Prevalence, risk factors and trends of human schistosomiasis in Côte d’Ivoire from 1974–2023: systematic review and meta-analysis
Rufin K. Assaré, Fidèle K. Bassa, Jean T. Coulibaly, Nana R. Diakité, Mamadou Ouattara, Eliézer K. N’Goran, Jürg Utzinger

TL;DR
This study reviews 50 years of data to show that schistosomiasis in Côte d’Ivoire has decreased but still affects many people, especially in certain regions and among specific groups.
Contribution
The study provides the first comprehensive meta-analysis of schistosomiasis prevalence and risk factors in Côte d’Ivoire over five decades.
Findings
The pooled prevalence of schistosomiasis in Côte d’Ivoire is 26.1%.
Prevalence dropped from 66.5% in 1994–2003 to 15.0% in 2014–2023.
Key risk factors include being male, older age (>15 years), and living at low altitude (<400 m).
Abstract
Schistosomiasis is a parasitic worm infection that affects an estimated 250 million people. In Côte d’Ivoire, schistosomiasis remains a public health problem despite control efforts that have been mounted since the new millennium. The aim of this study was to assess the pooled prevalence of human schistosomiasis, to determine trends over the past 50 years and to identify risk factors for schistosomiasis. We systematically searched Google Scholar, PubMed, Scopus and Web of Science Core Collection without language restriction for papers published from January 1, 1974 to December 31, 2023. We adhered to Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines. We performed random effect models for meta-analysis and generated forest plots. Pooled schistosomiasis prevalences and corresponding 95% confidence intervals (CIs) were determined. Heterogeneity among studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
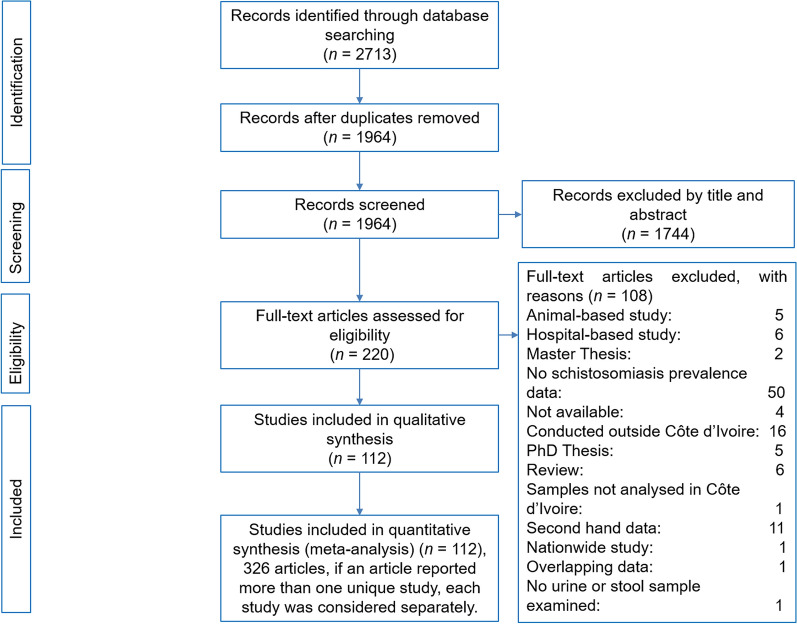 Figure 1
Figure 1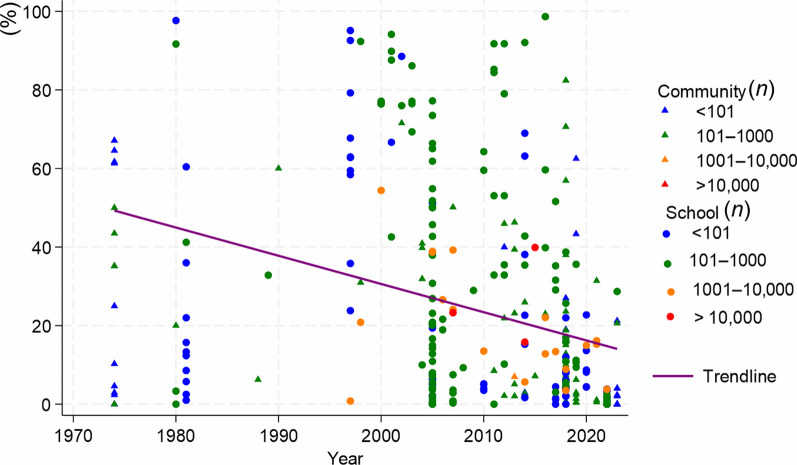 Figure 2
Figure 2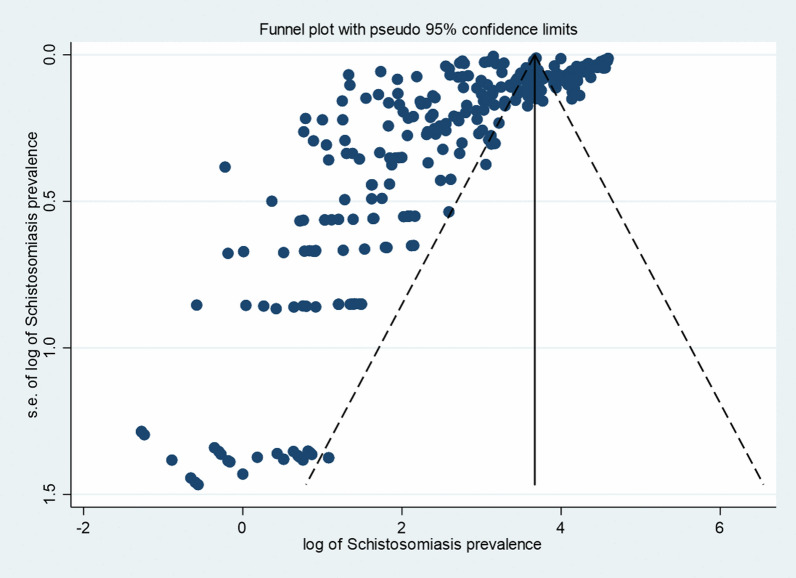 Figure 3
Figure 3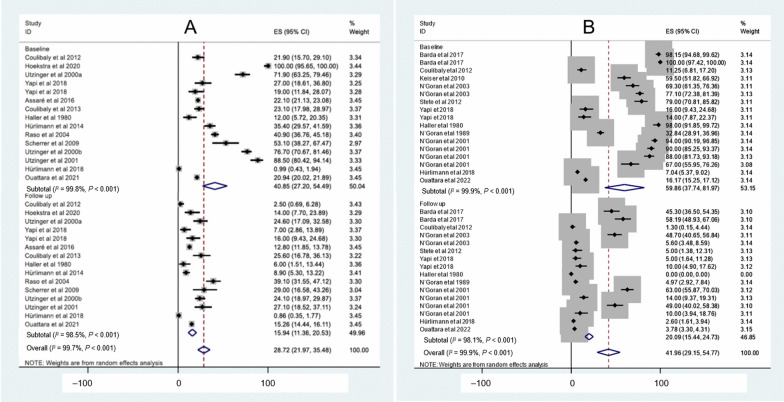 Figure 4
Figure 4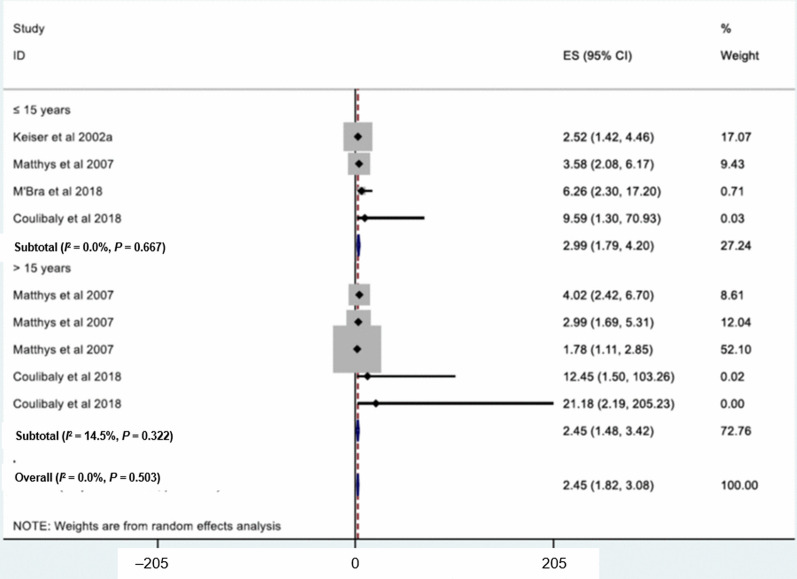 Figure 5
Figure 5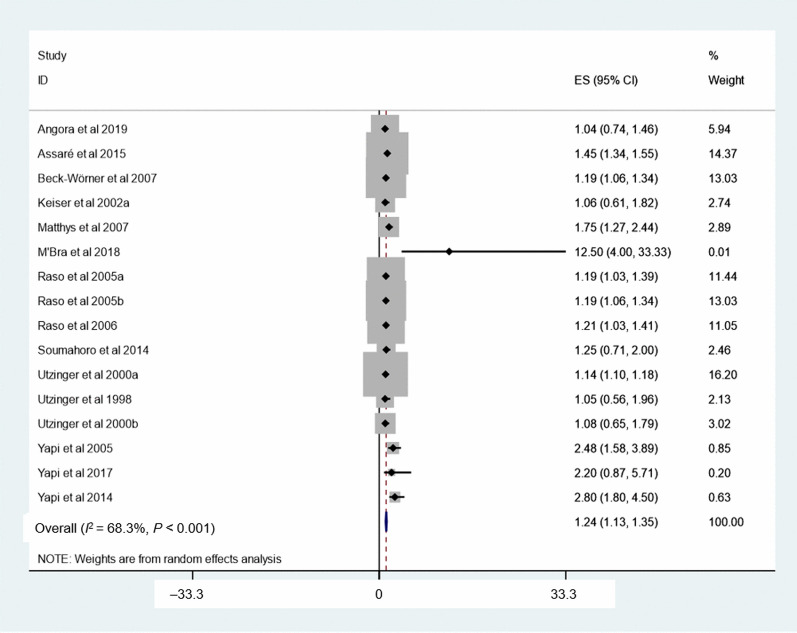 Figure 6
Figure 6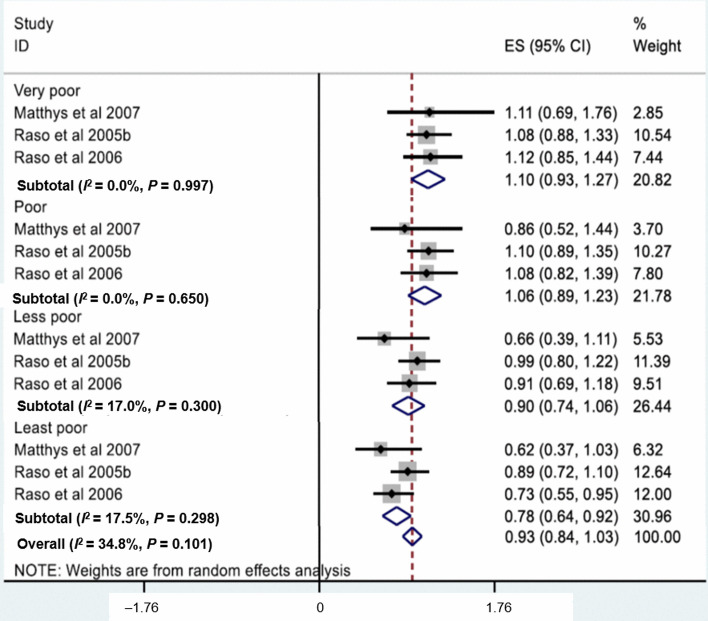 Figure 7
Figure 7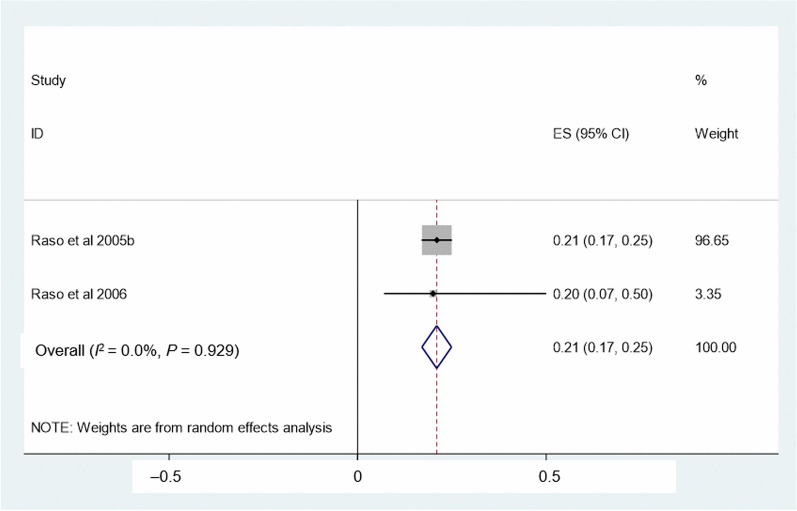 Figure 8
Figure 8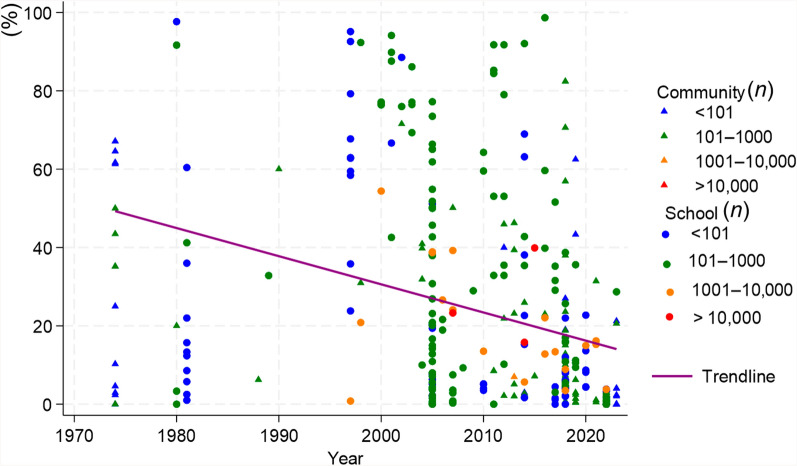 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Zoonotic diseases and public health · Parasite Biology and Host Interactions
Background
Schistosomiasis is endemic in 78 countries and constitutes a public health problem mainly in tropical and sub-tropical areas [1]. Schistosomiasis can lead to bladder cancer, infertility, hepatomegaly and splenomegaly [2–5]. In children, schistosomiasis is associated with anaemia, poor physical and delayed cognitive development. In 2013, an estimated 250 million people were infected worldwide with more than 80% concentrated in sub-Saharan Africa [6]. In 2021, the prevalence of schistosomiasis across Africa was estimated at 9.4% [7]. In Africa, schistosomiasis is mainly due to Schistosoma haematobium and S. mansoni. The latter causes intestinal schistosomiasis, while S. haematobium causes urogenital schistosomiasis. Hybridization within human schistosome species and between human and animal schistosomes have been reported in the western, central and southern parts of the continent, which highlight a potential zoonotic transmission of schistosomiasis [8–11]. Preventive chemotherapy with praziquantel is the mainstay of schistosomiasis control [12]. This strategy is pivotal for morbidity control and might also impact on transmission. However, re-infection can occur rapidly in the absence of ancillary measures. Hence, there is a need for integrated control approaches by combining preventive chemotherapy with provision of adequate water, sanitation and hygiene (WASH) facilities, behaviour change, communication and health education, and snail control [13–15].
In Côte d’Ivoire, schistosomiasis has been reported since the 1950s [16] and control efforts have been mounted by the Ivorian government to reduce the burden of the disease [17]. The first national schistosomiasis control programme was established in 1994 and included simultaneously human African trypanosomiasis and onchocerciasis within the frame of the West African Onchocerciasis Control Programme [17]. In 1998, the “Programme National de Lutte contre la Schistosomiase, les Géohelminthiases et la Filariose Lymphatique” was launched [17]. In 2012, the government of Côte d’Ivoire endorsed the London Declaration on Neglected Tropical Diseases and supported the World Health Organization (WHO) roadmap to prevent, control and eliminate schistosomiasis and other neglected tropical diseases. For effective implementation of preventive chemotherapy against parasitic worm infection in Côte d’Ivoire, the “Programme National de Lutte contre les Maladies Tropicales Negligées à Chimiothérapie Préventive” (PNLMTN-CP) was established in 2015, placing particular emphasis on schistosomiasis, soil-transmitted helminthiasis, onchocerciasis, lymphatic filariasis and trachoma.
Numerous parasitological assessments were carried out in Côte d’Ivoire since the 1970s to deepen the understanding of the epidemiology of schistosomiasis and to tailor control strategies to specific settings and population groups [14, 18, 19]. For instance, questionnaires, microscopic and antigen-based diagnostic approaches were evaluated for their accuracy in low-, moderate- and high-endemic settings [18, 20–22]. Recent studies showed that antigen-based methods might result in up to five-fold higher prevalence estimates of S. mansoni than the widely used Kato-Katz thick smear technique [23]. Several studies revealed that examination of repeated stool samples considerably increase the sensitivity of the Kato-Katz thick smear technique [24–26]. The Kato-Katz and urine filtration methods are the most widely used diagnostic approaches in research projects, such as mapping of schistosomiasis at different spatial scales, clinical trials to assess the efficacy of antischistosomal drugs and identification of disease risk factors [13, 27]. It was reported that socio-demographic, environmental and climatic factors, such as age, sex, socioeconomic status and altitude, might influence the occurrence, distribution and severity of schistosomiasis [28, 29]. Despite considerable efforts at administrative and research levels, the pooled prevalence and trends of schistosomiasis over time at the national level are poorly understood. In addition, prior studies often differed in terms of specific objectives, target population, sample sizes and diagnostic approach, among others.
The aim of this study was to estimate the pooled prevalence of schistosomiasis and the spatial distribution in the 20 regional health directorates of Côte d’Ivoire, and to assess trends over the past 50 years. Additionally, we determined risk factors of schistosomiasis. Results of this study will be useful for the PNLMTN-CP and schistosomiasis control and elimination efforts elsewhere in sub-Saharan Africa.
Methods
Protocol and registration
The protocol of this systematic review and meta-analysis was registered and is published on PROSPERO (https://www.crd.york.ac.uk/PROSPERO/view/CRD42021236785). The registration number is CRD42021236785. The following research question guided our review: What is the pooled prevalence of schistosomiasis in Côte d’Ivoire and how did it evolve over the past 50 years?
Search strategy
We systematically searched four readily available electronic databases (i.e. Google Scholar, PubMed, Scopus and Web of Science Core Collection) for articles published from January 1, 1974 to December 31, 2023 without language restriction. In Google Scholar, the search terms were “Côte d’Ivoire”, “schistosomiases*”, “schistosomiasis”, “prevalence” and “bilharziasis” for the period 1974–2023. The following search string ((schisto) OR (bilharzi*)) AND (Côte d’Ivoire) (filters: from 1974–2023), TITLE-ABS-KEY-AUTH ((Côte AND dʼIvoire) AND (schistosomiase OR schistosomiasis OR prevalence OR bilharziasis)) AND (EXCLUDE (PUBYEAR, 2024)) and TS = ((Côte dʼIvoire) AND (schistosomiase, OR schistosomiasis OR prevalence OR bilharziasis)) refined by: [excluding] PUBLICATION YEARS: (2024) were utilized in PubMed, Scopus and Web of Science Core Collection. The systematic review and selection of relevant literature were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines [30] (Additional file 1).
Inclusion and exclusion criteria
Studies were included if they (i) pursued a cross-sectional design; (ii) were school-based and/or community-based; (iii) were conducted in Côte d’Ivoire; (iv) assessed human schistosomiasis prevalence and/or risk factors; (v) had available data that could be used to evaluate schistosomiasis prevalence; and (vi) employed the Kato-Katz thick smear technique for S. mansoni or urine filtration for S. haematobium diagnosis.
Studies were excluded if they (i) were carried out in health facilities; (ii) were review articles; (iii) consisted of comments, letters, conference abstracts or interviews; (iv) were based on secondary data; and (v) reported prevalence of Schistosoma infection in non-human vertebrate hosts. Authors of original studies were not contacted for additional information. In case a publication reported more than one unique study, each study was considered separately [31].
Data extraction
One researcher performed the literature search (RKA). Articles were double-checked by another researcher (EKN), according to study inclusion and exclusion criteria. In case of discrepancies, a third researcher (JU) was involved and results discussed until consensus was reached. From each eligible study, the following information was extracted: title of the study, first author, year of publication, study location, health district, regional health directorate, study population (school-based or community-based), sample size, time of the study, diagnostic method, number of individuals who provided urine samples, number of *S. haematobium-*positive individuals, prevalence of S. haematobium, number of individuals who provided stool samples, number of S. mansoni-positive individuals and prevalence of S. mansoni.
Quality assessment
The quality of studies included was assessed by using the checklist of Joanna Briggs Institute (JBI) for prevalence studies quality assessment tools. The assessment tool used the following nine items: (i) sample frame appropriate to address the target population; (ii) study participants sampled in an appropriate way; (iii) adequate sample size; (iv) study participants and setting described in detail; (v) data analysis conducted with sufficient coverage of the identified sample; (vi) valid methods used for the identification of the condition; (vii) the condition was measured in a standard and reliable way for all participants; (viii) appropriate statistical analysis; and (ix) adequate response rate. The response of each parameter was scored 0 for “not reported” and 1 for “reported”. Total scores ranged between 0 and 9 [32].
Statistical analysis
Extracted data were entered into an Excel 2016 spreadsheet. Statistical analyses were performed using STATA version IC15.1 (Stata Corporation; College Station, TX, USA). Schistosomiasis prevalence estimates were reported with their corresponding 95% confidence interval (CI). For studies with number of participants examined and number of positive individuals, prevalence of schistosome species were estimated by multiplying the ratio of cases to sample size by a factor of 100. The 95% CI of schistosome prevalence was calculated using the exact binomial interval (http://statpages.info/confint.html accessed from 31 October 2023 to 31 January 2024).
Schistosomiasis risk factors were determined and expressed with odds ratio (OR). The relationship between schistosomiasis and the risk factors were estimated based on the pooled ORs. Statistical heterogeneity among the studies were assessed by Cochran’s Q test and I^2^ statistic test. I^2^ values of 25%, 50% and 75% were interpreted as low, moderate and high heterogeneity, respectively [33]. Cochran’s Q test with* P*-value (P) < 0.1 was considered to show statistically significant heterogeneity between studies [34]. Random effect models for the meta-analysis were used and forest plots generated. Forest plot, funnel plot and Egger’s test were generated using STATA version IC15.1 (Stata Corporation; College Station, TX, USA).
Subgroup analysis, heterogeneity and publication bias
Subgroup analysis was done based on study setting (school or community), regional health directorates, schistosome species (S. haematobium and S. mansoni) and study decade (1974–1983, 1984–1993, 1994–2003, 2004–2013 and 2014–2023). Publication bias was statistically examined with funnel plot and Egger’s test [35]. A P < 0.05 of the Egger’s test was considered as indication for the presence of publication bias.
Results
Description of included studies
Overall, 2713 articles were identified in the four electronic databases. After removing duplicates (n = 749) and non-relevant articles (n = 1852), 112 articles consisting of 326 unique studies fulfilled our inclusion criteria (Fig. 1). Among the 112 included articles, 96 articles (85.7%) and 13 (11.6%) were categorized as high quality and low quality, respectively (additional file 2).Fig. 1. Flowchart of the study selection. n: number
Study characteristics
All included studies had a cross-sectional design (additional file 3). Overall, 279,340 participants were included to estimate the pooled prevalence of schistosomiasis in Côte d’Ivoire. The sample size varied from 29 to 118,327 participants. The highest prevalence of schistosomiasis (98.7%) was reported in Azaguié Makouguié in Agboville health district belonging to Agnéby-Tiassa Mé regional health directorate. The lowest prevalence of infection (0.0%) was observed in 26 locations.
Among the 326 studies that provided data for this meta-analysis, it was not possible to identify the regional health directorates in 13 (4.0%) of the studies. The remaining 313 studies were reported from 17 regional health directorates. Most of the studies were carried out in Agnéby-Tiassa Mé, Tonpki, Abidjan 1 Grands ponts, Cavally-Guemon and Poro Tchologo Bagoué, where 96 (30.7%), 53 (16.9%), 36 (11.5%), 24 (7.7%) and 36 (11.5%) studies were reported, respectively. Studies with sample sizes exceeding 1000 individuals were predominantly school-based and carried out between 1994 and 2023 (Fig. 2). The prevalence of schistosomiasis decreased from 1974 to 2023. The shape of funnel plot of the studies was asymmetric, indicated the presence of publication bias, which was statistically evidenced by Egger’s test (P < 0.001) (Fig. 3).Fig. 2. Reported schistosomiasis prevalences in community and school-based studies from 1974 to 2023 in Côte d’Ivoire. n: sample sizeFig. 3Funnel plot of schistosomiasis studies. Egger’s test [ꞵ = 39.9 (95% CI: 33.7–46.1), P < 0.001]
Prevalence of schistosomiasis
There was considerable heterogeneity in the prevalence of schistosomiasis among the included studies (I^2^ = 99.6%, Cochran’s Q P < 0.001) (Table 1). Hence, a random effect model was employed and revealed that the pooled prevalence of schistosomiasis among all age categories in Côte d’Ivoire was 26.1% (95%* CI:* 24.2–27.9%).Table 1. Subgroup prevalence estimate for schistosomiasis in Côte d’IvoireVariablesSubgroups analysisN articlesN examinedPrevalence (%)95%* CI**I*^2^ (%)P-valueOverall326279,34026.124.2–27.999.6 < 0.001Study decades1974–1983313,16431.919.5–44.399.1 < 0.0011984–199331,28332.76.4–59.199.2 < 0.0011994–20033016,15566.553.2–79.899.8 < 0.0012004–201397159,47927.324.1–30.599.5 < 0.0012014–202316599,25915.012.7–17.199.3 < 0.001Regional health directoratesAbidjan 1 Grands ponts365,0972.91.3–4.691.1 < 0.001Abidjan 251,3054.4− 0.1 to 8.972.90.011Agnéby-Tiassa Mé9624,94634.629.3–39.899.6 < 0.001Bélier115,20626.420.1–32.898.2 < 0.001Tonkpi5333,85850.145.0–55.298.9 < 0.001Cavally-Guemon242,11411.68.0–15.185.7 < 0.001DRS13190,15816.811.3–22.299.9 < 0.001Gbêkê121,36013.15.7–20.696.1 < 0.001Gboklé Nawa San Pedro31,0802.5− 0.1 to 5.190.30.002Gôh24908.5− 4.0 to 21.086.40.007Hambol141,8844.62.3–7.091.0 < 0.001Haut-Sassandra7117013.60.3–26.998.0 < 0.001Indénié Djuablin41,26310.23.2–17.397.6 < 0.001Kabadougou Bafing Folon220018.2− 16.1 to 52.597.80.009Marahoué73,21011.27.5–14.992.5 < 0.001Poro Tchologo Bagoué365,96913.29.9–16.595.7 < 0.001Sud Comoé13013.33.8–30.70.0–Study populationSchoolchildren226254,95428.726.4–31.099.6 < 0.001Community9723,86619.517.1–21.898.3 < 0.001Pre-schoolchildren352016.64.0–29.193.7 < 0.001CI confident interval, DRS Studies carried out in differents regional health directorates, N number
Subgroup analysis
Table 1 summarises subgroup analyses that revealed stark differences in schistosomiasis prevalence between regional health directorates, time of surveys (decadal periods), study populations and schistosome species. Stratified by the decade of publication, approximately half of the articles (50.6%) were reported in the last decade (2014–2023). The highest prevalence of schistosomiasis was obtained between 1994 and 2003 (66.5%; 95% CI: 53.2–79.8%), while the lowest prevalence was observed between 2014 and 2023 (15.0%; 95%* CI:* 12.7–17.1%). Stratified by regional health directorates, the highest prevalence of schistosomiasis was observed in Tonkpi regional health directorate (50.1%; 95% CI: 45.0–55.2%), located in the western part of Côte d’Ivoire. The lowest prevalence of schistosomiasis was reported in Gboklé Nawa San Pedro (2.5%, 95% CI: − 0.1–5.1%) and Abidjan 1 Grands ponts (2.9%, 95% CI: 1.3–4.6%). Stratified by study population, the pooled prevalence of schistosomiasis was significantly higher among school-aged children (28.7%, 95% CI: 26.4–31.0%) compared to preschool-aged children (16.6%, 95%* CI:* 4.0–29.1%).
The prevalence of S. haematobium and S. mansoni, stratified by regional health directorate is summarised in Table 2. One third of the surveys pertaining to urogenital schistosomiasis were conducted in Agneby-Tiassa Mé regional health directorate (35.1%, 80/228). The pooled prevalence of S. haematobium in Côte d’Ivoire was 19.0% (95% CI: 17.3–20.8%) (Table 2). The highest prevalence of S. haematobium was 42.8% (95% CI: 36.6–49.2%), reported in Abidjan 1 Grands ponts. The largest number of S. mansoni surveys were found in Agnéby-Tiassa Mé (77 articles) and Tonkpi (51 articles) regional health directorates. The pooled prevalence of S. mansoni was 20.0% (95% CI: 18.1–21.9%) across Côte d’Ivoire (Table 2). The highest S. mansoni prevalence was reported in Tonkpi regional health directorate (45.5%, 95% CI: 40.4–50.7%).Table 2. Prevalence of S. haematobium and S. mansoni stratified by regional health directoratesRegional health directoratesS. haematobium**S. mansoniN articlesN examinedPrevalence (%)95% CIN articlesN examinedPrevalence (%)95% CIAbidjan 1 Grands ponts125042.836.6–49.2354,8470.70.2–1.1Abidjan 211080.051,3054.4− 0.1 to 8.9Agnéby-Tiassa Mé8019,20428.624.2–33.07720,96422.418.4–26.3Bélier115,20626.420.1–32.8104,7672.61.3–3.9Tonkpi314,47318.914.3–23.55132,83145.540.4–50.7Cavally-Guemon242,1642.61.1–4.1242,01611.57.9–15.0DRS6141,84414.17.3–21.010172,43717.411.1–23.8Gbêkê121,35712.65.4–19.997511.1− 0.1 to 2.3Gboklé Nawa San Pedro31,0802.5− 0.1 to 5.1Gôh24908.5− 4.0 to 21.0Hambol141,9662.30.8–3.71013196.22.7–9.6Haut-Sassandra681020.27.9–32.555561.2− 0.9 to 3.2Indénié Djuablin41,26310.23.2–17.3Kabadougou Bafing Folon220018.2− 16.1 to 52.5Marahoué62,8509.76.5–12.973,2108.15.0–11.1Poro Tchologo Bagoué366,1335.43.6–7.2355,82510.37.6–12.9Sud Comoé13013.33.8–30.7Total228186,36519.017.3–20.8290253,89120.018.1–21.9CI confident interval, DRS Studies carried out in differents regional health directorates, N number
The reported control or specific interventions for S. mansoni between 1974 and 2023 are shown in Table 3. There were 19 studies; 11 pertained to mass drug administrations (MDA), five were clinical trials, two focused on improved sanitation and one to MDA combined with WASH. The first intervention was conducted in 1980 in Mopé, while the most recent study pertaining to S. mansoni was implemented from October 2018 to 2019 in three villages of Taabo (Agnéby-Tiassa Mé regional health directorate). There were three studies without follow-up for S. mansoni prevalence, resulting in 16 studies for further analysis. The pooled prevalence of S. mansoni decreased from 40.9% (95% CI: 27.2–54.5%) to 15.9% (95% CI: 11.4–20.5%) (Fig. 4A).Table 3. Reported interventions for schistosomiasis mansoni control from 1974 to 2023 in Côte d’IvoireAuthorSettingStudy populationType of interventionDiagnostic methodDate of baselineDate of follow-upBaseline sample sizeBaseline S. mansoni prevalenceFollow-up sample sizeFollow-up S. mansoni prevalenceCoulibaly et al. 20122 villages in Azaguié < 6 yearsClinical trialKKJune 2011November 201116021.91602.5Coulibaly et al. 20175 villages of Azaguié2–5 yearsClinical trialKKNovember 2014February 201566024.0143Coulibaly et al. 20175 villages of Azaguié5–15 yearsClinical trialKKNovember 2014February 201522580.0174Hoekstra et al. 20203 villages of Taabo5–17 yearsClinical trialKKOctober 2018Janvier 201983100.08314.0Utzinger et al. 2000aFagnampleu6–15 yearsClinical trialKKDecember 1998June 199912871.912824.6Yapi et al. 2018BlanflaCommunityProductive sanitationKKJune 2014July 201610027.01007.0Yapi et al. 2018North DiacohouCommunityProductive sanitationKKJune 2014July 201610019.010016.0Adoubryn et al. 2012Biankouma4–15 yearsMDAKK2006200738635.5Agbaya et al. 2004Agboville4–15 yearsMDAKKFebruary 2001June 200136010.012.5Assaré et al. 20164 regions of westerrn Côte d’Ivoire9–12 yearsMDAKKDecember 2011 to January 2012May 2013701122.1466712.8Coulibaly et al. 20132 village in Azaguié < 6 yearsMDAKKAugust 2011November 201124223.18625.6Haller et al. 1980Mopé5–15 yearsMDAKK198019808612.0736.0Hürlimann et al. 2014Niabé (Abengourou)4–15 yearsMDAKKDecember 2012May 201325735.42198.9Raso et al. 2004Zouatta IICommunityMDAKKMay 2002June 200254540.916139.1Scherrer et al. 2009Douimbly and Zouatta II4–13 yearsMDAKKJune 2007July 20074953.14929.0Utzinger et al. 2000bFagnampleu6–14 yearsMDAKKNovember 1998December 199825376.725324.1Utzinger et al. 2001Gbatongouin and Mélapleu7–14 yearsMDAKKNovember 1997February 19989688.59627.1Hürlimann et al. 20185 villages South Center of Côte d’IvoireCommunityMDA and WASHKKJuly 2011August 128101.08100.9Ouattara et al. 202175 Locations Western Côte d’Ivoire9–12 yearsMDAKKDecember 2011 to January 20122016741020.9722315.3KK Kato-Katz technique, MDA mass drug administration, WASH water, sanitation, and hygieneFig. 4Forest plot of prevalence of Schistosoma species at baseline and follow-up of control studies conducted across Côte d’Ivoire.** A** Intervention for S. mansoni control. B Intervention for S. haematobium control
The reported intervention for the control of S. haematobium between 1974 and 2023 are summarised in Table 4. There were 19 studies, including nine clinical trials, seven MDA, two improved sanitation and one MDA plus WASH. The first study focusing on S. haematobium control was carried out in 1980 in Mopé (Agnéby-Tiassa Mé regional health directorate), while the most recent studies took place from November 2015 to 2019 in 64 villages in the northern and central parts of Côte d’Ivoire. There were three studies without follow-up of S. haematobium prevalence. Hence, 16 intervention studies were included in the analysis. The pooled prevalence of S. haematobium decreased from 59.9% (95% CI: 37.7–82.0%) to 20.1% (95% CI: 15.4–24.7%) (Fig. 4B).Table 4. Reported interventions for schistosomiasis haematobium control from 1974 to 2023 in Côte d’IvoireAuthorSettingStudy populationType of interventionDiagnostic methodDate of baselineDate of follow-upBaseline sample sizeBaseline S. haematobium prevalenceFollow-up sample sizeFollow-up S. haematobium prevalenceBarda et al. 20174 villages of Adzopé2–5 yearsClinical trialUrine filtrationNovember 2015May 201616298.212845.3Barda et al. 20174 villages of Adzopé6–15 yearsClinical trialUrine filtrationNovember 2015May 2016141100.012258.2Coulibaly et al. 20185 villages of Adzopé2–5 yearsClinical trialUrine filtrationNovember 2015February 201662829.6157Coulibaly et al. 20185 villages of Adzopé6–15 yearsClinical trialUrine filtrationNovember 2015February 201635645.7166Coulibaly et al. 20122 village in Azaguié < 6 yearsClinical trialUrine filtrationJune 2011November 201116011.31601.3Keiser et al. 2010GuéssiguiéAug 16Clinical trialUrine filtrationNovember 2008December 200817359.583N’Goran et al. 2003Taabo Village5–15 yearsClinical trialUrine filtrationNovember 2000July 200115669.315648.7N’Goran et al. 2003Taabo Village5–15 yearsClinical trialUrine filtrationNovember 2000June 200135477.13545.6Stete et al. 2012Grand Moutcho7–15 yearsClinical trialUrine filtrationMarch 2010June 201012479.0805.0Yapi et al. 2018BlanflaCommunityProductive sanitationUrine filtrationJune 2014July 201610016.01005.0Yapi et al. 2018North DiacohouCommunityProductive sanitationUrine filtrationJune 2014July 201610014.010010.0Haller et al. 1980Mopé5–15 yearsMDAUrine filtration198019808698.0730.0N’Goran et al. 1989N’Guessan PokoukroCommunityMDAUrine filtration1989198954532.83425.0N’Goran et al. 2001Taabo Village4–15 yearsMDAUrine filtrationMay 1997Octber 199722294.019063.0N’Goran et al. 2001Bodo4–15 yearsMDAUrine filtrationMay 1997Octber 199723690.020314.0N’Goran et al. 2001Batera4–15 yearsMDAUrine filtrationMay 1997Octber 199713788.012249.0N’Goran et al. 2001Assinzé4–15 yearsMDAUrine filtrationMay 1997Octber 19979067.07310.0Hürlimann et al. 20185 villages South Center of Côte d’IvoireCommunityMDA and WASHUrine filtrationJuly 2011August 20128107.08102.6Ouattara et al. 202264 villages of Northern and Central Côte d’IvoireCommunityMDAUrine filtrationNovember 20152016–2019609216.256893.8MDA mass drug administration, WASH water, sanitation, and hygiene
Risk factors for schistosomiasis
The relationship between age group and S. mansoni is shown in Fig. 5. Four studies were included to determine associations between age and S. mansoni. Children aged above 15 years had a higher odds of S. mansoni infection than their younger counterparts aged 6–10 years (OR = 2.45, 95% CI: 1.48–3.42). For the assessment of the relationship between sex and schistosomiasis, 15 studies were included. High heterogeneity was observed (I^2^ = 57.3%, P < 0.001), and hence, a meta-analysis with a random effect model was performed. There was a statistically significant association between sex and schistosomiasis with males at higher odds of Schistosoma infection than females (OR = 1.24, 95% CI: 1.13–1.35) (Fig. 6).Fig. 5. Forest plot for odds ratio of the association of age group with S. mansoni. Age group-reference: 6–10 yearsFig. 6Forest plot for odds ratio of the association sex with schistosomiasis. Sex reference: Female
Three studies were included to determine the association between socioeconomic status and schistosomiasis. Least poor individuals were less likely to be infected with Schistosoma spp. compared to the poorest quintile (OR = 0.78, 95% CI: 0.64–0.92) (Fig. 7). The odds of infection among poor individuals grouped into less poor, poor and very poor quintiles were 0.90 (95% CI: 0.74–1.06), 1.06 (95% CI: 0.89–1.23) and 1.10 (95% CI: 0.93–1.27), respectively, when compared to most poor as reference. The pooled OR showed that there was no significant association (OR = 0.93, 95% CI: 0.84–1.03).Fig. 7. Forest plot for socio-economic status with schistosomiasis
The relationship between altitude and schistosomiasis is shown in Fig. 8. The pooled OR showed that the odds of being infected with schistosome was much lower among people living at higher altitude (> 400 m) compared to those living at lower altitude (OR = 0.21, 95%* CI:* 0.17–0.25).Fig. 8. Relationship between altitude and schistosomiasis. Reference altitude: < 400 m
Discussion
We present the first systematic review and meta-analysis regarding the prevalence of human schistosomiasis in Côte d’Ivoire, including spatial and temporal trends and underlying risk factors. Most of the data stem from school-aged children and we found a pooled prevalence of schistosomiasis in Côte d’Ivoire of 26.1%. A recent systematic review and meta-analysis of schistosomiasis in school-aged children in Ethiopia found a slightly higher pooled prevalence of 28.8% [36]. In contrast, a systematic review coupled with a geospatial analysis assessing the spatial distribution of schistosomiasis and treatment needs in sub-Saharan Africa, reported significantly lower prevalence of schistosomiasis in Côte d’Ivoire (17.4%) [37]. In 2011, a geospatial analysis estimating the prevalence of schistosomiasis among children and adolescents below 20 years in West Africa reported a prevalence of 19.5% for Côte d’Ivoire [38]. A considerably lower prevalence of schistosomiasis was observed in national parasitological surveys conducted in Côte d’Ivoire (8.9%) and Kenya (2.1%) [39, 40]. The pooled prevalence of schistosomiasis in Côte d’Ivoire was significantly lower than results of a systematic review done in Zambia (47.5%) and a national survey carried out in Sierra Leone (42.2%) [41, 42]. The difference in the reported countrywide schistosomiasis prevalence estimates might be due to differences in study methodologies, WASH indicators, socioeconomic status, environmental characteristics of the countries and MDA coverage [7, 12, 43, 44].
Our findings showed that the pooled prevalence of schistosomiasis in Côte d’Ivoire was approximately halved from 1974 to 2023. In addition, the analysis of the reported intervention studies for the control of S. haematobium and S. mansoni revealed that urogenital and intestinal schistosomiasis were two-fold lower in recent years compared to the situation towards the end of the last millennium. The most likely explanation of this observation is that the national schistosomiasis control programme (PNLMTN-CP), emphasising MDA with praziquantel targeting school-aged children, showed success. In addition, water bodies in some locations have been treated with the molluscicide niclosamide, while communities in schistosomiasis endemic settings were sensitized to follow WASH strategies in order to prevent the disease [45, 46].
Our results revealed highest prevalence rates of schistosomiasis in the Tonkpi regional health directorate (50.1%). This observation confirms results of previous studies carried out in Côte d’Ivoire, which reported Schistosoma infection prevalence ranging from 50 to 100% [47–49]. Historically, intestinal schistosomiasis due to S. mansoni was the predominant schistosome species in this region, explained by environmental factors providing suitable conditions for the development of Biomphalaria pfeifferi, the intermediate host snail of S. mansoni. Moreover, most people in western Côte d’Ivoire practiced open defecation and several water contact activities in freshwater bodies such as bathing, washing clothes, crossing rivers, fishing and fetching water for domestic and agricultural use, which drive environment contamination and expose people to schistosome infection [19, 50].
Our subgroup analyses showed that schistosomiasis prevalence in preschool-aged children was higher than 10% (i.e. 16.6%). Moderate and high prevalence of schistosomiasis in preschool-aged children have been reported in previous epidemiological assessment in Côte d’Ivoire (31.4%), Ethiopia (14.6%) and Tanzania (60.6%) [51–53]. A systematic review and meta-analysis quantifying schistosomiasis infection in preschool-aged children in sub-Saharan Africa for the past 20 years revealed that the pooled prevalence of the disease was 19% [54]. These findings provide an evidence-base to include preschool-aged children in a comprehensive package of schistosomiasis control. Our findings also showed that the prevalence of schistosomiasis is higher among school-aged children compared to preschool-aged children. This observation corroborates with other studies from sub-Saharan Africa. Indeed, the prevalence of Schistosoma infection increases from early childhood with a peak usually observed at the age of 8–15 years, depending on the overall intensity of infection and decreases in adolescents and adulthood depending on setting-specific socioeconomic and behavioural factors [24, 52, 55, 56].
Findings on the analysis on relationship between age and schistosomiasis showed that there was strong association between age and schistosomiasis infection with older children at higher odds of infection compared to their younger counterparts. This observation might be explained by the characteristic of the study population. Indeed, in the study areas, older children practiced fishing and swimming in freshwater bodies and were involved in farming with their parents in irrigation schemes [57–60]. Hence, they were more exposed to schistosome cercariae than their younger counterparts.
The results of our systematic review and meta-analysis showed that males were more likely infected with schistosomes than females (OR = 1.24). A systematic review investigating the association between schistosomiasis pooled prevalence among Ethiopian school-aged children found that boys were more likely to be infected with schistosomes than girls (*OR *= 1.6) [36]. In addition, in a recent systematic review analysing 123 studies with prevalence and intensity of S. haematobium and S. mansoni infection showed that males were significantly more likely to be infected than females [61]. One plausible explanation is that males had higher frequency of contact with contaminated freshwater bodies and engaged in outdoor activities (e.g. fishing, swimming and irrigation farming) more often than females [14, 62, 63]. Other explanations could be religious and sociocultural reasons that limit water contact activities of females [64], and the adventurous nature of males who spent more time away from their homes than females [65].
The findings of our study further revealed that least poor individuals were less likely to have an infection with schistosome compared to the poorest quintile (OR = 0.78). A previous study conducted in Uganda evaluating the association between socioeconomic status and schistosomiasis reported that the odds of being infected for the lowest wealth quintile was 10.4 times higher compared to the highest wealth quintile (OR = 10.42). [66]. These data indicate that wealthy persons were less likely to have Schistosoma infection. A plausible explanation for this finding is that wealthy persons have limited contact with infected water bodies and have better access to health services and praziquantel treatment. This observation confirms that schistosomiasis is a poverty-related disease and improving the socioeconomic status of communities could help to decrease significantly the burden of schistosomiasis.
Our study showed that the odds of being infected with schistosome were much lower among people living at higher altitude (> 400 m) compared to those living at lower altitudes (OR = 0.21). A negative association between altitude and schistosomiasis prevalence was also found in the western part of Côte d’Ivoire, the western part of Ethiopia, the south-western part of Tanzania and the north-eastern part of the Democratic Republic of the Congo [28, 29, 67–69]. It is suggested that higher altitude leads to higher water velocity and cooler temperature of water bodies that present unsuitable habitat conditions for schistosomiasis intermediate host snails.
Strengths and limitations
Our study has several limitations that are offered for consideration. First, the sample size in some studies was low, which in turn could affect the estimated pooled prevalence of schistosomiasis and the validity of the obtained results. Second, no prior systematic review and meta-analysis assessing schistosomiasis prevalence and risk factors in Côte d’Ivoire was available for comparison. Third, the inclusion of studies using more sensitive diagnostic methods such as point-of-care circulating cathodic antigen urine cassette test for S. mansoni could result in higher pooled prevalence estimates of schistosomiasis. Fourth, data from 9 studies overlapped in different regional health directorates, which limit the subgroup analysis at regional health directorate scale. Lastly, data available from PNLMTN–CP and other non-governmental agencies were not considered because we only used data from published articles for replicability reason. Hence, care is indicated while interpreting the results of our meta-analysis.
Strengths of our study are that we adhered to the PRISMA guidelines, employed random effect models for meta-analysis and covered a large time frame of half a century. The marked decline of the prevalence of human schistosomiasis over the past 50 years in Côte d’Ivoire is encouraging. Data presented here will be shared, uploaded and curated by the Global Neglected Tropical Diseases database [70] for continued update and refinement of schistosomiasis geostatistical analysis at different spatial scales across Africa.
Conclusion
The systematic review and meta-analysis presented here showed moderate prevalence of human schistosomiasis in Côte d’Ivoire. Moderate prevalence was also reported among preschoolers. Hence, the study highlights the need to include preschool-aged children in control programmes and the availability of a paediatric formulation of praziquantel is welcomed. The main risk factors for schistosomiasis are age (> 15 years), male gender, living in low-income households and low altitude (< 400 m). The quality of the sampling method is an important parameter that should be considered in epidemiological investigations of schistosomiasis. We encourage public health decision makers in Côte d’Ivoire to improve surveillance and tailor control efforts to high-risk communities, in order to further reduce the burden of the disease. Future studies should assess the prevalence, intensity and burden of schistosomiasis, the intermediate host snails and species abundance and distribution in the context of climate change and continuous efforts with integrated control approaches.
Supplementary Information
Supplementary Material 1.Supplementary Material.2.Supplementary Material 3.