Failed anterior cruciate ligament reconstructions have both increased posterior tibial slope and increased posterior tibial plateau offset
Romed P. Vieider, Robert E. Bilodeau, Mahmut E. Kayaalp, Tyler M. Hauer, Karina Dias, Ting Cong, Jonathan D. Hughes, Volker Musahl

TL;DR
This study introduces a new measurement called posterior tibial plateau offset (PTO) and finds it correlates with the slope of the tibia in patients with failed ACL reconstructions.
Contribution
The study introduces the PTO as a new, reliable measurement that correlates with the posterior tibial slope.
Findings
PTO and posterior tibial slope showed a moderate positive correlation in both the ACL failure group and control group.
There was no significant difference in PTO between patients with ACL graft failure and the control group.
PTO is a simple and repeatable measurement with high inter-rater reliability.
Abstract
This study introduces the posterior tibial plateau offset (PTO). It was hypothesised that (1) the PTO is reliably quantifiable and (2) correlates with the posterior tibial slope (PTS). The study involved lateral radiographs of patients who sustained an anterior cruciate ligament (ACL) graft failure and a control group. Exclusion criteria were skeletal immaturity, osteoarthritis (Kellgren and Lawrence grade > I), lateral radiographs with <15 cm of tibial shaft, or malrotated radiographs. The PTS was measured in both groups. The PTO was defined as the relative distance from the posterior tibial plateau to the tibial shaft axis in relation to the sagittal diameter of the tibial plateau (in%). Linear correlation assessed the PTS to PTO association. A total of 146 patients (ACL graft failure, n = 103; control group, n = 43; 45% female, 60% left knees) were included. Mean overall PTO was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
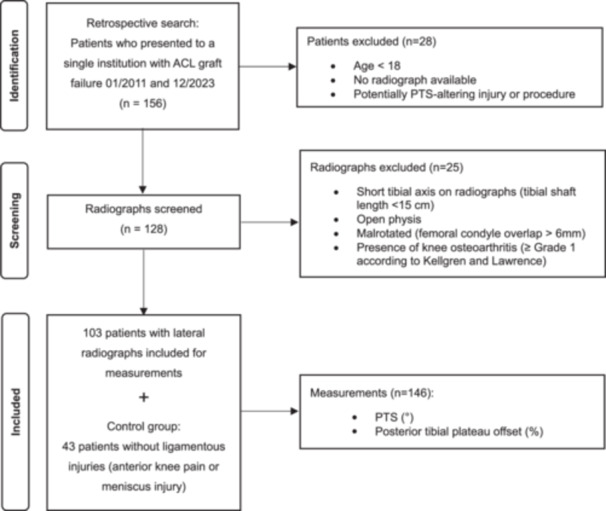 Figure 1
Figure 1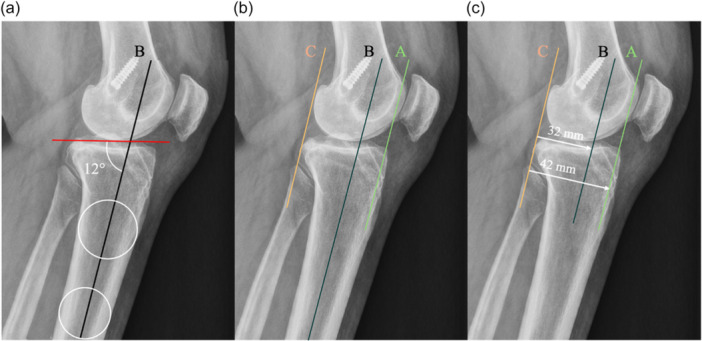 Figure 2
Figure 2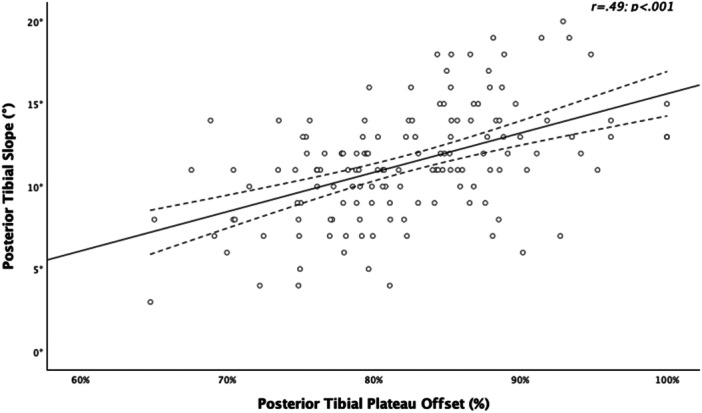 Figure 3
Figure 3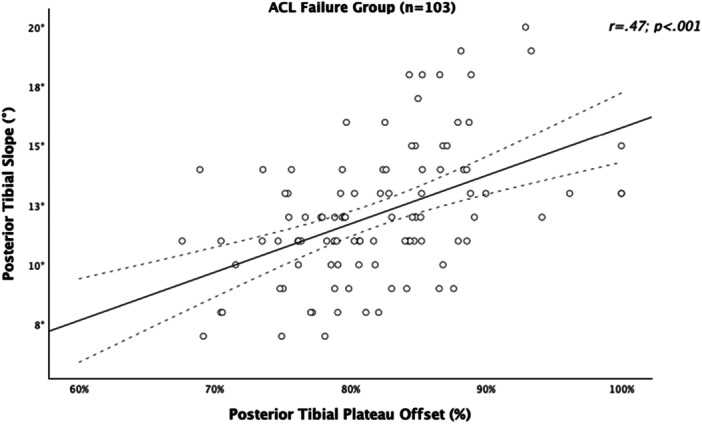 Figure 4
Figure 4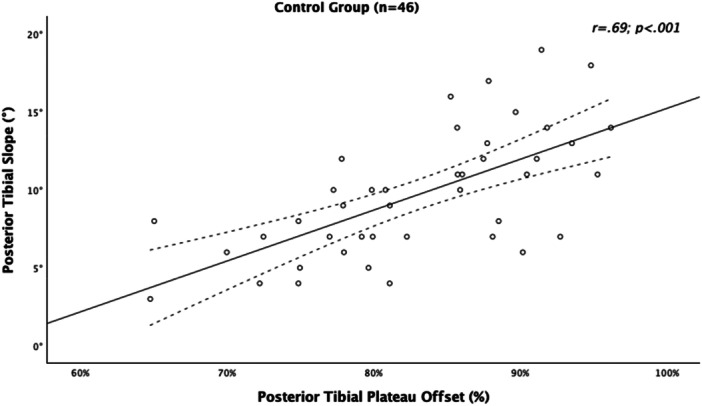 Figure 5
Figure 5| ACL graft failure + control group ( | |||
|---|---|---|---|
| Parameter | Mean ± SD | Min. | Max. |
| Age (years) | 31 ± 8 | 18 | 52 |
| Sex (female, | 60 (41%) | n/a | n/a |
| Laterality (left, | 68 (47%) | n/a | n/a |
| PTS (°) | 12 ± 4 | 3 | 20 |
| PTO (%) | 82 ± 7 | 65 | 99 |
| Distance P—A (mm) | 50 ± 6 | 35 | 72 |
| Distance P—tibial shaft axis (mm) | 42 ± 6 | 26 | 57 |
| ACL graft failure | |||
|---|---|---|---|
| Parameter | Mean ± SD | Min. | Max. |
| Age (years) | 30 ± 7.9 | 18 | 44 |
| Sex (female, | 39 (49%) | n/a | n/a |
| Laterality (left, | 46 (45%) | n/a | n/a |
| PTS (°) | 12 ± 3 | 7 | 20 |
| PTO (%) | 83 ± 6 | 66 | 94 |
| Distance P—A (mm) | 50 ± 7 | 39 | 63 |
| Distance P—tibial shaft axis (mm) | 42 ± 5 | 32 | 57 |
| Control group | |||
|---|---|---|---|
| Parameter | Mean ± SD | Min. | Max. |
| Age (years) | 41 ± 16 | 18 | 52 |
| Sex (female, | 21 (28) | n/a | n/a |
| Laterality (left, | 22 (51%) | n/a | n/a |
| PTS (°) | 10 ± 4 | 7 | 18 |
| PTO (%) | 82 ± 8 | 68 | 99 |
| Distance P—A (mm) | 51 ± 7 | 35 | 72 |
| Distance P—tibial shaft axis (mm) | 42 ± 7 | 26 | 56 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes · Osteoarthritis Treatment and Mechanisms
INTRODUCTION
A thorough understanding of the proximal tibial morphology is essential in knee‐preserving surgery [14, 15, 17, 25]. Several parameters have been described to quantify morphological characteristics of the proximal tibia [5, 6, 12, 13]. In the sagittal plane, the most frequently discussed parameter is the posterior tibial slope (PTS). The PTS quantifies the posterior inclination of the tibial plateau in relation to its shaft and is most frequently measured on a true lateral radiograph [10, 19, 24].
The PTS does not characterise the anteroposterior orientation of the tibial plateau related to the tibial shaft in the sagittal plane. The authors define this position as the posterior tibial plateau offset and aimed to propose a parameter to quantify the posterior tibial plateau offset (PTO) on the lateral radiograph. The variation in PTO may have important clinical implications. For example, differences in PTO could affect the required length of osteotomy cuts when planning an anterior closing wedge high tibial osteotomy (HTO). In addition, PTO variation may influence knee biomechanics and kinematics.
Therefore, this study aims to quantify the PTO on lateral radiographs. The purpose of this study was to define a repeatable measurement method to quantify the PTO. The study's hypothesis was (1) The PTO is reliably quantifiable, and it positively correlates with the PTS. (2) There is a high interindividual variability in PTO values.
METHODS
Lateral knee radiographs of all patients >18 years of age who presented with an anterior cruciate ligament (ACL) graft failure between 01/2022 and 12/2023 were included in the study. A control group was established for individuals who underwent lateral radiographs due to anterior knee pain or meniscus tears, but without ligamentous injuries, to account for confounding factors in the ACL graft failure group other than the PTS. Lateral knee radiographs with a short tibial shaft axis (tibial shaft length < 15 cm), malrotated radiographs (defined as a posterior femoral condyle overlap > 6 mm [26]), and radiographs from patients with knee osteoarthritis. Grade I or higher according to Kellgren and Lawrence [16], or a history of potentially PTS‐altering injuries or procedures, were excluded (Figure 1). Demographic data (age, sex and side) of the patients were analysed. All measurements were performed using the picture archive and communication system (PACS, Koninklijke Philips N.V.).
Flowchart of patient selection for the measurement of medial posterior tibial slope (PTS) and posterior tibial plateau offset in patients with anterior cruciate ligament (ACL) graft failure and the control group.
For each radiograph, the PTS was measured according to the most frequently used method (Figure 2a) [8, 23]. To determine the anatomical tibial shaft axis, two circles were placed at points 5 and 15 cm distal to the tibial joint surface, aligned with the anterior and posterior cortices. The midpoint of each circle was identified, and a line connecting these midpoints was defined as the anatomical tibial shaft axis. The PTS was defined as the angle between a tangent of the medial tibial plateau and a perpendicular line of the proximal tibial shaft axis (Figure 2a) [8].
True lateral radiograph of a left knee with high posterior tibial offset of 74%. (a) The medial posterior tibial slope was defined by the angle between the anatomical tibial shaft axis (B, black line) and a line tangent to the medial tibial plateau, measuring 12° in the current example. (b) The posterior tibia plateau offset was then determined as follows: First, the anterior (A, green line) and posterior (C, orange line) tibial articular margins of the plateau were identified, and parallel tangents to the tibial axis were placed. The margins (A and C) were located at the most anterior and posterior edges of the tibial joint surface. The tangent points were defined at the locations where the tibial joint surface begins to “fall off,” and the tangent lines were positioned accordingly. (c) The posterior tibial plateau offset was then determined by the distance between C and B (in image 1c: 32 mm) divided by the distance from C and A (in image 1c: 42 mm), which resulted in 0.74, meaning the anatomical axis intersects the tibial plateau at 26% from an anteroposterior perspective.
To assess the posterior offset of the tibial plateau, two lines parallel to the tibial shaft axis were drawn. The first line was positioned tangentially at the most anterior margin of the medial tibial plateau, while the second was placed at the most posterior margin of the medial tibial plateau. The distance between these two tangential lines and the distance from the tibial shaft axis to the posterior tangential line was measured in millimetres (Figure 2b).
To provide a normalised parameter for the tibial shaft axis position in relation to the tangential reference lines, the percentage was calculated by dividing the distance from the tibial shaft axis to the posterior tangential line by the total distance between the two tangential lines. This percentage was subtracted from 100 to enable standardised comparisons of the tibial shaft axis intersecting the tibial plateau across individuals (Figure 2c).
Statistical analysis
Descriptive statistics and tests for significance were calculated using SPSS 27.0 (IBM‐SPSS) and displayed by graphs and tables. After testing the data homogeneity of variance (Levene test) and normal distribution (Shapiro–Wilk test), continuous variables were presented as mean and standard deviation (normally distributed) or median and 25%–75% interquartile range (non‐normally distributed). A paired t‐test (normally distributed data) or Wilcoxon rank sum test (non‐normally distributed data) was used for group comparison of continuous variables. Due to the predefined ACL graft failure group, a power analysis was conducted for the control group to determine the necessary sample size for pairwise comparisons of the posterior tibial plateau offset measurement. Based on 10 preliminary measurements (PTO and PTS) in a sample of the control group, a mean effect size of d = 0.4 was detected with a two‐sided significance at α = 0.05. Achieving an adequate power (1‐β = 0.8) necessitated a sample size (n) of 43 radiographs, as determined by the analysis. A Pearson correlation was used to analyse the correlation between the PTS and posterior tibial plateau offset. The calculation utilised G*Power 3.1.9.6 software [8].
To determine the intrareader reliability PTS and posterior tibial offset measurements, a single rater (R.P.V.) performed the measurements at a time interval of 3 months between measurements, and the Pearson correlation coefficient was calculated. The intraclass correlation coefficient (ICC) of three raters (R.V., R.B. and T.H.) was calculated to assess the interrater reliability of the measurements and interpreted according to Koo and Li (<0.50 poor, 0.50–0.75 moderate, 0.75–0.90 good, >0.90 excellent) [17].
RESULTS
A total of 146 (n = 103 ACL graft failure, n = 43 control) patients were included in this study. Of the study population, 45% were female (n = 65) and 60% (n = 88) were left knees. The demographic data is visualised in Table 1. The mean posterior tibial offset was 82% ± 7% (65%–99%) and the mean PTS was 12° ± 3 (7–20). In the overall study group (ACL graft failure plus control group), the correlation analysis resulted in a significant correlation between the PTPO and PTS (r = 0.49, p < 0.001), indicating that higher posterior tibial plateau offset values were associated with higher PTS values (Figure 3). The same effect of a positive correlation of PTS with PTO was detected when separating the groups into ACL graft failure group (Table 2, Figure 4) and control group (Table 3, Figure 5). There was no statistical difference in PTO between the ACL graft failure (83%) and the control group (82%, p < 0.05). The interrater and interrater readability between the three raters for PTS and posterior tibial offset ranged from 0.8 to 0.9 (p < 0.05) for all measurements.
Scatter plot with a trendline (black line) and confidence intervals (dotted lines) illustrating the positive correlation of the posterior tibial plateau offset (%) and the posterior tibial slope (°).
Scatter plot with a trendline (black line) and confidence intervals (dotted lines) illustrating the positive correlation of the posterior tibial plateau offset (%) and the posterior tibial slope (°) of the anterior cruciate ligament (ACL) failure group.
Scatter plot with a trendline (black line) and confidence intervals (dotted lines) illustrating the positive correlation of the posterior tibial plateau offset (%) and the posterior tibial slope (°) of the control group.
DISCUSSION
The most significant finding of this study was the observation of a moderate, significant correlation between the PTPO and the PTS, indicating that knees with a higher PTS present with a greater posterior tibial plateau offset, which reflects a more posteriorly oriented tibial plateau. Furthermore, the posterior tibial plateau offset is a simple and repeatable measure of the posterior positioning of the proximal tibial plateau relative to the tibial shaft axis. The interindividual variability of the PTPS was high in patients who experienced an ACL graft failure and in a control group.
The morphology of the proximal tibia has significant biomechanical and clinical relevance, particularly in the context of ACL injuries [3, 14, 20]. Within the sagittal morphology of the tibia, the PTS is the most widely investigated parameter, with higher PTS values consistently reported in cohorts with ACL tears and graft failures [4, 7, 22]. However, PTS only describes the posterior inclination of the tibial plateau and not its posterior positioning relative to the tibial shaft. The present study adds to the current knowledge by quantifying this posterior positioning through the posterior tibial plateau offset, showing a higher PTPO, meaning a more posterior orientation of the tibial plateau in relation to the tibial shaft axis.
Multiple parameters were published to describe the proximal tibial morphology in addition to the PTS [1, 9, 21, 27]. One study investigated metaphyseal inclination and found a correlation between PTS and posterior metaphyseal tilt, showing that increased slope is associated with posteriorly inclined metaphysis [9]. The findings of the current study support the concept that the posterior inclination of the tibial plateau translates into a posterior positioning of the tibial plateau in relation to the tibial shaft. Another study has identified that tibial tubercle overgrowth and tibial tubercle height both positively correlated with PTS [21]. The PTPO does not take the tibial tubercle into account and may be seen as a complementary variable to the tibial tubercle height and angle.
A magnetic resonance imaging (MRI) based study showed that the posterior tibial offset ratio did not identify significant differences in ACL‐injured versus intact knees [27]. Notably, MRI‐based measurements are prone to underestimating the PTS. This occurs due to a more posteriorly tilted tibial shaft axis in the two‐circle method used. The method used to define the proximal tibial anatomical axis in the current study is a widely accepted method and the current gold standard in measuring the PTS. It does not rely on the tibial tubercle and benefits from a long tibial shaft axis, potentially offering a more anatomically accurate assessment [11, 19].
The correlation between posterior tibial offset and PTS may have clinical implications. As previous studies showed, an increased PTS leads to an increased strain on the ACL, ACL‐graft, and the posterior horn of the medial and lateral meniscus [2, 25]. An increased posterior tibial plateau offset may therefore be a factor that influences the load distribution in knee kinematics, especially in the context of anterior closing wedge HTOs. Another clinical implication may occur in osteotomy planning. A high posterior tibial plateau offset may pose challenges for infratubercle anterior closing wedge HTO, as the curvature of the posterior cortex may limit the ability to reach the desired hinge point. In turn, non‐optimal hinge placement may increase the risk of mal‐correction or hinge fractures, as this has been shown in medial opening wedge HTOs [18].
The PTS is currently one of the most discussed risk factors in ACL graft failure. Subjectively, the authors noted that the PTO also showed considerable variability. Therefore, the aim of this study was to quantify the PTO to support one aspect of the hypothesis: that the PTO correlates with the PTS in a cohort of ACL failures, which naturally demonstrate higher PTS values. The study also attempted to determine whether PTO correlates with PTS in a control group. In future studies with larger sample sizes, it could be investigated whether interchangeable or modifying effects exist between PTS and PTO (e.g., whether the risk of ACL graft failure in patients with high PTS is increased or reduced by a high PTO). This could help explain why many patients with high PTS values still have intact ACLRs.
This study has limitations that should be considered when interpreting the findings. First, the analysis was conducted on a specific patient group consisting solely of individuals who had ACL graft failure. Therefore, the PTS of this group was generally higher and may not reflect the general population. In this study, it was aimed to determine if the posterior tibial plateau offset increases with an increase in PTS and to assess the reliability and repeatability of measuring the posterior tibial offset. Second, the measurements were performed using two‐dimensional lateral radiographs, which provide information limited to the sagittal plane. This approach does not account for three‐dimensional variations in tibial morphology. The measurement technique in this study followed the current gold standard for measuring the PTS, and for an appropriate comparability, the measurements for the posterior tibial plateau offset were performed on radiographs too. Finally, the study focused exclusively on morphological parameters and did not assess their functional implications. The correlation between posterior tibial plateau offset and clinical and functional outcomes or biomechanical implications may be further investigated.
The strengths of this study include the implementation of a simple and reliable measurement method to quantify the PTO in clinical practice. This may have important clinical implications, such as for planning an anterior closing wedge HTO. The PTO could influence the angle and length of the osteotomy cuts. Finally, the study highlights the variability of the PTO in both a cohort with naturally higher PTS and a control group, demonstrating that this is not merely a morphological characteristic specific to one population.
CONCLUSION
The posterior tibial plateau offset is a simple and repeatable measure of the posterior positioning of the tibial plateau related to the tibial shaft axis. A higher PTS is associated with a higher posterior tibial plateau offset and the variability across the patients with ACL graft failure and the control group was high. When planning osteotomy levels in the highly sloped proximal tibia, surgeons may want to consider high offset variability to optimise individualised planning for patients with failed ACL reconstruction.
AUTHOR CONTRIBUTIONS
Romed P. Vieider: Conceptualisation; methodology; writing—original draft preparation; writing—review and editing. Robert E. Bilodeau: Methodology; writing—original draft preparation; writing—review and editing. Mahmut E. Kayaalp: Methodology; writing—review and editing. Tyler M. Hauer: Conceptualisation; methodology; writing—review and editing. Karina Dias: Writing—review and editing. Ting Cong: Writing—review and editing. Jonathan D. Hughes: Writing—review and editing. Volker Musahl: Conceptualisation; writing—review and editing; supervision.
CONFLICT OF INTEREST STATEMENT
Volker Musahl declares educational grants, consulting fees and speaking fees from Smith & Nephew plc, educational grants from Arthrex and DePuy/Synthes, is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and deputy editor‐in‐chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). Jonathan D. Huhges: Associate Editor of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA), paid consultant to Smith and Nephew, editorial board of Annals of Joint. Mahmut E. Kayaalp: Associate Editor of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA), Member of the ESSKA U‐45 Scientific Committee. The remaining authors declare no conflicts of interest.
ETHICS STATEMENT
Institutional Review Board approval was obtained by the University of Pittsburgh prior to the initiation of the study (STUDY19030196).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akti S , Akti S , Zeybek H , Celebi NO , Karaguven D , Cankaya D . Anterior metaphyseal angle; much less individual variation in determining the posterior slope of the tibia. J Orthop Sci. 2023;28:1046–1051.35864026 10.1016/j.jos.2022.06.017 · doi ↗ · pubmed ↗
- 2Amirtharaj MJ , Pourmodheji R , Wheatley MGA , Leluc J , Pechstein AE , Hirth JM , et al. Sagittal slope‐reducing high tibial osteotomy decreases anterior cruciate ligament force and coupled internal tibial rotation under pivoting loads: a computational modeling study. Am J Sports Med. 2025;53:1614–1621.40292779 10.1177/03635465251334649 · doi ↗ · pubmed ↗
- 3Bayer S , Meredith SJ , Wilson KW , De Sa D , Pauyo T , Byrne K , et al. Knee morphological risk factors for anterior cruciate ligament injury: a systematic review. J Bone Jt Surg. 2020;102:703–718.10.2106/JBJS.19.0053531977822 · doi ↗ · pubmed ↗
- 4Beel W , Schuster P , Michalski S , Mayer P , Schlumberger M , Hielscher L , et al. High prevalence of increased posterior tibial slope in ACL revision surgery demands a patient‐specific approach. Knee Surg Sports Traumatol Arthrosc. 2023;31:2974–2982.36622421 10.1007/s 00167-023-07313-2 · doi ↗ · pubmed ↗
- 5Brandon ML , Haynes PT , Bonamo JR , Flynn MI , Barrett GR , Sherman MF . The association between posterior‐inferior tibial slope and anterior cruciate ligament insufficiency. Arthrosc J Arthrosc Rel Surg. 2006;22:894–899.10.1016/j.arthro.2006.04.09816904590 · doi ↗ · pubmed ↗
- 6Chang TW , Huang CH , Mc Clean CJ , Lai YS , Lu YC , Cheng CK . Morphometrical measurement of resected surface of medial and lateral proximal tibia for Chinese population. Knee Surg Sports Traumatol Arthrosc. 2012;20:1730–1735.22048749 10.1007/s 00167-011-1749-9 · doi ↗ · pubmed ↗
- 7Dejour DH , Dan MJ , Cance N . Editorial commentary: posterior tibial slope‐reducing osteotomy should be considered in patients having primary anterior cruciate ligament reconstruction if posterior tibial slope is greater than 12° to 14°. Arthrosc J Arthrosc Rel Sur. 2025;41:3196–3199.10.1016/j.arthro.2025.03.00440081626 · doi ↗ · pubmed ↗
- 8Dejour H , Bonnin M . Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Jt Surg Br. 1994;76:745–749.8083263 · pubmed ↗