Falciform Ligament Appendagitis: A Rare Cause of Acute Epigastric Pain
Ahmed A Alali, Hamza M Ahmed

TL;DR
A rare case of acute epigastric pain caused by falciform ligament appendagitis is reported, highlighting its diagnostic challenge and successful conservative treatment.
Contribution
This case report adds to the limited literature on falciform ligament appendagitis, emphasizing its clinical presentation and management.
Findings
Falciform ligament appendagitis can present with severe epigastric pain and RUQ radiation, mimicking more common abdominal conditions.
Contrast-enhanced CT is crucial for accurate diagnosis, showing fat-density lesions and inflammatory stranding near the falciform ligament.
Conservative management with analgesia and supportive care effectively resolves symptoms without surgery.
Abstract
Falciform ligament appendagitis is an exceedingly rare cause of acute abdominal pain resulting from inflammation and infarction of the falciform ligament’s fatty appendage. Its presentation often mimics more common causes of acute abdomen, making diagnosis challenging. We report the case of a 36-year-old Bangladeshi male with no prior medical history who presented with a four-day history of severe epigastric pain radiating to the right upper quadrant (RUQ). Clinical examination revealed localized tenderness and a palpable soft, well-circumscribed swelling, with laboratory investigations within normal limits except for mild leukocytosis and a slightly elevated alanine aminotransferase (ALT). Initial ultrasound suggested a rectus sheath hematoma; however, contrast-enhanced CT imaging demonstrated a fat-density lesion adjacent to the falciform ligament with surrounding inflammatory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
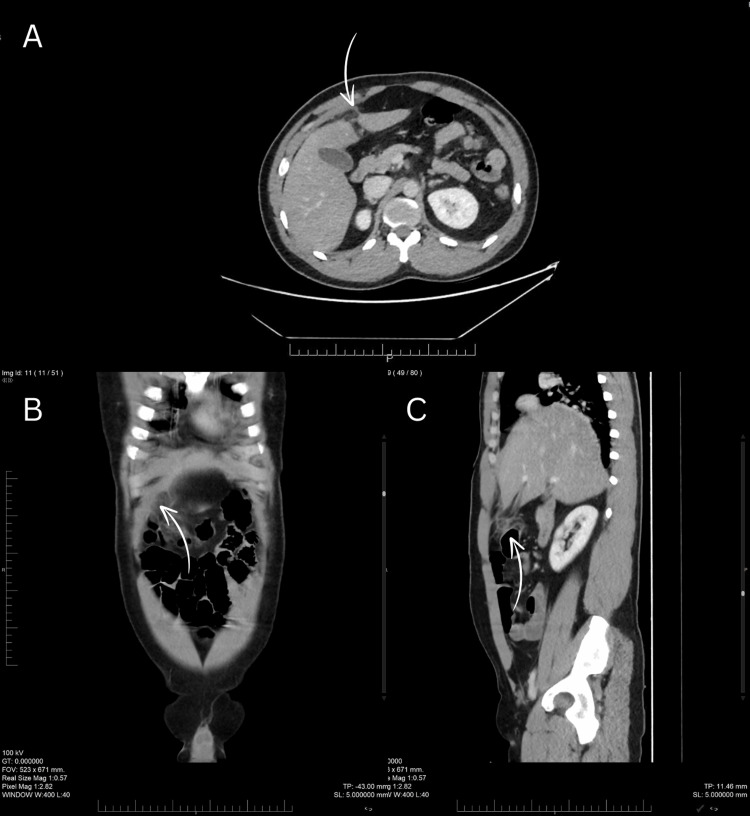 Figure 1
Figure 1| Parameter | Reference range | Day 1 | Day 4 |
| Complete blood count | |||
| Hemoglobin (g/dL) | 13.2-16.6 | 16.8 | 15.2 |
| Total red blood cell count (x1012/L) | 4.35-5.65 | 5.94 | 5.48 |
| Total leucocyte count (x109/L) | 3.4-9.6 | 10.24 | 7.80 |
| Platelet count (x109/L) | 150-400 | 295 | 266 |
| Biochemistry | |||
| Serum creatinine (µmol/L) | 65-104 | 78 | 79 |
| Serum urea (mmol/L) | 3.2-8.2 | 4.4 | 3.8 |
| Bilirubin (total) (µmol/L) | 5-21 | 19 | 17 |
| Alkaline phosphatase (U/L) | 56-116 | 77 | 73 |
| Electrolytes | |||
| Sodium (mmol/L) | 136-145 | 138 | 138 |
| Potassium (mmol/L) | 3.4-4.5 | 4.6 | 4 |
| Liver function test | |||
| Protein (total) (g/L) | 57-82 | 71 | 65 |
| Albumin (g/L) | 35-52 | 45 | 42 |
| Author(s) | Number of cases | Age group | Year | Imaging modality | Management |
| Rousslang et al. [ | 1 | Adult | 2020 | Ultrasound, CT | Conservative |
| Miura et al. [ | 2 | Adult | 2022 | Ultrasound, CT; Ultrasound, MRI | Conservative |
| Muleta et al. [ | 1 | Pediatric | 2024 | Ultrasound | Conservative |
| Chen et al. [ | 2 | Adult | 2024 | Ultrasound, CT, MRCP; CT | Conservative |
| Manso and Agostinho [ | 1 | Adult | 2024 | CT | Conservative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOmental and Epiploic Conditions · Intestinal and Peritoneal Adhesions · Case Reports on Hematomas
Introduction
The falciform ligament is a fold of peritoneum that separates the liver’s left and right lobes and connects to the anterior abdominal wall. It contains the ligamentum teres hepatis, the remnant of the umbilical vein, and adjacent extraperitoneal fat [1]. Falciform ligament appendagitis is a very rare condition involving inflammation and infarction of the fatty tissue adjacent to the falciform ligament, often presenting with severe abdominal pain that can mimic more common causes of acute abdomen [2]. Here, we report a 36-year-old man who presented with severe right upper quadrant (RUQ) abdominal pain, later confirmed by contrast-enhanced CT imaging as falciform ligament appendagitis.
Case presentation
A 36-year-old Bangladeshi male with no significant past medical history and no known drug allergies presented to the emergency department in July 2025 with a four-day history of severe epigastric pain radiating to the RUQ. The pain was constant and non-colicky, with no associated nausea, vomiting, changes in bowel or urinary habits, fever, or other constitutional symptoms. There was no previous history of similar pain, abdominal trauma, or recent heavy exertion.
On examination, the patient was alert, oriented, and hemodynamically stable. Vital signs were within normal limits, and he was afebrile. Abdominal examination revealed localized tenderness and mild guarding over the epigastric and RUQ regions, with a palpable soft, well-circumscribed swelling measuring approximately 3 × 4 cm. There was no distension, rebound tenderness, or other peritoneal signs. The remainder of the systemic examination was unremarkable.
Initial laboratory investigations showed a white blood cell count of 10.24 × 10^9^/L, hemoglobin 16.8 g/dL, and platelet count of 295 × 10^9^/L. Liver enzymes were within normal limits, except for a slightly elevated alanine aminotransferase (ALT) of 60 U/L. Other biochemical parameters were unremarkable. An ultrasound of the abdomen performed prior to admission suggested a possible rectus sheath hematoma; however, to further delineate the lesion, a contrast-enhanced CT scan of the abdomen was obtained. CT imaging demonstrated a fat-density, oval-shaped lesion adjacent to the falciform ligament with surrounding inflammatory stranding, consistent with falciform ligament appendagitis (Figure 1). No rectus sheath hematoma, gallbladder pathology, or intra-abdominal collection was identified.
Contrast-enhanced CT scan of the abdomen showing features suggestive of falciform ligament appendagitis.(A) Axial, (B) coronal, and (C) sagittal views demonstrate a fat-attenuated oval lesion with surrounding inflammatory changes adjacent to the falciform ligament (arrows).
The patient was admitted under the General Surgery department and managed conservatively. He was initially kept nil per os (NPO) and started on intravenous antibiotics, analgesia including paracetamol 1g every six hours and naproxen 250mg twice daily, and intravenous fluids. Daily laboratory monitoring and clinical assessments were performed.
On hospital day 2, the patient continued to report localized RUQ pain but remained afebrile and hemodynamically stable. Repeat physical examination showed persistent but improving tenderness without guarding or distension. Laboratory investigations were repeated, with results showing stable hemoglobin and platelet counts.
By hospital day 3, the patient’s condition had notably improved. He was pain-free at rest, tolerated clear fluids, and exhibited no new symptoms. Abdominal examination revealed only mild epigastric tenderness with no peritoneal signs. The patient was started on a regular diet, and his intravenous fluids were gradually reduced.
On hospital day 4, the patient was asymptomatic, and physical examination was completely normal. Repeat laboratory results showed a normalized WBC count of 7.8 × 10^9^/L, while hemoglobin (15.2 g/dL) and platelets (266 × 10^9^/L) remained within normal limits (Table 1). The patient was deemed clinically stable for discharge.
The patient showed complete clinical improvement during hospitalization and was discharged in stable condition. At the time of discharge, he was asymptomatic, tolerating oral intake, and did not require ongoing analgesia. No scheduled outpatient follow-up was arranged, and the patient was advised to return if symptoms recurred.
Discussion
The falciform ligament is a sagittal double fold of the peritoneum. It extends from the liver to the anterior abdominal wall. The left inferior phrenic and middle hepatic arteries provide the falciform ligament's primary blood supply. The falciform ligament serves as an excellent material for covering organ defects and repairing damaged surfaces within the abdominal cavity due to its extensive size, adequate length, rich blood supply, and well-developed vascular connections [3].
Fatty-falciform ligament appendage torsion (F-FLAT) is a rare condition caused by torsion of the extraperitoneal lipomatous appendage of the falciform ligament, leading to ischemia and aseptic fat necrosis. This results in falciform ligament appendagitis, an entity that clinically mimics other intraperitoneal focal fat infarctions (IFFIs) such as omental infarction and epiploic appendagitis, often making diagnosis challenging [2,4].
To date, only seven cases of falciform ligament appendagitis have been explicitly reported, highlighting the rarity of this condition. Within the spectrum of IFFI of the falciform ligament, few reports have specifically used the term "falciform ligament appendagitis" or "hepatic falciform ligament appendagitis." A focused review of peer-reviewed case reports identified seven previously reported patients meeting this terminology (Table 2). Our case, therefore, represents the eighth reported patient diagnosed with falciform ligament appendagitis using this specific label. Additional cases with similar pathology have been published under alternative terms, such as "torsion of a fatty appendage of the falciform ligament," "falciform ligament fat infarction," or "fat necrosis/inflammation of the falciform ligament"; however, these were not included in this count, as they do not explicitly mention appendagitis in the title or abstract.
Falciform ligament appendagitis occurs slightly more often in males than in females, with an almost equal sex ratio (approximately 1:1) and a median age of around 59.5 years. The only reported risk factor is obesity, particularly an increase in abdominal visceral fat, although available data remain limited [9]. Other falciform ligament pathologies include internal herniation through congenital defects, as well as congenital, infectious, or neoplastic cysts and lipomas. In some cases, isolated necrosis of the falciform ligament may occur without any associated abnormalities [10].
Clinically, patients typically present with RUQ or epigastric pain that is usually non-radiating, accompanied by low-grade fever and leukocytosis [5,9]. Ultrasound can help locate and identify the lesion through real-time dynamic assessment with the patient. Using a high-frequency probe may further enhance diagnostic accuracy when FLA is suspected; however, it is insufficient for distinguishing between different possible causes [6,11].
CT imaging is crucial for accurately diagnosing gastroduodenal and pancreatic conditions, as well as rare mimicking entities such as IFFI [11]. It typically demonstrates falciform ligament appendagitis as a focal, well-defined area of fat attenuation adjacent to the falciform ligament, surrounded by a thin hyperattenuating rim, with or without a central dot representing a thrombosed draining vein [6]. MRI may also detect the lesion, typically appearing as a fat-signal area with surrounding inflammation, but its role is secondary compared to CT [12].
Falciform ligament appendagitis is a self-limiting condition that typically resolves within three to 14 days with conservative management, without the need for surgical intervention. Very rare complications may include adhesion formation, peritonitis, abscess development, or calcified peritoneal loose bodies [1,10]. A few reported cases underwent surgery, mainly because of limited awareness of the condition and its typically self-limiting course. Another indication for laparotomy was the concern for necrosis and gangrene, as documented in some reports [13,14].
Conclusions
Falciform ligament appendagitis is a rare but self-limiting cause of acute RUQ pain that can be accurately diagnosed with CT imaging, allowing safe conservative management and avoiding unnecessary surgical approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torsion of the fatty appendage of the falciform ligament Radiol Case Rep Smeeing DP Bernsen ML 435543571720223618808210.1016/j.radcr.2022.08.050PMC 9520422 · doi ↗ · pubmed ↗
- 2A case report of falciform ligament appendagitis Cureus Manso M Agostinho L 016202410.7759/cureus.51965 PMC 1085299638333502 · doi ↗ · pubmed ↗
- 3Anatomical study on the morphology and blood supply of the falciform ligament and its clinical significance Surg Radiol Anat Li XP Xu DC Tan HY Li CL 1061092620041458656410.1007/s 00276-003-0184-0 · doi ↗ · pubmed ↗
- 4Fatty-falciform ligament appendage torsion (F-FLAT): diagnosis and management in a pediatric patient Radiol Case Rep Horak RD Mega JD Tanton PJ Criman ET Tabak BD Rooks VJ 1811851520203189006410.1016/j.radcr.2019.11.004PMC 6923463 · doi ↗ · pubmed ↗
- 5Falciform ligament appendagitis after Roux-en-Y bypass surgery mimicking acute cholecystitis BMJ Case Rep Rousslang LK Mc Coy MF Gould CF 23564213202010.1136/bcr-2020-235642 PMC 743788032816881 · doi ↗ · pubmed ↗
- 6Hepatic falciform ligament appendagitis evaluated by ultrasound: a report of 2 cases Radiol Case Rep Miura D Shindo M Fukuda Y 442544301720223618809310.1016/j.radcr.2022.08.090PMC 9520509 · doi ↗ · pubmed ↗
- 7An uncommon cause of epigastric pain in a child: falciform ligament appendigitis Radiol Case Rep Muleta RT Kassa NB Alamneh TT 643364351920243938080910.1016/j.radcr.2024.09.047PMC 11460365 · doi ↗ · pubmed ↗
- 8Intraperitoneal focal fat infarction of the falciform ligament: a report of two cases UCLA Radiol Sci Proc Chen M Pahwa A Beckett K 42024