Multi‐Chamber Intracardiac Thrombi Complicated With Pulmonary and Lower Extremity Thrombosis in Male Patient: Case Report and Literature Reviews
Eba Fufa, Yitagesu Getachew, Samson Mulugeta, Abera Birhanu, Abel Yirga, Amdemeskel Mersha, Banchiaymolu Damtie, Balew Arega, Begashaw Belay, Brook Fanuel, Misgana Lukas

TL;DR
A rare case of multi-chamber heart blood clots leading to lung and leg clots is reported, emphasizing the need for careful treatment.
Contribution
Presents a rare clinical case of multi-chamber intracardiac thrombi with systemic embolization in a male patient.
Findings
Multi-chamber intracardiac thrombi can occur in dilated cardiomyopathy despite normal heart rhythm.
Such cases pose significant risks of hemodynamic compromise and systemic embolization.
Abstract
Multi‐chamber intracardiac thrombi are a rare and high‐risk complication in dilated cardiomyopathy, even during sinus rhythm. This case highlights the associated dangers of hemodynamic compromise and systemic embolization. Management requires vigilant anticoagulation and close monitoring to balance thromboembolic and bleeding risks.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
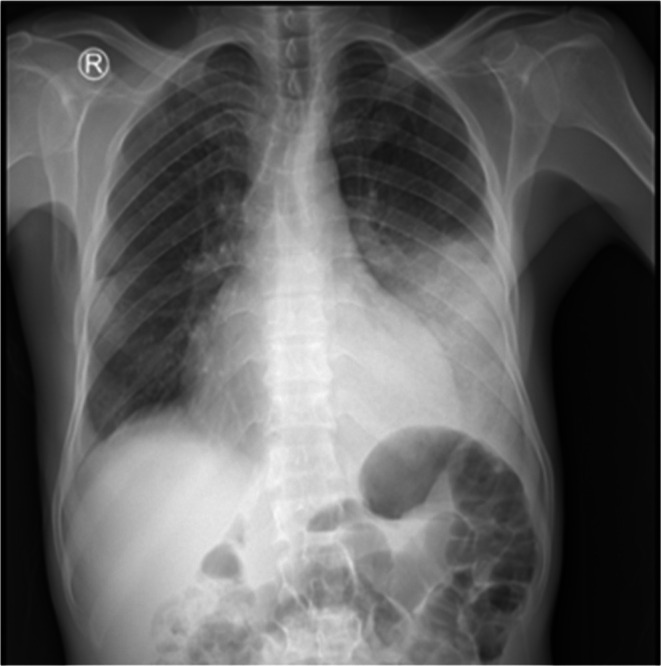 FIGURE 1
FIGURE 1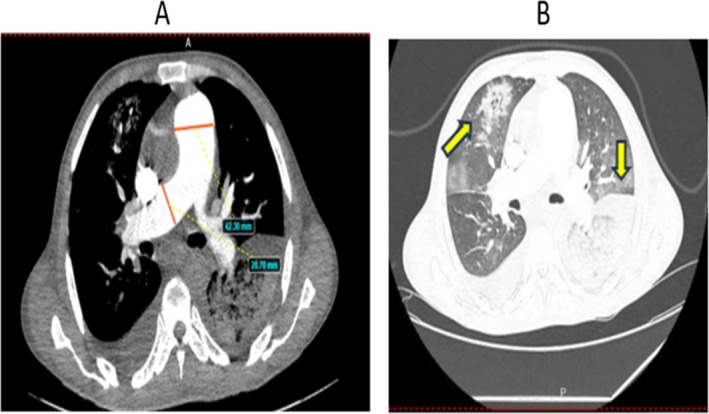 FIGURE 2
FIGURE 2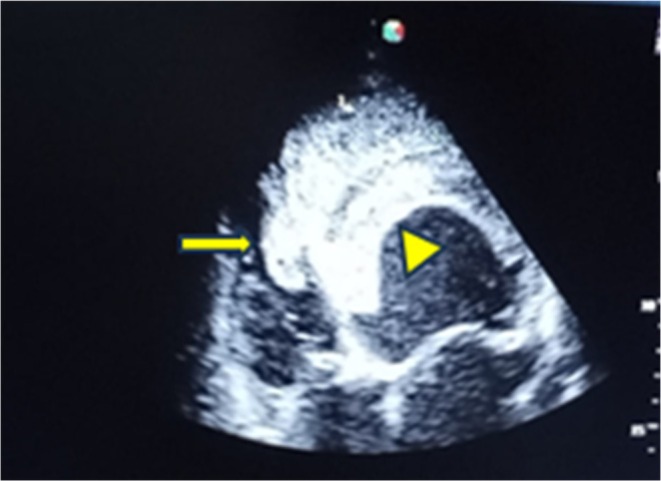 FIGURE 3
FIGURE 3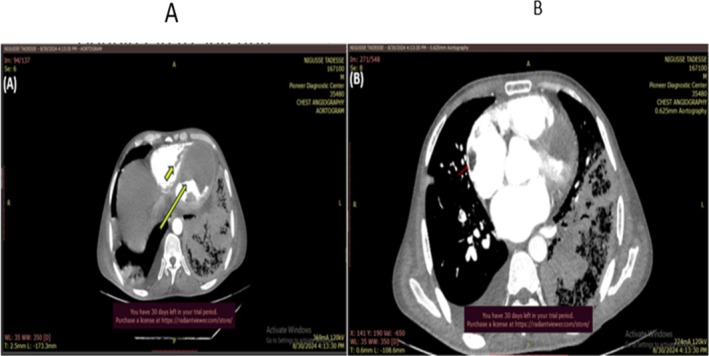 FIGURE 4
FIGURE 4| Laboratory tests | Done on the day of admission | 3 days after admission | Last updated after admission |
|---|---|---|---|
| White blood cell ( | 23.9 | 16 | 27.73 |
| Neutrophil (%) | 89.3 | 90.2 | 89.9 |
| Lymphocyte (%) | 4.6 | 5.1% | 5.2 |
| Monocyte (%) | 6.1 | 4.7% | 4.9 |
| Red blood cells ( | 4.69 | 4.15 | 3.62 |
| Hemoglobin (mg/dL) | 13 | 10.5 | 9.2 |
| Hematocrit (%) | 35.2 | 30.1 | 26.4 |
| Mean corpuscular volume (fl) | 75 | 72.5 | 72.9 |
| Mean corpuscular hemoglobin (pg) | 27.7 | 25.2 | 25.5 |
| Platelets ( | 168 | 213 | 205 |
| Prothrombin time | 21 | 18 | 21.8 |
| Activated partial thromboplastin time | 43.5 | 36.7 | 39.4 |
| International normalized ratio | 1.76 | 1.5 | 1.82 |
| Creatinine (mg/dL) | 1.17 | 0.8 | 1.3 |
| Blood urea (mg/dL) | 32 | 31 | 27 |
| Aspartate aminotransferase (μ/L) | 223 | 107 | 107 |
| Alanine aminotransferase (μ/L) | 282 | 131 | 146 |
| Alkaline phosphatase (μ/L) | 268 | 383 | 390 |
| Total bilirubin (mg/dL) | 3.33 | 2.63 | 3.99 |
| Direct bilirubin (mg/dL) | 1 | 1.14 | 1.18 |
| Potassium (mEq/L) | 2.71 | 3.29 | 3.46 |
| Sodium (mEq/dL) | 136.51 | 133 | 138 |
| Studies | Sex/age | Chamber involved | Others site thrombosis | Diagnosis and comorbidities | Management (anticoagulant) | Treatment outcome |
|---|---|---|---|---|---|---|
| Ida et al. (2014) [ | M/55 | All chambers | PTE | Ischemic CMP, atrial flatter, PFO | LMWH and mechanical thrombectomy | Died in the hospital |
| Singh et al. (2015) [ | M/48 | All chambers | No other sites of thrombosis | Alcoholic CMP | Anticoagulated | Survived |
| Elikowski et al. (2020) [ | M/60 | RV, RA, LV | PTE | Dilated CMP | Apixaban | Survived |
| Valle et al. (2015) [ | F/22 | RV, LV, LA | PTE | Peripartum dilated CMP | Warfarin and thrombi resolved | Survived |
| Agac et al. (2011) [ | M/22 | All chambers | No other sites of thrombosis | Acute myocarditis | Not mentioned | Died in the hospital |
| Kunkler et al. (2013) [ | M/74 | RA, LA, RV | Bilateral PTE, DVT | CAD, HPN, PFO | UFH with Warfarin | Survived |
| Izaga et al. (2020) [ | M/47 | All chambers | Bilateral PTE, DVT | PFO | UFH, embolectomy, and PFO closure | Survived |
| Nishigawa et al. (2011) [ | M/74 | LA, RA, LV | No other sites of thrombosis | HPN, Atrial fibrillation | Cardiopulmonary bypass and right atrial atriotomy, UFH | Survived |
| Shah et al. (2022) [ | F/27 | LA, LV, RV | DVT | COVID‐19 and DCP | Survived |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Aortic Thrombus and Embolism · Venous Thromboembolism Diagnosis and Management
Introduction
1
Intracardiac thrombosis is a blood clot in the heart that may occur de novo in any of the four cardiac chambers, including atrial appendages [1]. The underlying mechanisms for intracardiac thrombus formation have been attributed to either blood stasis or hematological abnormalities causing hypercoagulability [2]. Multi‐chamber intracardiac thrombi can develop among severe heart failure (HF) patients who are at risk of static blood flow, endothelial dysfunction, and increased hypercoagulable status [3]. Patients with dilated cardiomyopathy, myocardial infarction, and peripartum cardiomyopathy are at risk of developing intracardiac thrombosis [4], but it is extremely rare with sinus rhythm [5]. Coexistent thrombi in the right ventricle (RV) and right atrium (RA) can rarely be found among patients with left ventricle (LV) thrombus. Such patients have an increased risk of systemic and pulmonary embolism [6].
Vitamin K antagonists (VKAs), predominantly warfarin, have traditionally been used and recommended for the prevention and treatment of LV thrombus, but there is a growing interest in replacing VKAs with direct oral anticoagulants (DOACs) such as apixaban, rivaroxaban, edoxaban, and dabigatran [1]. There are a few anecdotal reports and retrospective small case series of surgical excision of LV thrombus [7]. On the other hand, the optimal medical or surgical treatment of right heart thrombi remains unclear, with limited experience with catheter‐directed thrombectomy [8, 9]. The therapy of multi‐chambered intracardial thrombi is challenging because these individuals are complicated with hemodynamic derangements, including shock, acute embolic events that can have cerebral effects, or systemic embolic events with increased mortality or morbidity if left untreated [10].
We describe dilated cardiomyopathy with huge tri‐chamber intracardiac thrombi involving LV, RV, and RA, and other site thrombosis, including lower extremity and pulmonary vein thrombosis, of an adult patient who presented to our hospital. This unusual example demonstrates the relevance of blood stasis as the cause of thrombus development in cardiac chambers, as well as a learning case for clinicians in the management of a huge tri‐chamber intracardiac thrombus in resource‐limited settings.
Case History and Examinations
2
A 40‐year‐old male Ethiopian farmer presented with a three‐month history of progressive easy fatiguability, a loss of appetite, and epigastric pain associated with significant but unquantified weight loss. Over the past 2 months before admission, he developed a dry intermittent cough that worsened with lying down, exertional shortness of breath (SOB), orthopnea of two pillows, paroxysmal nocturnal dyspnea (PND), and progressive asymmetric lower extremity swelling, more on the right leg.
Since the past 2 weeks before visits to Yekatit 12 Hospital Medical College's adult emergency department, the cough became productive of frothy sputum mixed with blood, which progressed to frank hemoptysis of clotted blood over the course of 1 week. In addition, he had SOB that occurs at rest and sleeps in a semi‐sitting position due to worsening orthopnea. He also complained of intermittent high‐grade fever and decreased urine output, but no color change. Otherwise, he had no known multimorbid illness, no risky behavior like smoking or alcohol drinking, or illicit as well as traditional medications. He was not treated for tuberculosis (TB). His COVID/vaccine status is unknown, but he has no history of flu‐like symptoms. He was married and a farmer from a rural area. He had never been admitted for a similar complaint. He lost his older brother 5 years ago at the age of 45 with a similar disease course, but he was not diagnosed. He died with massive blood coming from his mouth and nose at home, according to his description.
The patient's Glasgow Coma Scale (GCS) was 15 out of 15, and there were no memory, power, or tone abnormalities. The patient was in respiratory distress with an oxygen saturation of 80% with atmospheric air, a respiratory rate of 25 to 28 breaths/min, and a pulse rate of 109–129 beats per minute. He had no record of fever at presentation but had a low blood pressure of 80/50 mmHg with a regular, weak radial pulse.
Chest examination revealed bilateral coarse crepitus over the lower two‐thirds of the posterior chest and decreased air entry over the left lower posterior third. On the cardiovascular examination, jugular venous pressure was raised with no added sound in the pericardial examination. The abdominal examination revealed positive signs of fluid collection with no palpable organ. Abdominopelvic ultrasound showed only minimal ascites. He had grade II pitting edema, and his right and left legs had a three‐centimeter discrepancy.
Methods
3
Chest X‐ray showed cardiomegaly, left middle, and lower lung field homogenous opacity (Figure 1). Chest computed tomography angiography (CTA) showed enlarged bilateral pulmonary arteries and their lobar branches, and bilateral lungs with multiple large pulmonary infarctions, the largest at the left lower lobe, with bilateral mild pleural effusions (Figure 2A,B).
Erect posterior to anterior chest X‐ray showing cardiomegaly with left middle‐lower homogeneous opacity and right side costo‐phrenic angle blunting.
Enlarged bilateral pulmonary arteries and their lobar branches (A) and bilateral lungs with multiple large pulmonary infarctions, the largest at the left lower lobe (B).
The electrocardiogram showed left axis deviation with poor R‐wave progression. Echocardiography revealed a global LV wall hypokinesis suggestive of non‐ischemic dilated cardiomyopathy with reduced biventricular systolic function (EF of 20% and TAPSE of 13 mm) and secondary mild mitral and tricuspid regurgitation. There is a large left ventricular thrombus (43 by 58 mm) and a solitary laminar right ventricular thrombus (10 × 34 mm) (Figure 3). A transesophageal echocardiogram was not performed due to the patient's critical and unstable condition. Therefore, a patent foramen ovale (PFO) could not be definitively ruled out. The diagnosis of multi‐chamber thrombi was made by transthoracic echocardiogram (TTE), though the images were suboptimal due to the patient's clinical state. Ischemic etiology was excluded based on clinical assessment, a normal ECG without signs of ischemia, and negative serial troponin levels, as coronary angiography was not feasible.
A 2‐dimensional echocardiographic picture showing a large left ventricular thrombus (arrowhead) and a solitary laminar right ventricular thrombus (arrow).
The cardiac CT scan was not done due to persisting tachycardia, but chest CTA reported a large LV thrombus (11.5 × 7.5 cm) with markedly dilated LV (7.2 cm), RV thrombus (3.6 × 1.6 cm), and two right atrial thrombi (2.3 and 1.4 cm) (Figure 4). Doppler ultrasound of the right lower extremity reported acute proximal deep vein thrombosis. Serial determination of complete blood count and liver enzymes and bilirubin showed a raised value (Table 1).
Large LV thrombus (11.5 × 7.5 cm) (long arrow) with markedly dilated LV, RV thrombus (3.6 × 1.6 cm) (short arrow) (A), two right atrial thrombi (2.3 and 1.4 cm) (red arrow) (B).
Serum albumin was 2.6 g/dL. The coagulation profile is not significantly deranged. Cardiac troponin is normal. The lipid profile showed triglyceride, 51 mg/dL, total cholesterol, 87 mg/dL, high‐density lipoprotein, 22 mg/dL, and low‐density lipoprotein, 30 mg/dL. Lactate dehydrogenase (LDH) level was within normal limits (123 U/L).
Conclusion and Results
4
He was admitted to the adult intensive care unit (ICU) with the diagnosis of cardiogenic shock, acute decompensated HF secondary to dilated cardiomyopathy with reduced ejection fraction precipitated by severe community‐acquired pneumonia, tri‐chamber intracardiac thrombi, acute bilateral pulmonary thromboembolism, and right leg proximal acute deep vein thrombosis. He was started on (noradrenaline) standard doses of potent antibiotics (vancomycin and cefepime), hydrocortisone, unfractionated heparin infusion, intravenous furosemide, spironolactone, gastrointestinal prophylaxis, analgesics, and low‐dose morphine for cough suppression. Following a multidisciplinary review, fibrinolysis was contraindicated due to the high risk of catastrophic embolization from mobile ventricular thrombi and the significant hemorrhage risk from the patient's coagulopathy.
After 5 days of admission, he developed hematemesis from multiple episodes of upper gastrointestinal bleeding. Medical management was instituted, and unfractionated heparin was held. On serial determination, there was no significant change in the coagulation profile. Unfortunately, he succumbed to cardiac arrest 24 h after the onset of hematemesis. Endoscopic evaluation and intervention were not possible as he was not hemodynamically stable enough to be moved out of the ICU.
Discussion
5
This report details an adult man's case of non‐ischemic dilated cardiomyopathy with cardiogenic shock, tri‐chamber huge intracardiac thrombi, pulmonary thromboembolism, and left leg deep vein thrombosis. The patient was evaluated with echocardiography and CT angiogram, electrocardiography, cardiac biomarkers, and additional laboratory testing.
Similar to our findings, previously thrombi involving the LV, RV, and RA were simultaneously reported among case reports of patients with dilated CMP [6]. Other case reports documented the occurrence of thrombi in two atria and the LV [11, 12], the two ventricles and LA [12, 13], and involving all cardiac chambers [13, 14, 15, 16]. Premortem diagnosis of thrombi in three cardiac chambers at the same time in patients with pulmonary emboli is extremely rare, and we are aware of only a few case reports. In agreement with our finding, two other case reports documented bilateral PTE and DVT in addition to multiple intracardiac thrombi [12, 16]. The outcome of patients complicated with pulmonary embolism and multiple chamber thrombosis on the background of advanced HF is expected to be poor. Our patient developed cardiogenic shock, and despite appropriate management with the involvement of experienced cardiologists, he died in the hospital. Similarly, two case reports documented the in‐hospital mortality of patients diagnosed with multiple cardiac chamber thrombi [2, 15]. The distribution of intracardiac thrombi, chamber involved, treatment outcomes, and clinical presentation are presented in Table 2.
Veins of the lower extremities are classic sources of pulmonary embolisms and the thrombi in the right heart chambers. However, in the presence of PFO, the thrombus had migrated from the IVC and also migrated to the left heart. In our patient, there is no evidence of a patent foramen ovale on echocardiography and chest CTA assessment. In our patient, the source of the right chamber thrombi and thereby pulmonary embolism might have originated from the DVT in the right leg, which likely formed as a result of prolonged immobility from his severe heart illness.
On arrival at the hospital, the patient was hemodynamically unstable in cardiogenic shock, and a multidisciplinary team opted for conservative management with unfractionated heparin, management of the shock, and heart failure. We cannot further investigate the patient for possible other hypercoagulable factors, including proteins C and S, because there are signs of liver injury affecting the reliability of the finding.
In conclusion, timely identification and management of intracardiac thrombus in cardiomyopathy is of immense importance, as this condition may be fatal. Management in such uncommon cases remains challenging, and the complete scenario should always be taken into consideration. A multidisciplinary consensual approach should be encouraged. Emergency surgical management, with systemic anticoagulation, might save the lives of patients.
Author Contributions
Eba Fufa: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation. Yitagesu Getachew: conceptualization, data curation, formal analysis. Samson Mulugeta: conceptualization, data curation, formal analysis, methodology. Abera Birhanu: conceptualization, data curation, formal analysis, methodology. Abel Yirga: conceptualization, data curation, investigation, methodology. Amdemeskel Mersha: conceptualization, data curation, writing – original draft. Banchiaymolu Damtie: conceptualization, data curation, investigation. Balew Arega: conceptualization, data curation, formal analysis, investigation, writing – original draft, writing – review and editing. Begashaw Belay: conceptualization, data curation, investigation, methodology. Brook Fanuel: conceptualization, data curation, visualization, writing – original draft. Misgana Lukas: conceptualization, data curation, formal analysis, investigation, methodology.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. N. Levine , J. W. Mc Evoy , J. C. Fang , et al., “Management of Patients at Risk for and With Left Ventricular Thrombus: A Scientific Statement From the American Heart Association,” Circulation 146 (2022): E 205–E 223, 10.1161/CIR.0000000000001092.36106537 · doi ↗ · pubmed ↗
- 2M. Zhai , L. Huang , L. Liang , et al., “Clinical Characteristics of Patients With Heart Failure and Intracardiac Thrombus,” Frontiers in Cardiovascular Medicine 9 (2022), 10.3389/FCVM.2022.934160.PMC 958276436277765 · doi ↗ · pubmed ↗
- 3M. A. Talle , F. Buba , and C. O. Anjorin , “Prevalence and Aetiology of Left Ventricular Thrombus in Patients Undergoing Transthoracic Echocardiography at the University of Maiduguri Teaching Hospital,” Advances in Medicine 2014 (2014): 1–8, 10.1155/2014/731936.PMC 459096626556424 · doi ↗ · pubmed ↗
- 4A. Y. Lin , E. Dinatolo , M. Metra , et al., “Thromboembolism in Heart Failure Patients in Sinus Rhythm: Epidemiology, Pathophysiology, Clinical Trials, and Future Direction,” JACC. Heart Failure 9 (2021): 243–253, 10.1016/J.JCHF.2021.01.009.33714744 · doi ↗ · pubmed ↗
- 5W. Elikowski , M. Małek‐Elikowska , N. Fertała , et al., “Multichamber Intracardiac Thrombi Were Successfully Treated With Apixaban in a Patient With Dilated Cardiomyopathy and Sinus Rhythm,” Polskie Archiwum Medycyny Wewnętrznej 130 (2020): 997–999, 10.20452/PAMW.15577.32820883 · doi ↗ · pubmed ↗
- 6G. Pierre‐Justin and L. A. Pierard , “Management of Mobile Right Heart Thrombi: A Prospective Series,” International Journal of Cardiology 99 (2005): 381–388, 10.1016/j.ijcard.2003.10.071.15771917 · doi ↗ · pubmed ↗
- 7L. M. Burgos , J. P. Costabel , V. Galizia Brito , et al., “Floating Right Heart Thrombi: A Pooled Analysis of Cases Reported Over the Past 10years,” American Journal of Emergency Medicine 36 (2018): 911–915, 10.1016/J.AJEM.2017.10.045.29111332 · doi ↗ · pubmed ↗
- 8P. S. Rose , N. M. Punjabi , and D. B. Pearse , “Treatment of Right Heart Thromboemboli,” Chest 121 (2002): 806–814, 10.1378/CHEST.121.3.806.11888964 · doi ↗ · pubmed ↗