Robotic total knee arthroplasty with functional positioning safely addresses major coronal deformities: Comparable complications and survivorship
Luca Andriollo, Emanuele Diquattro, Christos Koutserimpas, Giovan Giuseppe Mazzella, Giulio Bonat, Elvire Servien, Cécile Batailler, Sébastien Lustig

TL;DR
Robotic-assisted knee replacement surgery works safely for patients with major leg deformities, offering similar outcomes to standard cases.
Contribution
The study demonstrates the feasibility of robotic TKA for severe deformities with comparable complication and revision rates.
Findings
Patients with deformities had similar complication and revision rates as controls.
Functional outcomes were better in the deformity group, though not clinically significant.
Postoperative alignment was less neutral in the deformity group but did not affect implant survival.
Abstract
Robotic‐assisted total knee arthroplasty (TKA) has emerged as a reliable strategy to improve surgical accuracy and enable functional alignment (FA), also referred to as functional knee positioning (FKP). However, its application in patients with major coronal plane deformities remains under‐investigated. This study aimed to evaluate complication rates, implant survival, radiographic outcomes and patient‐reported measures in patients with severe deformities undergoing robotic‐assisted TKA with FA/FKP principles compared to matched controls. A retrospective comparative study was conducted on patients who underwent robotic‐assisted TKA between March 2021 and February 2023 at a single high‐volume centre. Patients with ≥15° varus or ≥10° valgus deformity were included in the study group and matched 1:1 with controls presenting neutral alignment. All procedures used the Mako…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
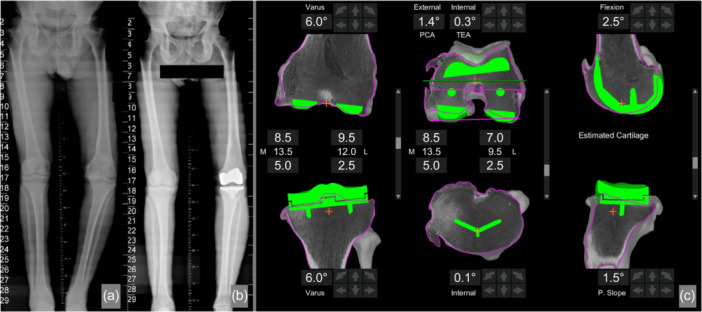 Figure 1
Figure 1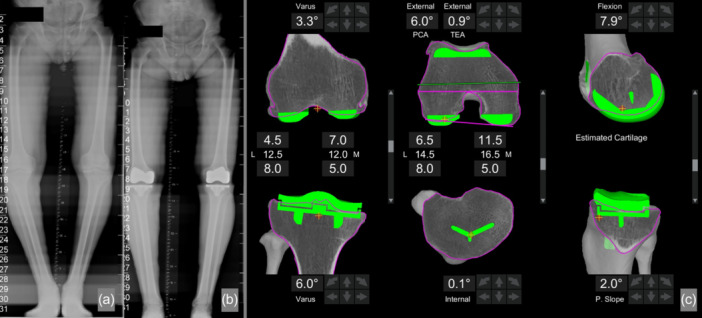 Figure 2
Figure 2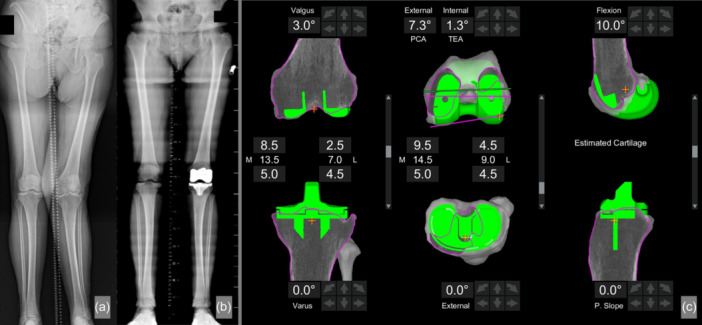 Figure 3
Figure 3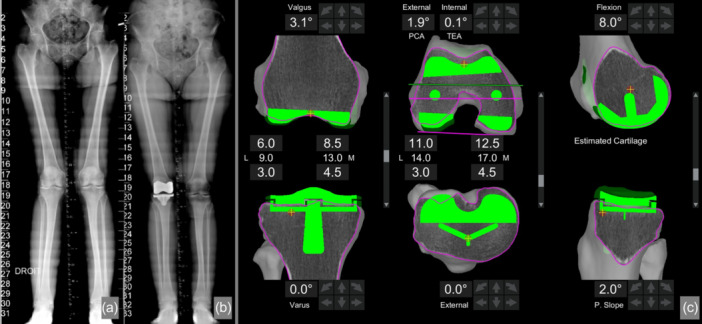 Figure 4
Figure 4| Study group ( | Control group ( |
| |
|---|---|---|---|
|
| |||
| Sex (female) | 65.9% (29) | 61.4% (27) | 0.83 |
| Age (years) | 70.5 ± 7.9 | 69.1 ± 11.5 | 0.11 |
| BMI (kg/m²) | 26.3 ± 4.4 | 27.8 ± 4.9 | 0.14 |
| CS liner | 40.1% (18) | 29.5% (13) | 0.38 |
| Follow‐up (years) | 2.9 ± 0.8 | 2.9 ± 0.8 | 0.42 |
|
| |||
| KSS knee | 62.8 ± 13.3 | 64.9 ± 11.7 | 0.45 |
| KSS function | 63.2 ± 14.2 | 64.0 ± 18.6 | 0.84 |
| Recurvatum (degrees) | 0.9 ± 2.5 | 0.6 ± 1.6 | 0.45 |
| Flexion contracture (degrees) | 1.6 ± 3.5 | 2.4 ± 4.3 | 0.36 |
| Maximum flexion (degrees) | 116.9 ± 19.0 | 119.7 ± 11.1 | 0.40 |
| mHKA (degrees) | 177.1 ± 14.5 | 179.1 ± 3.4 | 0.37 |
| LDFA (degrees) | 88.8 ± 5.2 | 92.1 ± 2.5 | <0.001 |
| MPTA (degrees) | 86.4 ± 5.9 | 88.5 ± 1.6 | 0.02 |
| TS (degrees) | 7.5 ± 3.0 | 7.3 ± 3.4 | 0.82 |
| Mako data on implant positioning | |||
|---|---|---|---|
| Values (degrees) | Study group ( | Control group ( |
|
| Femoral valgus | 0.2 ± 2.2 | 1.5 ± 1.7 | 0.002 |
| Femoral flexion | 7.4 ± 2.2 | 7.5 ± 2.6 | 0.92 |
| Femoral external rotation | 0.3 ± 1.6 | 0.1 ± 1.7 | 0.51 |
| Tibial varus | 2.7 ± 2.3 | 2.4 ± 1.5 | 0.39 |
| Tibial slope | 0.8 ± 1.0 | 0.7 ± 0.77 | 0.61 |
| Postoperative data | |||
|---|---|---|---|
| Study group ( | Control group ( |
| |
| KSS knee | 91.2 ± 16.0 | 91.0 ± 9.3 | 0.93 |
| KSS function | 90.7 ± 12.1 | 88.8 ± 10.5 | 0.42 |
| Recurvatum (degrees) | 0.6 ± 1.7 | 0.9 ± 1.8 | 0.53 |
| Flexion contracture (degrees) | 0.1 ± 0.8 | 0.2 ± 1.5 | 0.69 |
| Maximum flexion (degrees) | 126.0 ± 11.8 | 125.7 ± 11.0 | 0.89 |
| FJS‐12 | 83.9 ± 20.2 | 74.9 ± 19.0 | 0.04 |
| AKPS | 92.4 ± 13.6 | 88.2 ± 11.7 | 0.22 |
| mHKA (degrees) | 176.8 ± 4.7 | 180.0 ± 3.0 | 0.002 |
| LDFA (degrees) | 90.6 ± 2.8 | 91.3 ± 2.4 | 0.28 |
| MPTA (degrees) | 88.6 ± 2.7 | 88.7 ± 2.2 | 0.89 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Shoulder Injury and Treatment · Orthopaedic implants and arthroplasty
INTRODUCTION
Robotic‐assisted total knee arthroplasty (TKA) has shown promising results in recent years, particularly in enhancing surgical accuracy and patient‐reported outcome measures (PROMs) [8, 14, 28].
With robotic technology, it is now possible to pursue individualised or functional alignment (FA) strategies that account for three‐dimensional anatomy and soft tissue balance [1, 2, 3, 19]. Ensuring correct coronal alignment is essential for both functional improvement and long‐term implant survivorship [18, 20, 27].
Traditionally, severe varus or valgus deformities have been considered challenging in TKA, often leading to increased technical complexity, higher risk of residual imbalance, and the potential need for constrained implants [4, 7, 23, 26]. The standard goal has been to restore a neutral mechanical axis, but this approach may not always reflect patient‐specific anatomy [13, 29].
Robotic assistance provides surgeons with the ability to execute precise bone resections and tailor implant positioning, potentially reducing the need for extensive soft tissue release and offering more reproducible outcomes, even in anatomically complex knees [1, 2, 3]. Recent studies have demonstrated the feasibility of FA in robotic TKA. However, evidence specifically addressing cases with major deformities (≥15° varus or ≥10° valgus) remains limited [27].
In this study, patients with major coronal deformities were compared with those with standard alignment undergoing robotic‐assisted TKA performed with FA principles, also referred to as functional knee positioning (FKP). The primary endpoint was the comparison of PROMs between the two groups. Secondary endpoints included complication rates, implant survival and radiographic parameters. It was hypothesised that robotic TKA would achieve comparable safety profiles in complex deformities while potentially improving joint perception and functional recovery.
METHODS
This retrospective comparative study utilised a prospectively maintained database of patients who underwent robotic‐assisted TKA between March 2021 and February 2023. Patients were divided into two groups based on the presence or absence of major coronal plane deformities.
The study group included patients with a coronal plane deformity of ≥15° varus or ≥10° valgus, while the control group comprised patients with a mechanical hip‐knee‐ankle (mHKA) angle ranging between 166° and 179°. Preoperative coronal plane deformities were assessed using full‐length standing X‐rays.
All surgeries were carried out using the Mako robotic‐arm‐assisted system (Stryker, Mako Surgical Corp.). Every patient received a Triathlon Total Knee System implant (Stryker, Mako Surgical Corp.), with either a posterior stabilised (PS) or cruciate substituting (CS) liner. Procedures were performed at a single high‐volume centre with expertise in both primary and revision arthroplasty. A standardised surgical approach, following FA or FKP principles, was consistently applied [31, 32] (Figures 1, 2, 3, 4).
Seventy‐six‐year‐old female patient with a major varus coronal deformity, presenting a preoperative mechanical hip–knee–ankle (mHKA) angle of 161° on the left side, corrected to 167° after total knee arthroplasty (TKA). (a) Preoperative long‐leg standing radiograph; (b) postoperative long‐leg standing radiograph; (c) intraoperative screenshot of TKA performed with the Mako® robotic system (Stryker ®), showing planning adjustments according to functional knee positioning principles.
Seventy‐five‐year‐old male patient with a major varus coronal deformity, presenting a preoperative mechanical hip–knee–ankle (mHKA) angle of 161° on the right side, corrected to 171° after total knee arthroplasty (TKA). (a) Preoperative long‐leg standing radiograph; (b) postoperative long‐leg standing radiograph; (c) Intraoperative screenshot of TKA performed with the Mako® robotic system (Stryker ®), showing planning adjustments according to functional knee positioning principles.
Seventy‐three‐year‐old female patient with a major valgus coronal deformity, presenting a preoperative mechanical hip–knee–ankle (mHKA) angle of 192° on the left side, corrected to 185° after total knee arthroplasty (TKA). (a) Preoperative long‐leg standing radiograph; (b) postoperative long‐leg standing radiograph; (c) intraoperative screenshot of TKA performed with the Mako® robotic system (Stryker®), showing planning adjustments according to functional knee positioning principles.
Seventy‐two‐year‐old female patient with a major valgus coronal deformity, presenting a preoperative mechanical hip–knee–ankle (mHKA) angle of 188° on the right side, corrected to 187° after total knee arthroplasty (TKA). (a) Preoperative long‐leg standing radiograph; (b) postoperative long‐leg standing radiograph; (c) intraoperative screenshot of TKA performed with the Mako® robotic system (Stryker ®), showing planning adjustments according to functional knee positioning principles.
Patients were excluded if TKA was performed using mechanical alignment principles because of pre‐existing soft tissue issues, such as prior fractures, periarticular osteotomies, or major ligament injuries requiring deviation from FA. Further exclusions included patients with follow‐up shorter than 24 months and those with incomplete preoperative imaging or missing intraoperative robotic data to maintain consistency in the study methodology.
Demographic information, including age, gender and body mass index (BMI), was collected for all patients. Preoperative assessments included measurements of knee range of motion (ROM) and the knee society score (KSS) for both functional and clinical knee evaluation [16]. Imaging studies consisted of anteroposterior, lateral, Rosenberg, sunrise and full‐length standing X‐rays. From these images, the mHKA, lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA) and tibial slope (TS) were calculated [15]. Robotic system data provided detailed information on component positioning, using real‐time data obtained from preoperative CT scans. For the femoral component, parameters included flexion/extension relative to the mechanical axis (MA), varus/valgus alignment of the distal femoral cut and rotational alignment based on the surgical transepicondylar axis (sTEA). For the tibial component, varus/valgus alignment of the proximal cut and posterior tibial slope were assessed.
At the final follow‐up, clinical outcomes included KSS‐knee and KSS‐function scores, the Forgotten joint score (FJS‐12) and the Kujala anterior knee pain scale (AKPS), along with ROM measures for recurvatum, flexion contracture and maximum flexion [16, 24]. Data on septic and aseptic complications, reoperations and revision surgeries were also collected. A survival analysis of the implants was conducted, evaluating both all‐cause and aseptic revision rates between the study groups.
To ensure comparability between groups and minimise selection bias, a 1:1 nearest‐neighbour matching using a caliper of 0.5 units for continuous variables (age, BMI and follow‐up period). A total of 44 patients with major coronal plane deformity were included in the study group and matched with 44 patients from the control group based on similar demographic and preoperative characteristics. The groups, within the two respective analysed parameters, were compared in terms of clinical outcomes, radiographic measurements, robotic data and complication rates.
Ethical approval
This study was conducted in accordance with the ethical principles outlined in the 1964 Declaration of Helsinki and adhered to HIPAA regulations. Data collection and analysis were performed following the MR004 Reference Methodology established by the French Commission Nationale de l'Informatique et des Libertés (Ref. 2229975V0). Informed consent was obtained from all participants.
Statistical analysis
Continuous variables were reported as mean values with standard deviations (SD), while categorical variables were described using frequencies and percentages. The Shapiro–Wilk test was applied to assess the normality of data distribution. Depending on data distribution, comparisons between groups were performed using either the t‐test or the Mann–Whitney U test. Categorical variables were compared using the chi‐square test. Implant survival was examined to assess differences in revision rates between groups. A 95% confidence interval was used, and statistical significance was set at a p‐value < 0.05. All radiographic measurements were independently performed by two investigators, showing excellent interobserver reliability with intraclass correlation coefficients (ICCs) of 0.90 (95% CI: 0.86–0.94) for preoperative mHKA, 0.91 (95% CI: 0.87–0.95) for postoperative mHKA, 0.89 (95% CI: 0.84–0.93) for preoperative LDFA, 0.91 (95% CI: 0.87–0.94) for postoperative LDFA, 0.90 (95% CI: 0.85–0.94) for preoperative MPTA, 0.92 (95% CI: 0.88–0.95) for postoperative MPTA, and 0.89 (95% CI: 0.84–0.93) for posterior tibial slope. To define the minimal clinically important difference (MCID), the distribution‐based SD method was used, considering the MCID as equivalent to 0.5 × SD. All statistical analyses were conducted using Python version 3.11 (Python Software Foundation) and the statsmodels library (v0.13).
RESULTS
At the time of the final follow‐up, 88 patients were assessed, with a mean follow‐up duration of 2.8 ± 0.9 years. The cohort comprised 56 women (63.6%), with an average age of 68.8 ± 10.1 years and a mean BMI of 27.1 ± 4.7 kg/m². A CS liner was used in 31 cases (35.3%), while a PS liner was chosen in 57 patients (64.8%).
In the study group, 23 patients (52.3%) presented with major varus deformity, with a mean mHKA of 163.6 ± 2.5°, while 21 patients (47.7%) had major valgus deformity, with a mean mHKA of 192.0 ± 2.7°.
During the preoperative clinical evaluation, the mean KSS‐knee score was 63.9 ± 12.6, and the KSS‐function score averaged 63.2 ± 16.6. Regarding ROM, the mean recurvatum was 0.7 ± 2.1°, the mean flexion contracture was 2.0 ± 3.9°, and the mean maximum flexion reached 118.3 ± 15.3°.
In the preoperative radiographic assessment, the mean mHKA was 178.1 ± 10.4°, the LDFA was 90.5 ± 4.3°, the MPTA was 87.4 ± 4.4°, and the TS was 7.4 ± 3.3°.
Table 1 presents the comparison between the study group and the control group in terms of general and demographic characteristics, as well as preoperative clinical and radiographic data. Statistically significant differences were observed in LDFA (p < 0.001) and MPTA (p = 0.020).
The Mako data on tibial component positioning showed an average varus alignment of 2.5 ± 2.0° and an average slope of 0.7 ± 1.0°. For the femoral component, the mean valgus was 0.8 ± 1.9°, the average implant flexion was 7.5 ± 2.3°, and the mean external rotation was 0.2 ± 1.6°.
Table 2 presents data on implant positioning, following the principles of FA, also referred to as FKP. The only statistically significant difference was observed in the coronal plane alignment of the femoral component, which showed reduced valgus in the study group (0.2 ± 2.2° vs. 1.5 ± 1.7°, p = 0.002).
At the final follow‐up, patients in the study group reported a significantly higher FJS‐12 score compared to the control group (83.9 ± 20.2 vs. 74.9 ± 19.0; p = 0.04), indicating better joint perception. The overall FJS‐12 score was 79.7 ± 19.8, with a MCID of 9.9. Therefore, the difference of 9.0 points between the two groups does not reach clinical significance, as it falls below the MCID threshold. Radiographically, a significant difference in postoperative limb alignment was observed, with a less neutral mHKA in the study group (176.8 ± 4.7° vs. 180.0 ± 3.0°; p = 0.002). No other differences were observed. Table 3 reports the clinical and radiographic comparison between the two groups at the final follow‐up.
Four patients (4.5%) required manipulation under anaesthesia (MUA) or arthroscopic arthrolysis within 6 months postoperatively due to persistent stiffness. One patient (1.1%) underwent DAIR (debridement, antibiotics and implant retention) for an acute periprosthetic joint infection, while another (1.1%) required revision of the tibial component. The final implant survival rate was 97.7%, with only 2.3% of patients requiring partial or complete revision. No statistically significant differences were observed in terms of reoperation rate (9.1% vs. 4.5%, p = 0.668) or mechanical failure (2.3% vs. 0%, p = 0.987).
DISCUSSION
This study shows that robotic‐assisted TKA performed with FA principles can be applied reliably in patients with major coronal plane deformities, providing complication and revision rates comparable to those observed in patients with less severe deformities. These results are clinically relevant, since managing knees with large varus or valgus deviations has traditionally been considered more challenging, with concerns regarding residual imbalance, suboptimal implant positioning and higher risk of failure [6, 25]. By demonstrating no increase in adverse events, the findings support the safety of functional positioning even in complex anatomical situations and add evidence to the growing body of literature supporting robotic technologies in TKA [12, 22, 27, 35].
An important observation of this study concerns the PROMs. The FJS‐12 was significantly higher in patients with severe deformities compared to the control group, although the absolute difference did not exceed the MCID threshold. This suggests that while the magnitude of difference may not be sufficient to claim clear superiority in clinical terms, the subjective perception of improvement was greater in the study group. One possible explanation is that patients with major deformities start from worse functional and symptomatic conditions, as only partially captured by preoperative KSS scores, and therefore perceive the postoperative result more positively. This interpretation highlights the importance of considering baseline status when comparing PROMs across different patient subgroups and may reflect the fact that statistical significance does not always correspond to clinical relevance [30].
Recent evidence has shown that robotic‐assisted TKA can facilitate intra‐articular correction of severe extra‐articular deformities while reducing the need for extensive soft tissue release [10, 11, 36]. Although using an imageless robotic system, in a prospective series of 14 patients with femoral or tibial malunions, robotic TKA using a FA strategy achieved significant improvements in mechanical alignment and clinical scores, without major complications or the use of constrained implants. Notably, Oxford knee score (OKS) and KSS improved substantially at short‐term follow‐up [33].
Recent evidence has highlighted the impact of preoperative coronal alignment on intraoperative adjustments in robotic‐assisted image‐based TKA performed under FA principles. In a retrospective series of 355 knees, varus deformities required greater tibial varus positioning, whereas valgus deformities necessitated increased femoral valgus positioning and specific modifications in bone resections. Despite these distinct intraoperative strategies, postoperative functional outcomes, including KSS, FJS and AKPS, were comparable between varus and valgus knees, with implant survivorship exceeding 98% in both groups. These findings support the adaptability of FA in robotic TKA, demonstrating that individualised implant positioning can accommodate major deformities without compromising short‐term outcomes or implant longevity [20, 33].
Radiographic analysis also provides interesting insights. The postoperative mHKA was less neutral in the study group compared to controls (176.8 ± 4.7° vs. 180.0 ± 3.0°; p = 0.002), reflecting different correction patterns between groups. In particular, valgus deformities tended to be corrected toward neutral, while varus deformities were more often left in slight residual varus, generating outliers within the control cohort. These findings align with the principles of FA, which aim to balance the knee within an anatomically acceptable range rather than forcing all cases into strict mechanical neutrality [17, 31, 32].
Importantly, despite the presence of residual alignment variability, no negative impact on implant survival or complication rates was observed. This reinforces the concept that patient‐specific alignment strategies, facilitated by robotic assistance, may provide stable results without compromising safety and without an increase in early complications or revision rates, even in cases of extra‐articular or intra‐articular deformity, as demonstrated in other studies [5, 9, 33].
From a patient perspective, individuals with severe deformities may perceive a greater improvement in joint function, even if differences in PROMs do not exceed the thresholds for clinical significance [21]. From a radiographic perspective, the findings emphasise that residual varus in selected cases does not necessarily compromise clinical outcomes when the joint is balanced according to FA principles [34, 37].
This study has several strengths, including the use of a prospectively maintained database, standardised surgical techniques in a high‐volume centre, and robust radiographic and clinical follow‐up. One of the strengths of this study is one of the few studies to report both clinical outcomes and implant failure rates for total knee arthroplasties performed with an image‐based robotic system following FA principles in the presence of major lower limb deformities (≥15° varus or ≥10° valgus).
Limitations include its retrospective comparative design, the relatively short follow‐up of less than 3 years, and the limited sample size, which may reduce the ability to detect differences in rare complications or long‐term survival. Furthermore, only one validated PROM (FJS‐12) reached statistical significance, and the lack of additional quality‐of‐life measures may restrict the interpretation of subjective improvements. Future studies with larger cohorts and longer follow‐up will be important to determine whether the trends observed here persist over time and translate into clinically relevant differences in survivorship and patient satisfaction.
CONCLUSIONS
Robotic‐assisted TKA performed with FA/FKP principles appears to be a feasible option for patients with major coronal plane deformities, achieving short‐term complication and revision rates comparable to those observed in patients with preoperative neutral alignment. While patients with severe deformities reported higher FJS‐12 scores, this difference did not exceed the MCID threshold and should therefore be interpreted with caution. The radiographic differences observed in postoperative alignment suggest that respecting anatomical individuality rather than enforcing mechanical neutrality may be appropriate and does not increase early complication risks. These findings support the application of FA/FKP in complex primary TKA as a viable and reproducible strategy.
AUTHOR CONTRIBUTIONS
Luca Andriollo: Conceptualisation; methodology; data curation; writing original draft. Emanuele Diquattro: Conceptualisation; methodology; data curation; writing original draft. Christos Koutserimpas: Data curation and review; editing original draft. Giovan Giuseppe Mazzella: Data curation and review; editing original draft. Giulio Bonat: Data inspection. Elvire Servien: Supervision; reviewing and editing. Cécile Batailler: Supervision; reviewing and editing. Sébastien Lustig: Conceptualisation; supervision; validation; reviewing; editing.
CONFLICT OF INTEREST STATEMENT
Christos Koutserimpas is consultant for Smith and Nephew. Cécile Batailler and Elvire Servien are consultant for Stryker. Sébastien Lustig: Consultant for Stryker, Smith and Nephew, Heraeus, Depuy Synthes. Institutional research support to Lepine and Amplitude. Editorial Board for Journal of Bone and Joint Surgery. The remaining authors declare no conflicts of interest.
ETHICS STATEMENT
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee, the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Data collection and analysis were carried out in accordance with MR004 Reference Methodology from the Commission Nationale de l'Informatique et des Libertés (Ref. 2226075) obtained on April 19, 2022. The study was registered and filed on the Health Data Hub website. Written informed consent was obtained from all patients and/or families.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andriollo L , Gregori P , Koutserimpas C , Servien E , Batailler C , Lustig S . Beyond the coronal plane in robotic total knee arthroplasty‐Part 2: combined flexion does not affect outcomes. Knee Surg Sports Traumatol Arthrosc. 2025;33(8):2939–2949.40145260 10.1002/ksa.12660 PMC 12310087 · doi ↗ · pubmed ↗
- 2Andriollo L , Koutserimpas C , Gregori P , Servien E , Batailler C , Lustig S . Beyond the coronal plane in robotic total knee arthroplasty‐Part 1: variations in tibial slope and distal femoral flexion do not affect outcomes. Knee Surg Sports Traumatol Arthrosc. 2025;33(8):2928–2938.40130477 10.1002/ksa.12658 PMC 12310085 · doi ↗ · pubmed ↗
- 3Andriollo L , Koutserimpas C , Gregori P , Servien E , Batailler C , Lustig S . A new parameter in the era of robotic total knee arthroplasty: coronal alignment at 90° of flexion impacts clinical outcomes. Knee Surg Sports Traumatol Arthrosc. 2025;33(7):2581–2591.40099499 10.1002/ksa.12648 PMC 12205417 · doi ↗ · pubmed ↗
- 4Andriollo L , Picchi A , Demattia G , Marescalchi M , Sangaletti R , Benazzo F , et al. Imageless robotic surgery and a personalized approach: optimizing TKA after ACL reconstruction. Knee. 2025;57:353–360.41067207 10.1016/j.knee.2025.09.007 · doi ↗ · pubmed ↗
- 5Batailler C , Lording T , Libert T , Servien E , Lustig S . Achieving better clinical outcomes after total knee arthroplasty in knees with valgus deformity: the role of alignment strategies. J Bone Jt Surg. 2025;107(2):152–162.10.2106/JBJS.24.0020739591439 · doi ↗ · pubmed ↗
- 6Beckers G , Kiss M‐O , Massé V , Malavolta M , Vendittoli P‐A . Personalized total knee arthroplasty in patients with extra‐articular deformities. EFORT Open Rev. 2024;9(7):646–657.38949174 10.1530/EOR-23-0215 PMC 11297404 · doi ↗ · pubmed ↗
- 7Cholewinski P , Putman S , Vasseur L , Migaud H , Duhamel A , Behal H , et al. Long‐term outcomes of primary constrained condylar knee arthroplasty. Orthop Traumatol Surg Res. 2015;101(4):449–454.25952710 10.1016/j.otsr.2015.01.020 · doi ↗ · pubmed ↗
- 8Deckey DG , Rosenow CS , Verhey JT , Brinkman JC , Mayfield CK , Clarke HD , et al. Robotic‐assisted total knee arthroplasty improves accuracy and precision compared to conventional techniques. Bone Jt J. 2021;103–B(6 Supple A):74–80.10.1302/0301-620X.103B 6.BJJ-2020-2003.R 134053292 · doi ↗ · pubmed ↗