Atopic dermatitis and the risk of osteoporosis and fractures: a meta-analysis of cohort studies
Hongfei Liu, Huilin Ru, Peng Yu, Wei Wei, Shixuan Wang

TL;DR
This study finds that people with atopic dermatitis have a higher risk of osteoporosis and fractures, especially if their condition is severe.
Contribution
This paper provides the first meta-analysis linking atopic dermatitis severity to specific fracture risks in different body regions.
Findings
AD patients have a 56% increased risk of osteoporosis and an 8% increased risk of all-cause fractures.
Fracture risk rises with AD severity and is highest for vertebral and lower limb fractures.
No significant publication bias was detected, confirming the robustness of the findings.
Abstract
This meta-analysis aims to evaluate the risk of osteoporosis and fractures in patients with atopic dermatitis (AD) by synthesizing data from cohort studies. We also provide a comprehensive analysis of fracture risks across different severities of AD and anatomical sites. Following the PRISMA 2020 guidelines, a systematic search was conducted in PubMed, Embase, and the Cochrane Library up to May 30, 2025. Studies that investigated the relationship between AD and osteoporosis or fractures were included in the analysis. Data extraction and screening were performed independently by two reviewers. Study quality was assessed using the Newcastle-Ottawa Scale (NOS). A random-effects meta-analysis was applied, alongside sensitivity and subgroup analyses. Publication bias was evaluated using funnel plots and Egger’s test. Ten cohort studies, involving 368 to over 2 million AD patients, were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
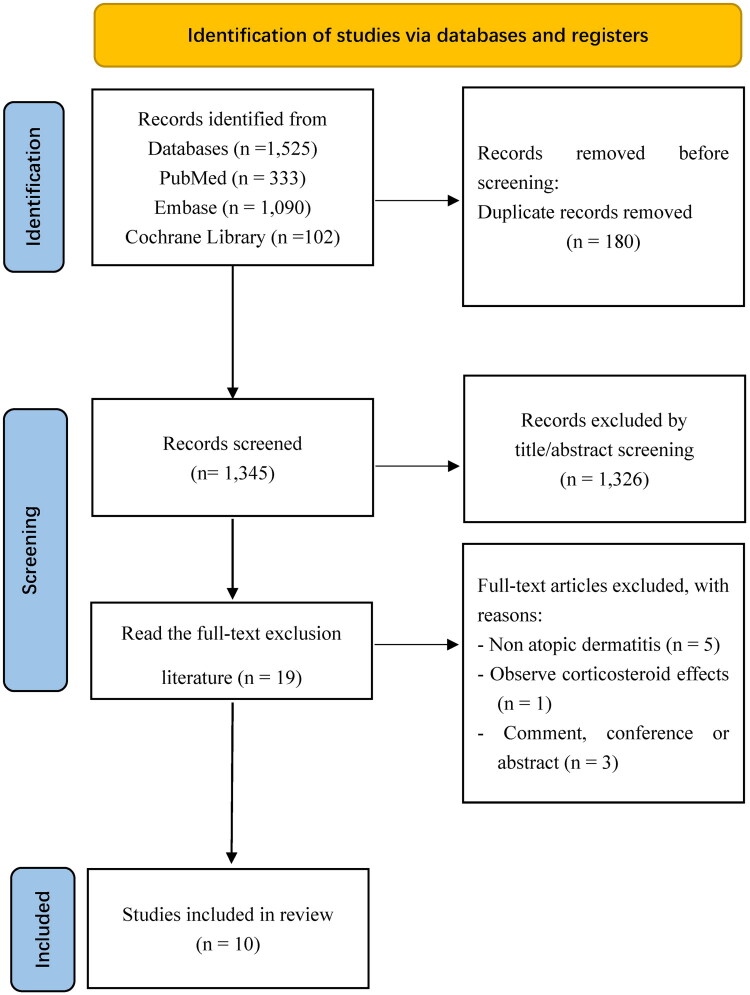 Figure 1
Figure 1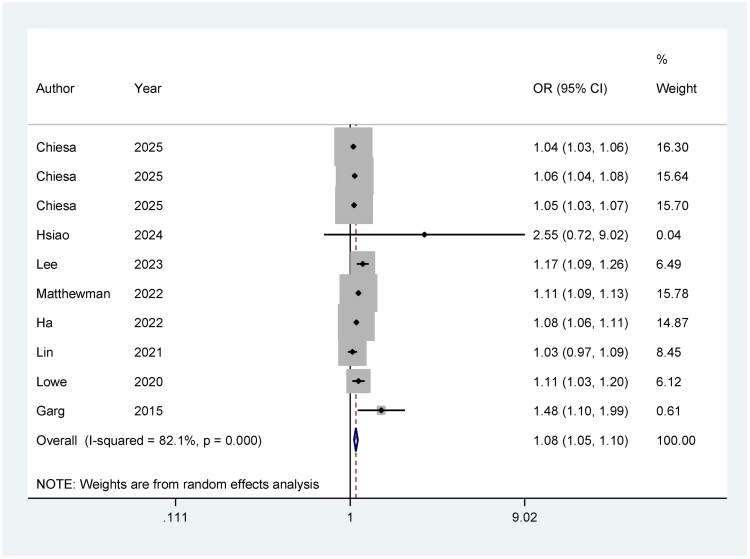 Figure 2
Figure 2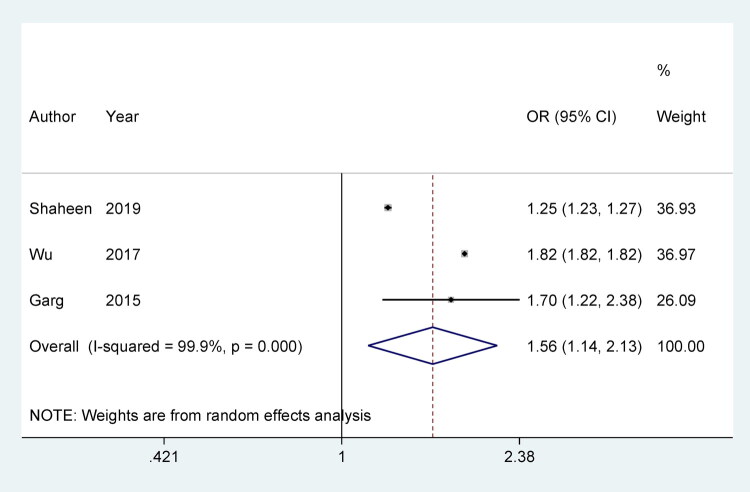 Figure 3
Figure 3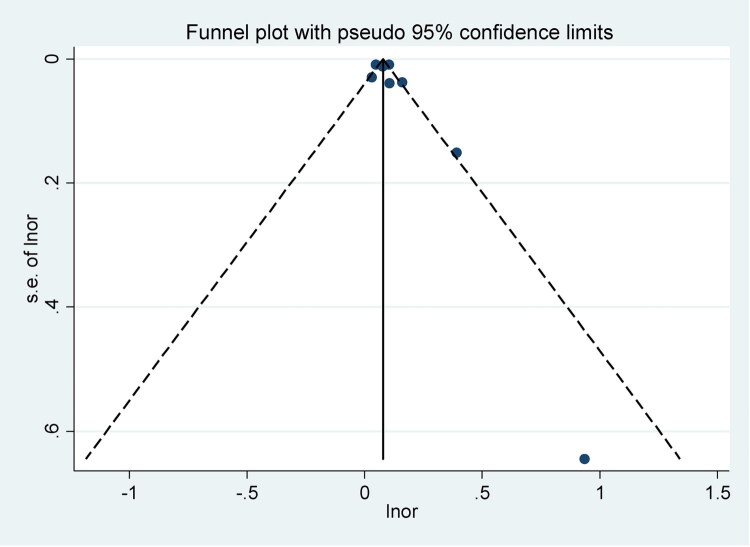 Figure 4
Figure 4| Author | Year | Study type | Country | Data source | Enroll period | Follow-up years (mean ± SD) y | AD1 diagnostic criteria | AD severity classification | Number of AD patients | Fracture/Osteoporosis diagnostic criteria | Number of fracture cases | Number of control group | Age | Confounders adjusted |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chiesa | 2025 | Retrospective cohort study | UK | The Health Improvement Network | 1994–2015 | 5.51–5.64 (4.22–4.40) | NR | Treatment-based13 | 465,622 | NR | NR | 2,678,888 | 18–65: 37–40 (27–52) y | Age, BMI, smoking status, drinking status and Townsend Index. |
| 6.21–6.93 (4.88–5.37) | 159479 | ≥ 65: 73–75 (69–81) y | ||||||||||||
| Hsiao | 2024 | Retrospective cohort study | China | Taichung Veterans General Hospital, Taichung, Taiwan | 2020–2021 | NR | Medical records | NR | 50 | BMD2 examination and medical records | 13 | 386 | Elderly people: 70 (62, 77) y | Age, corticosteroids use, history of fracture, chronic kidney disease, cardio vascular disease, and chronic lung disease. |
| Lee | 2023 | Retrospective cohort study | Korea | NHIS3 | NR12 | 7.52 | ICD4-10 | Treatment-based | 342,601 | ICD-10 | 86,233 | NR | Children | Sex, calendar period of birth, birth season, region of residence, household income, breastfeeding, preterm birth, low birth weight, allergic rhinitis, asthma, diabetes mellitus, thyroid disorder, chronic inflammatory disease, chronic kidney disease, chronic neurological disorder, anemia, neuropsychiatric disorder, food allergy, and long-term use of systemic corticosteroids. |
| Matthewman | 2022 | Retrospective cohort study | UK | CPRD5 and HES6 | 1998–2016 | 4.41 | Read code and ICD-10 | Treatment-based | 525,923 | Read code and ICD-10 | NR | 2,562,334 | NR | Age, sex, GP, date of cohort entry, calendar time, IMD, and asthma |
| Ha | 2022 | Retrospective cohort study | Korea | NHIS and NHSPIC7 | NR | 8.9 | ICD-10 | NR | 38,319 | ICD-10 | NR | 314,721 | Children ≤71 months | Birth year, certain conditions originating during the perinatal period, physical examination results at 4–6 months old, clinical conditions with possible confounding effects. |
| Lin | 2021 | Retrospective cohort study | China | NHIRD8 and LHID9 | 1997–2013 | NR | ICD-9 | Healthcare utilization-based14 | 36,825 | ICD-9 | 1,518 | 147,420 | 22.6 y | Each incremental year of age, sex, hospital visiting times, atopic dermatitis, moderate-to-severe atopic dermatitis, rheumatoid arthritis, osteoporosis, postmenopausal, topical corticosteroids, systemic corticosteroids, DMARDs, phototherapy. |
| Shaheen | 2019 | Retrospective cohort study | USA | NEDS10 and NIS11 | 2002–2012 | NR | ICD-9 | NR | NR | ICD-9 | 272,036 | NR | ≥ 50 y | NR |
| Lowe | 2020 | Retrospective cohort study | UK | CPRD and HES | 1998–2016 | 5 | NR | Treatment-based | 526,808 | NR | 520,197 | 2,569,030 | ≥18 y | Time-updated asthma, IMD, and calendar time, BMI, smoking status, harmful alcohol use, and high-dose oral glucocorticoid use. |
| Wu | 2017 | Retrospective cohort study | China | NHIRD | / | NR | ICD-9 | NR | 35,229 | BMD examination and ICD-9 | 360 | 35,229 | 20–49: 33.6 y | Age, sex, comorbidities (hypertension, diabetes mellitus, hyperlipidemia, chronic kidney disease, chronic liver disease, chronic obstructive pulmonary disease, depression) and use of systemic corticosteroids. |
| Garg | 2015 | Retrospective cohort study | USA | National Health and Nutrition Examination Survey | 2005–2006 | NR | Household surveys | NR | 368 | BMD examination and self-reported | 33 | 4,604 | 20–85 y | NR |
| Study | Year | Selection | Comparability | Outcome | Total |
|---|---|---|---|---|---|
| Cohort studies ( | |||||
| Chiesa | 2025 | *** | ** | *** | 8 |
| Garg | 2015 | ** | * | ** | 5 |
| Ha | 2022 | **** | ** | ** | 8 |
| Hsiao | 2024 | *** | ** | *** | 8 |
| Lee | 2023 | *** | ** | ** | 7 |
| Lin | 2021 | *** | ** | ** | 7 |
| Lowe | 2020 | **** | * | ** | 7 |
| Matthewman | 2022 | *** | ** | *** | 8 |
| Shaheen | 2019 | *** | ** | *** | 8 |
| Wu | 2017 | *** | ** | *** | 8 |
| Subgroups | Included studies | OR (95%CI) | Heterogeneity | |
|---|---|---|---|---|
|
| ||||
|
| ||||
| Mild AD | 4 | 1.05 (1.02, 1.09) | 95.2% | 0.000 |
| Moderate AD | 3 | 1.08 (1.03, 1.12) | 92.7% | 0.000 |
| Severe AD | 3 | 1.26 (1.21, 1.31) | 56.0% | 0.059 |
| Moderate to severe AD | 2 | 1.23 (1.20, 1.26) | 0.0% | 0.526 |
|
| ||||
| Cranial and facial bones | 2 | 1.13 (1.10, 1.15) | 0.0% | 0.362 |
| Lower limb bones | 6 | 1.11 (1.08, 1.13) | 65.0% | 0.014 |
| Ribs/thorax | 1 | 0.97 (0.91, 1.03) | ||
| Upper limb bones | 5 | 1.06 (1.05, 1.07) | 0.0% | 0.571 |
| Vertebral column | 6 | 1.14 (1.08, 1.20) | 67.3% | 0.009 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatology and Skin Diseases · Dermatological diseases and infestations · Psoriasis: Treatment and Pathogenesis
Introduction
Atopic dermatitis (AD) is the most prevalent chronic inflammatory skin disorder worldwide, characterized by severe itching, recurrent eczematous lesions, and a variable disease course [1,2]. In 2021, the global prevalence of AD reached 129 million cases, and the number is projected to increase steadily over the next three decades, presenting a significant public health challenge [3]. The pathogenesis of AD is multifactorial, involving genetic predisposition, dysregulated innate immunity, impaired epithelial barrier function, skin microbiome alterations, and environmental factors [4]. In addition to its frequent comorbidity with other atopic conditions, such as allergic rhinitis and asthma [5], AD has also been identified as an independent risk factor for a variety of non-atopic diseases, including cardiovascular and psychiatric disorders [6].
Recent evidence suggests that AD may have a detrimental impact on bone health, primarily through mechanisms such as chronic inflammation [7,8], prolonged corticosteroid use [9], and lifestyle factors like reduced physical activity due to constant itching [10]. A previous meta-analysis by Wu et al. [11] examined the relationship between AD, bone mineral density, osteoporosis, and fracture risk, focusing on both children and adults. However, this analysis included only four studies and was limited in its ability to address publication bias and the differential fracture risks at various anatomical sites. Another meta-analysis by Zhou et al. faced similar limitations, underscoring the need for a more comprehensive examination of this issue [12]. Given the growing body of research, including several large-scale cohort studies conducted recently [13–16], the association between AD and bone health remains controversial. In light of this, we conducted a meta-analysis based on cohort studies to better clarify the risks of osteoporosis and fractures in individuals with AD, ultimately aiming to inform targeted clinical prevention strategies.
Methods
This meta-analysis was conducted in accordance with the PRISMA 2020 guidelines for systematic reviews [17]. The protocol for this review was prospectively registered with PROSPERO (CRD420251066550), adhering to the established guidelines for systematic reviews and meta-analysis [18].
Data sources
A comprehensive literature search was performed in three major databases (PubMed, EMBASE, and the Cochrane Library), covering all available studies from database inception to May 30, 2025. No restrictions were imposed based on publication language or date. We employed subject terms (Emtree in Embase, MeSH in PubMed) along with relevant keywords to capture studies related to AD, osteoporosis, fractures, and their variations. To minimize the risk of missing eligible studies, we also examined the reference lists of included studies and relevant prior meta-analyses [11,12]. Detailed search strategies for each database are provided in Supplementary Tables 1–3.
Study selection
The initial set of records was imported into NoteExpress reference management software, and duplicate entries were removed to avoid redundancy. Two independent reviewers (Huilin Ru and Peng Yu) then performed title and abstract screening to exclude studies that were clearly irrelevant. The remaining records were classified as either eligible, ineligible, or uncertain. For studies with uncertain eligibility, full-text articles were reviewed to determine inclusion. Any disagreements between the two primary reviewers were resolved through discussion with a third reviewer (Shixuan Wang), ensuring consensus and minimizing bias in the selection process.
Eligibility criteria
Studies were included in this meta-analysis if they investigated the association between AD and the risk of osteoporosis or fractures. Eligible studies needed to report outcomes such as diagnosed osteoporosis, all-cause fractures, or fractures at specific anatomical sites in participants diagnosed with AD or with a documented history of AD. The comparison group had to consist of healthy individuals or non-AD patients. Furthermore, the studies were required to provide effect estimates such as odds ratios (OR), relative risks (RR), or 95% confidence intervals (CIs), which allowed for the assessment of the strength of the association between AD and the specified outcomes. Only cohort studies, either prospective or retrospective, were included to minimize methodological biases that could arise from other types of observational studies. When multiple publications used the same underlying database over overlapping time periods, we prioritized the cohort with the largest sample size and most comprehensive reporting for the primary meta-analysis and used additional overlapping studies only for sensitivity or subgroup analyses to minimize double-counting of participants.
Studies were excluded if they did not meet the above criteria, such as conference abstracts, commentaries, or duplicate publications. Also, studies that did not report independent data on fractures or osteoporosis, like reviews or meta-analyses without primary data, were excluded. This ensured that only high-quality, relevant studies were included, providing the most reliable evidence on the relationship between AD and fracture or osteoporosis risk.
Data extraction
Data were systematically extracted using a pre-designed form created in Microsoft Excel (Microsoft Corporation, USA). Two reviewers (Hongfei Liu and Wei Wei) independently extracted data from eligible studies, including the following key information: first author, year of publication, study type, country of origin, data source, enrollment period, follow-up duration, diagnostic criteria for AD, the number of AD patients, fracture/osteoporosis diagnostic criteria, number of fracture cases, size of the control group, patient age, and potential confounders. Extracted data were cross-verified to ensure accuracy and consistency, and any discrepancies were resolved through discussion and consensus.
Study quality
The methodological quality of the included cohort studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS) (available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp). The NOS assesses three major domains: selection, comparability, and outcome assessment, with a total score ranging from 0 to 9 stars. Studies were categorized based on their NOS score as follows: high quality (7–9 stars), moderate quality (4–6 stars), and low quality (0–3 stars).
Data synthesis
Data analysis was performed using Stata software (version 14). Due to anticipated clinical, methodological, and statistical heterogeneity across studies, a random-effects model was employed to pool the effect estimates, enhancing the robustness and generalizability of the findings [19,20]. Sensitivity analyses were conducted to evaluate the stability of the overall results, helping to identify potential sources of heterogeneity. Subgroup analyses were performed to explore variations in fracture risk based on factors such as fracture site and the severity of AD. Publication bias was evaluated using funnel plots and Egger’s regression test.
Results
Study selection
A total of 1,525 records were identified from various databases, including PubMed (n = 333), Embase (n = 1,090), and the Cochrane Library (n = 102). After removing duplicates (n = 180), 1,345 records remained for screening. From the title and abstract screening, 1,326 records were excluded, leaving 19 full-text articles for further evaluation. These full-text articles were excluded for the following reasons: non-atopic dermatitis (n = 5), observational corticosteroid effects (n = 1), and being comments, conference abstracts, or similar (n = 3). The list of excluded studies is in Supplementary Table 4. Ultimately, 10 studies [13–16, 21–25, 27] were included in the meta-analysis. This process is visually depicted in the literature screening flowchart (Figure 1).
Literature screening flow chart.
Studies characteristics
This meta-analysis includes 10 cohort studies conducted in various countries, including the UK, China, Korea, the USA, and Taiwan, from 2005 to 2025. These studies analyzed the relationship between AD and the risk of fractures or osteoporosis, utilizing diverse data sources such as national health databases, hospital records, and household surveys. The diagnostic criteria for AD and fractures/osteoporosis varied across studies, with some using ICD codes, medical records, and bone mineral density (BMD) examinations. The patient populations included both children and adults, with sample sizes ranging from 368 to over 2 million participants. Follow-up periods ranged from 4 to 9 years, with adjustment for multiple confounders such as age, BMI, smoking, comorbidities, and medication use. The basic characteristics of the included cohorts are shown in Table 1.
Quality of included studies
Most studies received a total score between 7 and 8, indicating generally good quality. The selection domain was strong for most studies, with several studies achieving high ratings. However, the comparability domain showed some variability, with a few studies scoring lower, reflecting weaker control of confounders. In the outcome domain, most studies demonstrated adequate methods for assessing outcomes. Overall, the studies were of good methodological quality, with minor weaknesses in controlling for confounders in some studies. The detailed assessment scores are presented in Table 2.
AD and the risk of all-cause fractures
The overall pooled analysis shows a significant association, with an OR of 1.08 (95% CI: 1.05, 1.10), suggesting that patients with AD have an increased risk of fractures compared to those without AD. The heterogeneity is high (I^2^ = 82.1%), indicating substantial variability between the studies (Figure 2). The sensitivity analysis plot provides a visual representation of the influence of individual studies on the overall effect estimate. It shows that the meta-analysis results remain robust even when specific studies are omitted. The individual study estimates, represented by their confidence intervals, vary but consistently suggest an increased fracture risk in AD patients. This indicates the robustness of the findings across different study populations and methodologies (Supplementary Figure 1).
Meta-analysis of AD and the risk of all-cause fractures.
AD and the risk of osteoporosis
The pooled OR for osteoporosis risk in AD patients is 1.56 (95% CI: 1.14, 2.13), suggesting a significant increase in osteoporosis risk among AD patients. The heterogeneity of the studies is very high, with an I^2^ value of 99.9% (p = 0.000), indicating substantial variability between the included cohort studies (Figure 3). The sensitivity analysis, shown in Supplementary Figure 2, assesses the robustness of the overall findings by excluding one study at a time. The results remain consistent even when individual studies are omitted, indicating the robustness of the meta-analysis. This suggests that the relationship between AD and the increased risk of osteoporosis is stable across different studies.
Meta-analysis of AD and the risk of osteoporosis.
Subgroup analysis
For disease severity, the analysis reveals that the risk of fractures increases with the severity of AD. Mild AD is associated with a OR of 1.05 (95% CI: 1.02, 1.09), with high heterogeneity (I^2^ = 95.2%, p < 0.0001). Moderate AD shows a slightly higher OR of 1.08 (95% CI: 1.03, 1.12) with similarly high heterogeneity (I^2^ = 92.7%, p < 0.0001). Severe AD has an even higher OR of 1.26 (95% CI: 1.21, 1.31), but with moderate heterogeneity (I^2^ = 56.0%, p = 0.059). For moderate to severe AD, the OR is 1.23 (95% CI: 1.20, 1.26), showing no significant heterogeneity (I^2^ = 0.0%, p = 0.526), suggesting consistent results across studies.
In terms of fracture sites, the risk is highest for vertebral column, with an OR of 1.14 (95% CI: 1.08, 1.20) and moderate heterogeneity (I^2^ = 67.3%, p = 0.009). For lower limb bones, the OR is 1.11 (95% CI: 1.08, 1.13) with moderate heterogeneity (I^2^ = 65.0%, p = 0.014). The rib/thorax site shows no significant association (OR = 0.97, 95% CI: 0.91, 1.03), with no data on heterogeneity. The upper limb bones show a slight increase in risk (OR = 1.06, 95% CI: 1.05, 1.07) with no heterogeneity (I^2^ = 0.0%, p = 0.571). Lastly, fractures of the cranial and facial bones are associated with an OR of 1.13 (95% CI: 1.10, 1.15), with no heterogeneity (I^2^ = 0.0%, p = 0.362). The subgroup analysis for the risk of all-cause fractures in patients with AD is summarized in Table 3.
Publication bias
The funnel plot appears symmetrical, suggesting no significant publication bias in the included studies (Figure 4). Additionally, Egger’s test was conducted to statistically assess publication bias, with a p value of 0.316. This p value indicates that there is no evidence of publication bias, as the result is not statistically significant (p > 0.05).
Funnel plot of publication bias.
Discussion
Main findings
This meta-analysis provides a comprehensive review of the risk of osteoporosis and fractures in patients with atopic dermatitis (AD), comparing them to those without AD, based on data from ten cohort studies. We found a significant association between AD and increased risks of osteoporosis and fractures. Specifically, AD patients showed a 56% higher risk of osteoporosis (OR = 1.56, 95% CI: 1.14–2.13; I^2^ = 99.9%, p < 0.0001) and an 8% higher risk of all-cause fractures (OR = 1.08, 95% CI: 1.05–1.10; I^2^ = 82.1%, p < 0.0001). Subgroup analyses further revealed that fracture risk increased progressively with the severity of AD. Site-specific fracture risks were significantly higher for the vertebral column (OR = 1.14, 95% CI: 1.08–1.20; I^2^ = 67.3%, p = 0.009) and the lower limb (OR = 1.11, 95% CI: 1.08–1.13; I^2^ = 65.0%, p = 0.014). These findings reinforce previous research on the relationship between AD and skeletal complications while contributing new insights, especially by quantifying fracture risks in different body regions.
Comparison with previous meta-analyses
Our results are consistent with previous studies [11,12], confirming significantly increased risks of both osteoporosis (OR = 1.56 vs. RR = 1.95 in Wu et al.) and all-cause fractures (OR = 1.08 vs. RR = 1.13 in Wu et al.), solidifying AD as an independent risk factor for these outcomes. However, our study improves on prior work by incorporating methodological advancements. Previous meta-analyses included both cross-sectional (n = 7) and cohort studies (n = 3), which may have introduced susceptibility bias. Moreover, Egger’s regression test indicated publication bias (p = 0.028). In contrast, we focused exclusively on cohort studies (n = 10), reducing heterogeneity and enhancing causal inference, with no evidence of publication bias (p = 0.316). Furthermore, our analysis uniquely quantified risks for vertebral and lower limb fractures (OR = 1.14, p = 0.009 and OR = 1.11, p = 0.014, respectively), a novel contribution. Additionally, we identified a progressive increase in fracture risk with greater AD severity, emphasizing the need for tailored clinical approaches for patients with severe AD, especially those at risk for vertebral and lower limb fractures.
Possible mechanisms linking atopic dermatitis and bone health
The association between AD and bone health can be explained by multiple factors related to the pathophysiology of AD and its treatments. AD is a chronic inflammatory condition [2], and the activation of osteoclasts by pro-inflammatory cytokines such as IL-1, IL-6, IL-17, IL-31, IL-33, TNF-α, and RANKL accelerates bone resorption [26]. This inflammatory process may contribute to the early onset of bone loss, particularly in children and adolescents [15,27]. Additionally, glucocorticoids (GCs), commonly prescribed for AD, can impair bone formation and enhance resorption through various mechanisms, including alterations in muscle strength, calcium and vitamin D metabolism, fat metabolism, and sex steroid levels [28,29]. While systemic and topical glucocorticoids are well-established contributors to bone loss, one large cohort reported that the association between AD and fractures persisted after adjustment for oral corticosteroid use, suggesting that corticosteroids alone do not fully explain the increased risk [16]. Lifestyle and dietary factors may also play a role, such as reduced calcium and vitamin D intake due to food intolerances, lower physical activity due to itching, and psychological factors like stress and sleep disturbances [7,11,16,27]. Moreover, our previous Mendelian randomization study suggested a potential causal relationship between allergic diseases, eosinophils, and osteoporosis based on genetic variation [8]. In summary, the link between AD and bone health is complex, extending beyond the effects of GCs and inflammation, and warrants further investigation.
Limitations and clinical implications
This meta-analysis adheres to the latest PRISMA 2020 guidelines, was prospectively registered with PROSPERO, and includes the largest cohort of patients with AD examined in relation to osteoporosis and fractures. These findings offer valuable insights for clinical practice, particularly for the prevention and management of bone health in AD patients.
However, several limitations must be acknowledged. First, substantial heterogeneity was observed in the pooled estimates, especially for osteoporosis (I^2^ = 99.9%) and all-cause fractures (I^2^ = 82.1%). This variability may be due to differences in study populations (e.g. age, sex), data sources (e.g. administrative vs. clinical databases), diagnostic criteria for AD and outcomes (e.g. ICD codes vs. BMD measurements), and the degree of confounder adjustment. Although sensitivity and subgroup analyses confirmed the robustness of our results, unexplained heterogeneity limits the precision and generalizability of our findings. Second, while our stratified analysis by AD severity showed a gradient in fracture risk, many studies lacked standardized definitions of AD severity, potentially introducing misclassification bias. Future studies should use standardized scoring systems (e.g. SCORAD, EASI) to enhance comparability. Third, information on topical and systemic corticosteroid exposure was not consistently reported across the included cohorts. Although several studies adjusted for or stratified by oral and/or topical corticosteroid use, others did not provide sufficient detail to allow pooled analyses by corticosteroid dose or duration. Therefore, residual confounding by corticosteroid exposure cannot be entirely excluded. Moreover, important determinants of bone health, including physical activity, diet, sun exposure, vitamin D or calcium supplements, smoking, and alcohol use, were not uniformly measured. These unmeasured or incompletely captured factors may influence both AD severity and bone outcomes, and thus our results should be interpreted as evidence of association rather than proof of causality. Fourth, diagnostic bias is an inherent limitation of observational studies using routine healthcare data. Patients with AD are more likely to have repeated contact with healthcare providers, which may increase the probability of diagnosing both AD and comorbid osteoporosis or fractures. Because the included studies relied on routine medical records, differential healthcare utilization may introduce potential diagnostic or surveillance bias that cannot be fully eliminated. Lastly, as all studies included were retrospective cohort studies, causal inference is limited by potential bias in exposure and outcome assessment. Prospective studies are needed to validate these findings.
In addition to adults, children with AD also have a relatively high incidence of fracture events. From a clinical perspective, fractures in children may affect peak bone mass and future bone development, while osteoporosis and fractures in adults (especially the elderly) are major factors contributing to morbidity, disability, and mortality. Therefore, identifying age-specific risks associated with traumatic fractures is crucial for formulating precise prevention strategies tailored to children and adult populations. Because few paediatric cohorts reported age-stratified effect estimates, future large studies should provide separate risk estimates for children, adolescents, and adults to allow more refined age-specific meta-analyses.
Furthermore, the included cohort studies did not consistently report baseline fracture or osteoporosis incidence in AD versus non-AD groups, preventing a reliable pooled calculation of absolute risk differences. Despite this limitation, even small relative increases may lead to meaningful public health impacts given the high global prevalence of AD. Importantly, our findings still warrant clinical attention, as they highlight the need for greater vigilance for bone health in AD populations. Specifically, our results suggest that AD (particularly moderate-to-severe disease, older age, and concomitant long-term systemic corticosteroid use) may be considered a risk-enhancing factor when evaluating the need for osteoporosis screening and fracture prevention. In such patients, clinicians may reasonably prioritize bone-health counseling (adequate calcium and vitamin D intake, safe weight-bearing exercise), cautious use of systemic corticosteroids, and consideration of bone mineral density testing. From the perspective of healthcare services, this may be more feasible than universal screening. However, considering Alzheimer’s disease as a risk marker in existing fracture risk assessment approaches requires further evaluation of its cost-effectiveness in dedicated health economics research.
Conclusion
This meta-analysis provides evidence that AD is associated with an increased risk of osteoporosis and fractures, particularly in patients with severe AD and those at higher risk of vertebral or lower limb fractures. These findings highlight the importance of targeted bone health monitoring in the clinical management of AD. However, due to the heterogeneity and potential residual confounding, clinicians should interpret these findings with caution.
Future prospective studies are warranted to more rigorously examine the association between AD and adverse bone outcomes. Such studies should incorporate standardized assessments of AD severity and bone health, using validated severity scoring systems and uniform diagnostic criteria for osteoporosis and fractures. They should also include broader representation of pediatric patients, enable long-term follow-up from childhood-onset AD into adulthood, and systematically document corticosteroid exposure and other key determinants of bone health. These efforts will help clarify the underlying associations and support the development of more precise and individualized prevention strategies for patients with AD.
Supplementary Material
Supplemental Material
Appendix PRISMA_2020_checklist.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ständer S. Atopic dermatitis. N Engl J Med. 2021;384(12):1136–1143. doi: 10.1056/NEJ Mra 2023911.33761208 · doi ↗ · pubmed ↗
- 2Guttman-Yassky E, Renert-Yuval Y, Brunner PM. Atopic dermatitis. Lancet. 2025;405(10478):583–596. doi: 10.1016/S 0140-6736(24)02519-4.39955121 · doi ↗ · pubmed ↗
- 3GBD 2021 Asthma and Allergic Diseases Collaborators. Global, regional, and national burden of asthma and atopic dermatitis, 1990-2021, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Respir Med. 2025;13(5):425–446. doi: 10.1016/S 2213-2600(25)00003-7.40147466 · doi ↗ · pubmed ↗
- 4Schuler CF 4th, Billi AC, Maverakis E, et al. Novel insights into atopic dermatitis. J Allergy Clin Immunol. 2023;151(5):1145–1154. doi: 10.1016/j.jaci.2022.10.023.36428114 PMC 10164702 · doi ↗ · pubmed ↗
- 5Weidinger S, Beck LA, Bieber T, et al. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1):1; [cited 2018 Jun 21]. doi: 10.1038/s 41572-018-0001-z.29930242 · doi ↗ · pubmed ↗
- 6Thyssen JP, Halling AS, Schmid-Grendelmeier P, et al. Comorbidities of atopic dermatitis – what does the evidence say? J Allergy Clin Immunol. 2023;151(5):1155–1162. doi: 10.1016/j.jaci.2022.12.002.36621338 · doi ↗ · pubmed ↗
- 7Mukovozov IM, Morra DE, Giustini D, et al. Atopic dermatitis and bone health: a systematic review. J Eur Acad Dermatol Venereol. 2021;35(3):615–628. doi: 10.1111/jdv.16895.32853421 · doi ↗ · pubmed ↗
- 8Yue X, Liu H, Yang S, et al. Causal association of allergic diseases, eosinophils, and osteoporosis: a Mendelian randomization study. World Allergy Organ J. 2025;18(3):101039; [cited 2025 Mar 11]. doi: 10.1016/j.waojou.2025.101039.40151544 PMC 11946878 · doi ↗ · pubmed ↗