pandemic, recruitment followed a face-to-face model, where patients received an invitation letter and participant information sheet by post before their clinic visit and prior to commencing drug protocols. A research midwife or nurse obtained written informed consent in person.
Post-pandemic, due to fewer in-person visits, the recruitment process shifted to remote consent (see Box 1). Patients were contacted via email and telephone (with up to two follow-up calls) and completed written online consent forms in consultation with a research midwife or nurse. As part of enrollment, participants also provided written consent for NHS medical record linkage to facilitate data collection on pregnancy and birth outcomes.
Data collection
Questionnaires.
Participants completed a baseline questionnaire on paper (pre-Covid) or online (post-Covid) at the point of recruitment. The questionnaire (adapted from the Glasgow IVF Study questionnaire [13]) asked about employment, education, current use of medications, own and family history of cardiovascular disease, smoking, alcohol use and physical activity. A copy of the questionnaire is provided in the Supplementary material (S1 File).
Baseline study measurements
Between September 2019 and March 2020, study measures were completed at the point of recruitment. Following the April 2021 reopening, an appointment was made during the consent call for the research team to collect study measures. At these visits, participants had height, weight and blood pressure measured and blood and urine samples taken. Saliva samples were sought where participants were not able to or did not want to give a blood sample. Where it was not possible to conduct a study visit, height, weight and blood pressure were obtained from BCRM notes or self-reported by the participant.
Data collection from BCRM medical notes
For each woman undergoing treatment, information on reproductive history including previous pregnancies and births, previous fertility treatments, duration and causes of infertility, antral follicle count and anti mullerian hormone (AMH) level was provided by participants and/or extracted from their BCRM medical notes by the research midwives/nurses. Information on ART treatments was extracted from BCRM medical records, covering both ongoing and prior treatment cycles (for those recruited after their 7-week scan). The extracted data included treatment type, drug regimens, treatment protocols, folliculograms, number of eggs collected, sperm parameters, embryological data and treatment outcomes (pregnancy and birth). Treatment information was collected for participants up until the 31^st^ March 2024. Collection of information on birth outcomes from these treatments is still ongoing.
Pregnancy follow up procedures
If participants became pregnant following ART and had a viable pregnancy confirmed by ultrasound at 7 weeks gestation, they and their partners were invited to participate in the pregnancy follow up study. Invitations were initially sent by post but transitioned to email following the COVID-19 pandemic. Pregnant women were asked to complete an early pregnancy questionnaire (before 18 weeks gestation), a late pregnancy questionnaire (after 28 weeks gestation) and a birth questionnaire (around 2 weeks after the birth of their baby). Partners were sent one questionnaire during their partner’s pregnancy and a questionnaire after the birth of their baby. Questionnaires collected information on pregnancy health, substance use, feelings and emotions, plans and expectations for labour and parenthood and birth experiences. All pregnancy and birth questionnaires were the same as those used in ALSPAC-G2 and are available in supplementary material (S1 File).
Pregnant women and their partners were also invited to attend a clinic at the University of Bristol during pregnancy. At these clinics, participants had anthropometry and blood pressure measured and undertook physical capability and cognitive tests. They were asked to complete a 5-day online diet diary and to wear an activity monitor. Participants had blood samples taken and pregnant women provided a urine sample. Saliva was collected when blood sampling was not possible. Due to COVID-19 restrictions, virtual visits were implemented for a subset of participants, for which an equipment pack was provided which enabled collection of a subset of the measures from the face-to-face clinic.
At birth, cord blood and placenta samples, and measurements of the babies were collected where women delivered at participating hospitals (University Hospitals Bristol and Weston NHS Foundation Trust (St Michael’s), North Bristol NHS Trust (Southmead Hospital) and Royal United Hospitals Bath NHS Foundation Trust. Where possible, virtual post birth visits were conducted 7–15 days after the birth of the baby to collect anthropometric information for both the mother and baby.
All pregnancy clinics, birth sample collections and post birth follow-up visits were carried out by ALSPAC fieldworkers using identical protocols as the ALSPAC second generation pregnancy clinics [21]. This harmonization allows for direct comparisons between pregnancies conceived via ART and naturally conceived pregnancies in future analyses.
Biological samples
Biological samples were collected at three key phases: baseline, during pregnancy and at the time of birth (Fig 1). At baseline, non-fasting blood, urine and saliva samples were collected from participants. Blood samples were collected in Ethylenediaminetetraacetic acid (EDTA) tubes, centrifuged within 24 hours to separate plasma and white blood cells (a source of DNA) and stored at −80 °C within 2 hours of processing. Plasma was stored in 200 µl and 500 µl aliquots, while white blood cells were stored in 1 ml aliquots. Initial processing for most samples took place at the BCRM or University of Bristol laboratories at Southmead Hospital. All samples were processed following standardised protocols and have since been transferred for long term storage at Bristol Bioresource Laboratories (BBL).
*Biological samples collected for BRIST-IVF.Icon made by Freepik/DinosoftLabs from www.flaticon.com. EDTA: Ethylenediaminetetraacetic acid, ACD: acid citrate dextrose, NMR: nuclear magnetic resonance. 21 plasma samples failed NMR quality control, 1 sample was not sent for analysis due to participant not undergoing ART treatment.
For an initial set of participants, we also collected a blood sample in acid citrate dextrose (ACD) tubes for the creation of immortalized cell lines. However, this collection was discontinued in November 2021 due to uncertainties regarding processing feasibility during the COVID-19 pandemic.
At the pregnancy clinic, non-fasting blood and urine samples were collected from pregnant women, while partners were asked to provide fasting blood samples where possible. For these pregnancy clinic samples, cholesterol and glucose levels were obtained using PTS panels® on a CardioChek® PA, and haemoglobin levels measured using a HemoCue® Hb 201 + system, within 90 minutes of obtaining the sample. Following these tests, EDTA plasma, heparin plasma, serum and white blood cell samples were aliquoted out after centrifuging and stored at −80 °C.
Cord blood EDTA samples and placentas were collected at participating hospitals and couriered to the University of Bristol for processing and storage. Before processing, placentas were photographed and measured. Placentas were processed to maximise future use by storing small pieces in a variety of ways including, snap freezing, fixing in formalin and in RNA later solution. Placental membrane and cord slices were also stored. Cord blood was centrifuged and separated into EDTA plasma (aliquoted into 200 µL and 500 µL) and white blood cells, which were stored at −80 °C.
Data management
Data have been collected and stored using the Research Electronic Data Capture (REDCAP) software and workflow technology hosted at the University of Bristol [22]. Research data is stored in a separate filestore from personal data and only three researchers have access to personal identifiers.
Patient involvement
A patient advisory group of people who had undergone or were undergoing ART treatment was set up in early 2019 to advise on the relevance, acceptability of study processes and documentation.
Ethical approval
All participants provided written informed consent to participate in the study. Ethics approval for the study was obtained from the UK National Health Service Southwest- Frenchay Research Ethics Committee (IRAS project ID 236773, Initial approval 10/7/2019).
Results and discussion
Findings to date: completed data collection
Characteristics of the recruited sample.
Fig 2 shows the flow of participants from initial screening through invitation to recruitment. To aid interpretation of numbers, counts of ‘participants’ refer to all women and partners undergoing treatment, whereas counts of ‘couples or single women’ refer to the treatment units (i.e., a woman and her partner are counted once).
Flowchart of study recruitment.
Prior to the COVID-19 pandemic, 213 couples or single women were screened, while 2,226 were screened following resumption of ART services. Of these 2,439 couples/single women, 1,215 met the study’s eligibility criteria, with 502 (41%) successfully recruited. Since recruitment one woman has withdrawn her consent. The final cohort comprises 501 women and 465 partners (445 women with a male partner (89%), 20 women with a female partner (4%) and 36 women undergoing treatment without a partner (7%)).
Characteristics of the recruited women and their partners are shown in Tables 1 and 2. Where same-sex couples were undergoing reciprocal IVF/ICSI, for data collection purposes we considered the woman who would carry the embryo as the woman undergoing treatment. Women undergoing treatment had a mean age of 35.8 years (SD = 4.4) at recruitment and a mean BMI of 25.1 (SD = 4.4). The majority (92%) were of white ethnicity. At the time of recruitment, 251 women (50%) had never been pregnant, and 374 (75%) had not had a previous live birth. Their partners had a mean age of 37.6 years (SD = 5.8) and a mean BMI of 26.8 (SD = 4.3), with 94% identifying as white.
Table 1: Characteristics of the women recruited to the study (N = 501)*.
Table 2: Characteristics of the partners (N = 465).
Treatment cycles and pregnancy outcomes
Among the 501 couples and single women who were successfully recruited and remained in the study, 12 (2%) were enrolled following a confirmed viable pregnancy at a 7-week gestational scan.
For this study, we defined a treatment cycle as an egg collection with or without a fresh embryo transfer or a frozen embryo transfer. Between recruitment and March 2024, 490 women underwent a total of 1,055 ART cycles. Follow up time in the study for the 11 women who were recruited but did not undergo any relevant cycles ranged from 11-23 months. Of the 1,055 ART cycles, 125 were IVF (in 69 of these the woman had a fresh embryo transfer), 429 were ICSI (in 273 of these the woman had a fresh embryo transfer) and 501 were frozen embryo transfers (see Fig 3).
Overview of treatment cycles in IVF/ICSI.Ovarian stimulation aims to stimulate follicles to produce multiple mature oocytes to be retrieved via follicular aspiration. Mature oocytes are fertilised in vitro via IVF or ICSI and successful fertilisation results in the formation of embryos. Embryos of sufficient quality can be transferred into the uterus without freezing (fresh embryo transfer) or may be frozen and stored for future use. Frozen embryos can then be thawed and transferred into the uterus (frozen embryo transfer). For each ovarian stimulation cycle, there may be both a fresh embryo transfer and multiple frozen embryo transfers. Couples/individuals may undergo multiple ovarian stimulation cycles. Icon made by Freepik/cube29/Backwoods/Smashicons from www.flaticon.com.
Of the 843 embryo transfers, 458 (54%) resulted in a positive pregnancy test, 378 (45%) in a negative pregnancy test and 7 outcomes were unknown. Of the 458 pregnancies, 96 were biochemical or ended in a miscarriage prior to the 7-week scan. Treatment information reported in this paper is taken from a data download on 15 August 2024. Reported numbers may change where there are updates to clinic records.
Pregnancy questionnaires and clinic
Following a positive 7-week scan confirming a viable pregnancy, 305 women and, where appropriate, their partners were invited to participate in the pregnancy follow up study. Of these 305, 19 had two pregnancies resulting in a total of 324 pregnancies over the course of the study (see Fig 4). Invitations were not issued for 38 pregnancies due to closure of clinics for the Covid-19 pandemic, lack of consent for pregnancy follow up, or the study team not being notified of the pregnancy.
Flowchart of the pregnancy follow up to date.
Among the 324 pregnancies, participation in pregnancy follow-up was as follows: 246 (76%) pregnancies returned at least one pregnancy questionnaire, 233 pregnancies have a completed birth questionnaire, 117 women (for 119 pregnancies) and 39 partners participated in pregnancy clinics at the University of Bristol and 70 placentas and 58 cord blood samples were donated.
Biological samples
A total of 831 plasma samples were collected, comprising 372 women at baseline, 307 partners at baseline, 64 woman during pregnancy, 30 partners during pregnancy and 58 offspring cord blood (see Fig 1). Of the baseline plasma samples analysed using the Nightingale Health NMR CoreMetabolomics platform (Nightingale Health Plc, Finland), 358 from women and 299 from partners passed QC; 21 samples failed QC and were excluded. Details of the platform and its epidemiological applications have been published previously [23]. These data will be used to investigate the research questions outlined in the Planned Analyses section, with comparisons made to the ALSPAC-G2 cohort, which includes equivalent NMR metabolite assessments during pregnancy and in cord blood.
The protocol used in this study for preparing and storing placental tissue is identical to that use in ALSPAC-G2. We are currently (December 2025) preparing all 70 BRIST-IVF placenta samples for transcriptomic and DNA methylation analyses to explore differences in these biological measures between ART and natural conceptions using the ALSPAC-G2 as a comparison (Fig 1).
With future funding, additional analyses are planned, including plasma proteomic analyses on baseline woman and partner plasma samples and mass spectrometry metabolite profiling of baseline and pregnancy urine samples in women and their partner.
Ongoing data collection: Pregnancy and birth outcomes
Data collection on pregnancy outcomes following treatments is ongoing. We are collecting data for all pregnancies of study participants from BCRM medical notes. This information includes pregnancy outcome (miscarriage, stillbirth, termination of pregnancy, live birth), sex and birth weight of the baby. Additionally, pregnancy and birth outcomes are being retrieved from obstetric records for women who have consented to access to their NHS medical records and have given birth at local participating hospitals. These NHS records include antenatal measures (height, weight, blood pressure, haemoglobin), hospital admissions, diagnoses during pregnancy (gestational hypertension, pre-eclampsia, gestational diabetes), details of labour (how labour started, mode of delivery), child measurements, Apgar score and any congenital anomalies diagnosed at birth. We anticipate that we will have NHS clinical data for approximately 200 pregnancies, and that these data will be available for research use by early 2026.
Planned analyses
The BRIST-IVF study will leverage its extensive dataset to investigate several key research questions related to ART, metabolic profiling, and perinatal outcomes (see Table 3). To address questions 1 and 2, we will follow up findings of and meta-analyse results with the Glasgow IVF study. To address questions 4 and 5, we will use data from the ALSPAC-G2 cohort [21] as a comparison group of naturally conceived pregnancies. Given that BRIST-IVF participants were followed up using identical clinic protocols, laboratory procedures, and placental tissue analyses, this will allow for direct and meaningful comparisons between ART and non-ART pregnancies.
Table 3: Planned analyses in the Bristol IVF Study.
Through our planned analyses, we aim to extend current knowledge by characterising circulating metabolic profiles in people undergoing ART and assessing their value as markers of fertility and treatment success. We will replicate findings from the Glasgow IVF study [12,13] and meta-analyse results across both cohorts to increase statistical power and enhance the robustness and generalisability of our findings. By adding to the growing evidence on molecular signatures in placental tissue [15,16], we can begin to understand mechanisms through which ART may impact on perinatal outcomes and longer term offspring health.
Strengths and limitations
BRIST-IVF is a large clinical cohort of women and their partners undergoing ART, with extensive demographic, lifestyle, biological samples and treatment-related data. We have also been able to follow up the pregnancies and births via questionnaires, clinics and medical record linkage. Importantly, pregnancy data collection followed the same protocols as the ALSPAC-G2 [21], enabling direct comparisons between ART pregnancies and naturally conceived pregnancies.
Our study cohort closely mirrors the UK population undergoing ART, both in terms of average age and family type. In 2021, the average age of IVF patients in the UK was 36.0 years, and 89% of women undergoing IVF had a male partner, 4% had a female partner, and 6% had no partner [24]. The BRIST-IVF cohort has a higher proportion of participants of white ethnicity (92%) compared to the UK average for IVF treatment in 2020−21 (77%) [25]. However, this proportion aligns with the ethnic composition of the South West region (93% of residents are of white ethnicity) [26].
Despite these strengths, limitations include the modest response, with only 41% of single women/couples screened agreeing to participate. A major reason for limited participation was the high proportion of patients (38%) who did not consent to be contacted for research when completing the HFEA form prior to beginning treatment. This proportion is similar to findings from a study conducted at a fertility centre in northern England between 2010 and 2019, where 47% of patients declined to provide consent for contact research [27].
Whilst we have near complete baseline questionnaire and treatment data from BCRM medical records, only 76% of women invited contributed to the pregnancy follow up study by answering a questionnaire or attending clinic. However, obstetric data will be available for all women who consented to NHS medical record abstraction and delivered within local participating hospitals. Additionally, most blood and urine samples were taken after women had started treatment protocols meaning that biological measures (e.g., metabolites) may be affected by ART medications. However, detailed information on treatment and drug protocols has been collected, allowing for appropriate adjustment in analyses.
Conclusions
The BRIST-IVF study, with its comprehensive metabolic, clinical, and biological data, is uniquely positioned to address some of the limitations of birth cohort and electronic health record studies in ART research. By integrating detailed treatment information with biospecimen analysis and pregnancy follow-up, the BRIST-IVF study offers a valuable resource for advancing our understanding of the predictors and consequences of ART conception, with important implications for optimizing fertility treatments and improving ART pregnancy outcomes.
Supporting information
S1 FileSupplementary Material.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Infertility prevalence estimates, 1990-2021. Geneva: World Health Organization. 2023. https://www.who.int/publications/i/item/978920068315
- 2Cousineau TM, Domar AD. Psychological impact of infertility. Best Pract Res Clin Obstet Gynaecol. 2007;21(2):293–308. doi: 10.1016/j.bpobgyn.2006.12.003 17241818 · doi ↗ · pubmed ↗
- 3Fauser BC. Towards the global coverage of a unified registry of IVF outcomes. Reprod Biomed Online. 2019;38(2):133–7. doi: 10.1016/j.rbmo.2018.12.001 30593441 · doi ↗ · pubmed ↗
- 4Vayena E, Peterson HB, Adamson D, Nygren K-G. Assisted reproductive technologies in developing countries: are we caring yet?. Fertil Steril. 2009;92(2):413–6. doi: 10.1016/j.fertnstert.2009.02.011 19324335 · doi ↗ · pubmed ↗
- 5Nelson SM, Lawlor DA. Predicting live birth outcomes after in vitro fertilisation. BJOG. 2012;119(13):1668; author reply 1668-9. doi: 10.1111/j.1471-0528.2012.03508.x 23164114 · doi ↗ · pubmed ↗
- 6Templeton A, Morris JK, Parslow W. Factors that affect outcome of in-vitro fertilisation treatment. Lancet. 1996;348(9039):1402–6. doi: 10.1016/S 0140-6736(96)05291-9 8937279 · doi ↗ · pubmed ↗
- 7Waylen AL, Metwally M, Jones GL, Wilkinson AJ, Ledger WL. Effects of cigarette smoking upon clinical outcomes of assisted reproduction: a meta-analysis. Hum Reprod Update. 2009;15(1):31–44. doi: 10.1093/humupd/dmn 046 18927070 · doi ↗ · pubmed ↗
- 8Fuentes A, Muñoz A, Barnhart K, Argüello B, Díaz M, Pommer R. Recent cigarette smoking and assisted reproductive technologies outcome. Fertil Steril. 2010;93(1):89–95. doi: 10.1016/j.fertnstert.2008.09.073 18973890 · doi ↗ · pubmed ↗