Comparative Efficacy of Two‐Session Radiofrequency Ablation Versus Transarterial Embolization Followed by Radiofrequency Ablation for the Treatment of Large Benign Thyroid Nodules
Cheng-Kang Wang, Yueh-Sheng Chen, Chen-Kai Chou, Wei-Chih Chen, Yuan-Pin Lin, An-Ni Lin, Chih-Ying Lee, Sheng-Dean Luo, Wei-Che Lin

TL;DR
This study compares two treatments for large benign thyroid nodules and finds that combining embolization with radiofrequency ablation may be more effective.
Contribution
The study provides a direct comparison of two treatment approaches for large benign thyroid nodules using propensity score matching.
Findings
The TAE/RFA group showed a higher daily volume reduction rate compared to the double-session RFA group.
TAE/RFA resulted in a larger pretreatment nodule volume and greater overall volume reduction.
The study suggests TAE combined with RFA is a more effective treatment for large benign thyroid nodules.
Abstract
To treat large benign thyroid nodules (BTNs), radiofrequency ablation (RFA) and transarterial embolization (TAE) combined with RFA are both used. This study aimed to compare the effectiveness of both treatments. Nineteen subjects with 20 BTNs received two sessions of RFA, while eight patients with 10 BTNs underwent TAE followed by RFA in a single medical center. Propensity score matching (PSM) was utilized to control for inherent potential biases by matching similar characteristics between the two groups. Prior to treatment, a larger median nodule volume was observed in the TAE with the RFA group (150.75 ± 202.61 mL) compared to that of the double‐session RFA group (81.44 ± 58.00 mL). The volume reduction ratio (VRR) was found to be 74.60 ± 14.49% in the TAE/RFA group and 83.93 ± 12.70% in the double‐session RFA group. To account for follow‐up duration, we calculated the variation of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
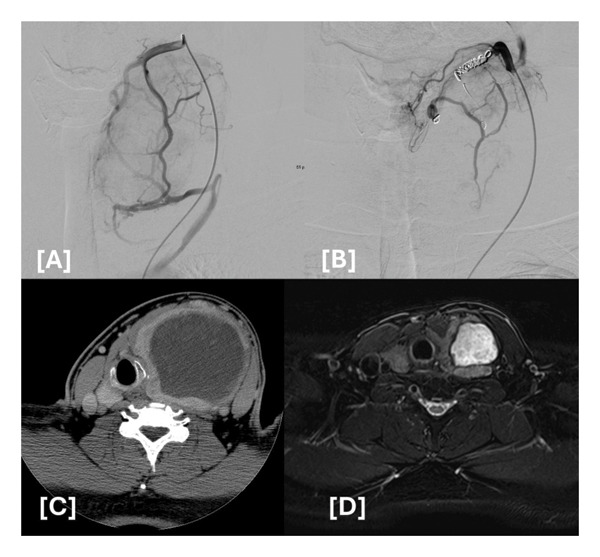 Figure 1
Figure 1|
|
|
| |
| Subjects | 19 | 8 | |
| Nodules | 20 | 10 | |
| Gender (F:M) | 16:3 | 7:1 | 0.455 |
| Age | 42.20 ± 9.29 | 47.00 ± 12.57 | 0.859 |
| T3 (ng/dL) pre | 103.78 ± 22.86 | 107.47 ± 64.96 | 0.055 |
| Free T4 (μg/dL) pre | 1.19 ± 0.14 | 1.21 ± 0.49 | 0.413 |
| TSH (μIU/mL) pre | 1.16 ± 0.65 | 0.79 ± 0.52 | 0.508 |
| Prevolume (mL) | 81.44 ± 58.00 | 150.75 ± 202.61 | 0.026 |
| Postvolume 1st RFA (mL) | 39.77 ± 40.42 | ||
| Postvolumetotal (mL) | 14.13 ± 13.89 | 32.35 ± 36.64 | 0.010 |
| VRR (%) post 1st RFA | 54.07 ± 19.50 | ||
| VRR (%)total | 83.93 ± 12.70 | 74.60 ± 14.49 | 0.413 |
| Δtime (days) | 170.60 ± 149.70 | ||
| Δtimetotal (days) | 733.80 ± 319.54 | 446.80 ± 87.26 | 0.001 |
| ΔVRR/Δtimetotal (%/days) | 0.13 ± 0.05 | 0.17 ± 0.05 | 0.040 |
| T3 (ng/dL) post | 88.07 ± 12.78 | 87.68 ± 11.45 | 0.392 |
| Free T4 (μg/dL) post | 1.10 ± 0.23 | 0.99 ± 0.23 | 0.705 |
| TSH (μIU/mL) post | 1.70 ± 0.87 | 1.42 ± 0.78 | 0.997 |
| kcal/mL | 0.30 ± 0.14 | 0.24 ± 0.18 | 0.773 |
| J/mL | 1271.11 ± 611.34 | 997.04 ± 768.45 | 0.773 |
| Patient no. | Age | Gender | Thyroid nodules | Prevolume | Intrathoracic extension | Time between double RFA in days |
|---|---|---|---|---|---|---|
| 1 | 43 | F | Predominantly solid | 56.91 | Grade 1 Type A | 374 |
| 2 | 45 | F | Predominantly solid | 30.13 | No | 296 |
| 3 | 25 | F | Predominantly solid | 72.06 | No | 217 |
| 4 | 37 | F | Predominantly solid | 148.96 | Grade 2 Type B | 112 |
| 5 | 38 | F | Solid | 30.01 | Grade 1 Type A | 497 |
| 6 | 35 | F | Solid | 68.21 | Grade 2 Type B | 365 |
| 7–1 | 42 | F | Predominantly solid (right) | 39.86 | No | 304 |
| 7–2 | 42 | F | Predominantly solid (left) | 30.06 | No | 119 |
| 8 | 66 | M | Predominantly solid | 251.98 | Grade 2 | 191 |
| 9 | 37 | F | Solid | 173.27 | Grade 2 Type B | 210 |
| 10 | 38 | F | Predominantly solid | 101.82 | Grade 2 Type B | 383 |
| 11 | 58 | F | Solid | 55.41 | Grade 3 Type C | 142 |
| 12 | 47 | M | Predominantly solid | 76.69 | Grade 1 Type A | 896 |
| 13 | 44 | F | Solid | 138.45 | Grade 1 Type B | 222 |
| 14 | 41 | F | Solid | 79.52 | Grade 1 Type A | 209 |
| 15 | 42 | F | Solid | 47.4 | Grade 1 Type A | 828 |
| 16 | 54 | M | Solid | 37.25 | Grade 1 Type A | 479 |
| 17 | 39 | F | Predominantly solid | 53.65 | No | 534 |
| 18 | 43 | F | Solid | 82.87 | Grade 1 Type A | 317 |
| 19 | 28 | F | Solid | 80.73 | Grade 1 Type A | 289 |
| Patient no. | Age | Gender | Thyroid nodules | Prevolume | Intrathoracic extension | Time between TAE and RFA in days |
|---|---|---|---|---|---|---|
| 1 | 39 | M | Predominantly cystic | 698.39 | Grade 1 Type A | 0 |
| 2 | 81 | F | Solid | 158.69 | Grade 2 Type C | 1 |
| 3 | 37 | F | Solid | 30.12 | Grade 1 Type A | 0 |
| 4 | 43 | F | Solid | 87.13 | Grade 1 Type A | 0 |
| 5 | 46 | F | Predominantly solid | 34.82 | Grade 1 Type A | 0 |
| 6 | 38 | F | Predominantly solid | 39.13 | No | 122 |
| 7 | 45 | F | Predominantly solid | 223.75 | Grade 1 Type A | 73 |
| 8–1 | 47 | F | Predominantly solid (isthmus) | 129.91 | Grade 1 Type A | 207 |
| 8–2 | 47 | F | Solid (right) | 55.91 | No | 207 |
| 8–3 | 47 | F | Solid (left) | 50.13 | No | 207 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid and Parathyroid Surgery · Management of metastatic bone disease
Key Points
- •Double‐session RFA and TAE are both therapeutic modalities for the treatment of large benign thyroid nodules.
- •The group of TAE combined with RFA exhibited a relatively higher median daily VRR after treatment.
- •TAE followed by RFA may be more effective for the treatment of large benign thyroid nodules than two sessions of RFA.
1. Introduction
Thyroid nodules are among the most common clinical findings in the general population, with prevalence estimates ranging from 16% to 67% depending on the detection methods and demographic characteristics of the population studied [1]. Their occurrence increases significantly with advancing age, female sex, and prior exposure to ionizing radiation [1]. In Taiwan, ultrasound‐based population studies have reported a prevalence of approximately 16%–19%, consistent with rates observed worldwide [1]. Although the majority of thyroid nodules (around 90%–95%) are benign, distinguishing benign from malignant nodules remains a crucial clinical challenge [1].
Benign thyroid nodules (BTNs) require intervention when they produce symptomatic compression such as airway narrowing, dysphagia, or neck discomfort, when cosmetic concerns adversely affect quality of life, when intrathoracic extension (intrathoracic goiter, ITG) causes functional limitation, or when progressive growth is documented [1, 2]. Surgery has long been considered the standard treatment for symptomatic BTNs, but it carries potential risks, including permanent hypoparathyroidism, recurrent laryngeal nerve injury, and general anesthesia‐related morbidity [1].
Management becomes more complex for large BTNs, typically defined as those with a volume > 30 mL or a maximal diameter > 4 cm. These nodules show higher rates of regrowth or incomplete treatment response compared with smaller nodules [1]. When extending into the mediastinum as ITGs, surgical management may require extracervical approaches such as manubriotomy or thoracotomy, further increasing procedural risks [2–4]. Additionally, a considerable proportion of patients decline surgery or are deemed medically ineligible due to advanced age or cardiopulmonary comorbidities [1, 5].
Several previous studies have reported on the efficacy of transarterial embolization (TAE) as applied in the treatment of nodular goiters, Graves’ disease, and hyperthyroidism [6–8]. Selective embolization of thyroid arteries has an outcome similar to a surgical subtotal thyroidectomy [9], while exhibiting a lower complication rate and an acceptable VRR as compared to RFA [6].
While the clinical effectiveness of both RFA and TAE in the treatment of BTNs has been demonstrated in separate studies, there is currently a lack of literature directly comparing the therapeutic efficacy of these two approaches when RFA is combined with TAE versus applied as multiple sessions alone [1]. This knowledge gap is particularly important for very large benign nodules, where achievement of satisfactory treatment response remains challenging and treatment failure rates are higher.
Therefore, we undertook this retrospective study to compare the effectiveness and safety of two treatment approaches for large BTNs: (1) two‐session RFA and (2) combined TAE followed by RFA. We aimed to evaluate the comparative therapeutic efficacy, safety profiles, and patient outcomes between these two treatment modalities in patients with large BTNs who were unsuitable for or refused surgical intervention.
2. Patients and Methods
The institutional review board of the Chang Gung Memorial Hospital approved this retrospective study, and informed consent was obtained from all patients prior to the RFA and TAE procedures. All subjects received two separate fine‐needle aspiration (FNA) or core‐needle biopsy (CNB) procedures in different parts of the thyroid lesions to confirm the benign nature of the thyroid nodules. There were no suspicious malignant features on US examination, including hypoechoic taller‐than‐wide shape, or ill‐defined margins. Two radiologists experienced in the thyroid RFA field reviewed the images.
The inclusion criteria for this study were as follows: (1) a large thyroid nodule volume (> 30 mL); (2) a maximum diameter of the thyroid nodule > 4 cm; (3) serum thyroid hormone, thyroid‐stimulating hormone (TSH), and thyroglobulin levels within normal ranges; (4) follow‐up period ≥ 6 months after RFA or TAE; and (5) patients who refused surgery. The exclusion criteria were as follows: (1) biopsy results showing follicular neoplasm or malignancy; (2) suspicious malignant features on ultrasonography even with a benign biopsy result; (3) coagulation disorder, contrast medium allergy, or other contraindications of angiography. Due to the relatively high risk of recurrence or regrowth, and intrathoracic extension, we recommended patients undergo two sessions of RFA or TAE procedure combined with RFA to downgrade the level of BTN during the initial RFA or TAE procedure. We then ablated the majority of BTNs in the subsequent RFA to achieve a better VRR. All patients were informed as to the risks and benefits associated with the RFA, TAE, and surgical procedures. A majority of patients refused surgery, while others were not suitable surgical candidates due to the underlying disease. There was a shared decision‐making process, which was well documented during which time patients were encouraged to sufficiently deliberate and express their opinions during the discussions.
A total of 27 patients presenting with 30 BTNs who underwent procedures at our institution between March 2017 and March 2021 were retrospectively enrolled in this study. Among them, 19 patients with 20 nodules who underwent two sessions of RFA at separate times were included in Group 1, and 8 patients with 10 nodules who received TAE with subsequent RFA were in Group 2.
2.1. Pretreatment Assessment
All the patients underwent the pretreatment assessments at the outpatient service of the departments of endocrinology, otolaryngology, thyroid interventional radiology, or surgery. The thyroid function tests included triiodothyronine (T3), free thyroxine (fT4), and TSH. In addition, US study combined with computed tomography (CT), or magnetic resonance imaging (MRI) was used to determine the size, echogenicity, margin, shape, component, calcification, location, and the level of intrathoracic extension. The nodular volume was calculated using the following equation: V = πabc/6 (V: volume; a: the largest diameter; b and c: the other double perpendicular diameters).
2.2. Radiofrequency Ablation
Prior to the ablation procedures, patients in the RFA group were informed of the requirement for two sessions of RFA to achieve a better VRR due to the relatively large nodular volume. The ablation procedures were performed by a radiologist with over 15 years of experience in US‐guided procedures. Each RFA procedure was performed with an RF generator (VIVA, STARmed and M2004, RF Medical) with an internally cooled electrode (18 gauge, with 10, 7, or 5‐mm active tip), the size of which was based on the nodular size and the status of the surrounding critical structures. The RFA procedures were performed using a trans‐isthmic approach, with hydrodissection and the moving‐shot technique. When all visual fields of the nodule had changed to transient hyperechoic zones, the ablation procedure was terminated.
2.3. TAE Combined With RFA
All TAE procedures were performed using the right femoral arterial approach with a 5‐F sheath. A catheter was advanced over a hydrophilic guide wire, and the nodular‐side superior and inferior thyroid arteries were selectively catheterized, identifying the thyroid arteries that fed the nodule (s). After a 2.7‐F microcatheter was selectively advanced into the major branches of the thyroid arteries and placed in a secure position, the artery was embolized with 300–500‐μm Embosphere microspheres until a decreased blood flow was observed. To ensure optimal embolization, the proximal part of the feeding arteries was occluded with coils. Based on the angiography results, embolization of the nodular‐side superior and inferior thyroid arteries was performed. Preservation of one inferior thyroid artery was considered to avoid the potential risk of hypoparathyroidism if a patient presented with bilateral thyroid nodules. The procedure was considered completed when the target arteries were optimally embolized. Some patients received subsequent RFA on the same day, while others received RFA several months later, depending on the level of intrathoracic extension and nodular components. After the TAE procedure, patients were observed overnight to monitor for potential complications, including airway compression and thyroid storm.
2.4. Follow‐Up Evaluations
Post‐treatment follow‐up US at 1, 3, 6, and 12 months were performed to evaluate the VRR. The VRR was assessed by medical imaging and was calculated by the following equation: volume reduction ratio (%) = initial volume (mL) − final volume (mL) × 100/initial volume. The vascularity of the ablated nodules, and cosmetic score and symptomatic scores were also evaluated at each follow‐up. A follow‐up contrast‐enhanced CT or MRI examination was performed at 6 months after the procedure to establish the thyroid gland volume. The serum levels of T3, fT4, and TSH were measured prior to the procedures and at 6 months. To evaluate the different treatment outcomes by considering the time factor, the imaging follow‐up interval between the RFA or TAE procedure and CT or MRI imaging study is represented as Δtime.
2.5. Analyses and Statistics
Statistical analyses were performed by using SPSS, version 26 (SPSS, Inc., Chicago, IL, USA). All data are given as the mean ± standard deviation (SD). Demographic characteristics, ultrasound, CT, or MRI results between the double groups were compared. Standard chi‐squared and Fisher’s exact tests were used for group comparisons of the categorical data. Group comparisons for the continuous variable data were performed by using the Mann–Whitney U test and the Kruskal–Wallis test (SPSS, Inc., Chicago, IL, USA).
We used R (R Core Team, 2014) to demonstrate propensity score matching (PSM) and propensity score weighting (PSW) in a regression model. To control for inherent potential biases, the one‐to‐one PSM by using the nearest‐neighbor matching method was applied to the two groups based on age, sex, largest diameter, volume, and follow‐up period. PSW with inverse probability of treatment weighting (IPTW) and standardized mortality ratio weighting (SMRW) were also performed to control for the influence of participants by weighting their responses based on their propensity scores. Average treatment effect on the treated (ATT) is an evaluator of PSW, which is the difference in the outcome variable between the average score for the two groups. Patient characteristics and outcomes were compared between the two groups both before and after matching. A 2‐sided p < 0.05 was considered as statistically significant.
3. Results
The demographic data of the two groups are shown in Table 1. There were 19 subjects with 20 BTNs included in the group of double‐session RFA group and 8 patients with 10 BTNs included in the TAE with the RFA group. There were no differences in age and sex distribution between the two groups. The thyroid functions between the two groups were within normal ranges.
3.1. Group 1: Double‐Session RFA
The double‐session RFA group data are shown in Tables 1 and 2. The mean pretreatment nodular volume was 81.44 ± 58.00 mL, while the average residual volume of the thyroid nodules was about 39.77 ± 40.42 mL. The mean VRR was 54.07 ± 19.50% after the first RFA. The mean interval between the first and the second RFA was 347.55 ± 206.24 days (ranging from 111 to 881 days). After the second RFA procedure, the median residual volume of the ablated nodules was 14.13 ± 13.89 mL, while VRR was 83.93 ± 12.70%. The medical imaging interval was 733.80 ± 319.54 days between the two RFA sessions. The mean daily VRR was 0.13 ± 0.05%/day, indicating an approximately 0.13% daily volume reduction ratio after the ablation treatment.
3.2. Group 2: TAE With RFA
The data for the TAE combined with the RFA group are shown in Tables 1 and 3. The median pretreatment nodular volume was 150.75 ± 202.61 mL, and the residual volume of the thyroid nodules was 32.35 ± 36.64 mL. The median VRR was 74.60 ± 14.49%. The median interval between the TAE and RFA procedures was 81.30 ± 95.29 days (ranging from 0 to 207 days). Significantly larger residual thyroid lesions were noted in the TAE with the RFA group as compared to that of the double‐session RFA group. The median medical imaging interval is 446.80 ± 87.26 days between the pretreatment assessment and the completed TAE with RFA treatments. The median daily VRR was 0.17 ± 0.05%/day. After treatment, thyroid functions were within normal range in both groups, with no significant difference. The energy delivered per nodular volume is considered a major factor affecting the VRR after RFA [5]. As such, the median RFA energy delivered was 1271.11 ± 611.34 J/mL (0.30 ± 0.14 kcal/mL) in the double‐session RFA group and was 997.04 ± 768.45 J/mL (0.24 ± 0.18 kcal/mL) in the TAE with the RFA group, indicating no significant difference in terms of RFA energy delivered between the two groups.
There were no major complications in both groups, such as permanent voice change, delayed rupture, or stroke. The most common complication among patients in both groups was pain and swelling, which were relieved within 1 week of the procedures.
4. PSM
To control for potential biases, propensity scores were used as weights to account for selection assignment differences between the two groups. Several variates, including the number of subjects, age, pre‐ and post‐treatment volumes, VRR, ΔVRR/Δtime, and J/mL, were analyzed in PSM and PSW. The one‐to‐one PSM by using the nearest‐neighbor matching method was applied with calipers of 0.2, 0.3, and 2.5, while the number of subjects was 8, 9, and 10, respectively, as shown in Supporting Table 1. The two different methods of PSW, IPTW, and SMRW are shown in Supporting Table 2. After the IPTW analysis, the number of subjects was 29.72 in the double‐session RFA group and 29.96 in the TAE with the RFA group. And after SMRW analysis, the number of subjects was 20.00 in the double‐session RFA group and 19.96 in the TAE with the RFA group. The median VRR together with the time factor was more notable in the TAE with the RFA group than the double‐session RFA group, although there was no significant difference in all variates after applying PSM and PSW analyses.
5. Discussion
The present study of patients with large BTNs treated by two RFA sessions or TAE combined with RFA demonstrates that both therapeutic modalities achieved a satisfactory VRR, with a mean volume reduction of 74% in the TAE with the RFA group and 83% in the double‐session RFA group. The preprocedural assessment revealed a larger average nodular volume in the TAE group as compared to that in the double‐session RFA group; hence, a relatively higher nodular volume reduction in the TAE group would be expected, accompanied by a lower VRR as compared to that in the double‐session RFA group. According to previous studies, a single session of RFA is less effective for BTNs with a volume of > 30 mL than for smaller BTNs [1]. Thus, for patients with large BTNs who refuse surgery, a single session of RFA may not be expected to achieve an acceptable VRR, suggesting that TAE would be a more effective treatment.
Multiple sessions of RFA can be effective in reducing the volume of large BTNs. In our study, the shortest interval between RFA sessions was 6 months, as the effect of the initial RFA will generally persist for at least this amount of time. In cases of the maximum diameter of a large BTN is > 5 cm and with a volume > 30 mL, more than a single session of RFA should be considered to achieve a satisfactory VRR. In this regard, a down‐staging procedure is a valuable step in a multisession RFA. For ITGs, the initial RFA can act to reduce the ITG grade, facilitating subsequent RFA procedures to achieve a better VRR. As there is a higher complication rate among large BTNs [1], multiple sessions of RFA are a strategy applied to reduce the risk of voice change, delayed rupture, and other complications.
TAE combined with RFA was used to treat patients presenting with large BTNs in this study. Among this group of patients, the average pretreatment nodular volume was significantly higher than that of the double‐session RFA group. Previous studies have indicated that TAE is a more effective treatment modality than traditional thermal ablation for large nodules [6, 10, 11]. In our study, 5 patients underwent TAE and RFA in the same day, while these BTNs were defined as mixed solid and cyst, or hemorrhagic cysts. To effectively decrease vascularity, TAE was performed with 300–500 μm Embosphere microspheres until optimal stasis was achieved followed by coils. For BTNs with a cystic component, TAE was introduced initially to control vascularity and possibly prevent hemorrhage during the ablation procedure, while the subsequent RFA procedure could focus on the solid section of the nodule (Figure 1). The other three patients received the two procedures with an interval of between 2 and 6 months. Of these patients, two had predominantly solid thyroid nodules, while one patient presented with three large predominantly solid nodules. These patients underwent the RFA procedure after a period of time to avoid postembolization compression of the trachea due to a large solid nodule component. Of note, TAE acts as a downgrading procedure for large BTNs. The initial TAE procedure serves to embolize the inferior thyroid arteries, which supply the intrathoracic part of large BTNs, allowing for the subsequent RFA procedure to effectively ablate the residual sections of BTNs.
Patient one of the TAE with the RFA group. (A) Diagnostic angiography before embolization. (B) Post‐TAE with embosphere followed by coil embolization. (C) CT study before TAE. (D) MRI study at a 6‐month follow‐up post TAE with RFA.
In our procedural analysis, we used the PSM by matching each treated unit with a nontreated unit with similar characteristics among the two groups. Among three different caliper distances, there was no significant difference in age and pretreatment volume between the two groups; however, the TAE with the RFA group exhibited a relatively larger pretreatment volume. Additionally, IPTW and SMRW using the propensity score apply weights based on the propensity score to create a synthetic sample in which the distribution of measured baseline covariates is independent of treatment assignment. Although there remained no significant difference in terms of post‐treatment volume, VRR, and ΔVRR/Δtime, several trends were revealed in the results. More specifically, we noted a higher absolute reduced nodular volume in the TAE with the RFA group than the double‐session RFA groups due to the larger pretreatment nodular volume. The TAE with the RFA group also exhibited a relatively higher median daily VRR after treatment. These results indicate that TAE or TAE combined with RFA may be more effective than multiple sessions of RFA to treat large BTNs.
There are several limitations to this study. First, as this was a retrospective single‐center study, uncontrolled bias could have been introduced. Further prospective study or randomized controlled study is required to validate our results. Second, the sample size of the two groups was too small, although PSM was used to mimic some of the characteristics of a randomized controlled trial. Third, the long‐term outcomes of the two groups should be determined by continued follow‐up. Finally, a separate study should be conducted to compare the effectiveness of the TAE combined with RFA treatment with that of pure TAE treatment.
In conclusion, our study indicates that TAE combined with RFA showed a potential benefit in volume reduction for large BTNs compared to two‐session RFA, though further studies are required to confirm this finding. As an initial down‐staging procedure, TAE can act to effectively reduce a greater nodular volume without the risk of major complications. The findings may assist physicians to better inform the decision‐making process when discussing the various treatment options available to patients presenting with large BTNs.
NomenclatureUSUltrasoundRFARadiofrequency ablationTAETransarterial embolizationBTNsBenign thyroid nodulesVRRVolume reduction ratioITGIntrathoracic goiterFNAFine‐needle aspirationCNBCore‐needle biopsyT3TriiodothyroninefT4free thyroxineTSHThyroid‐stimulating hormoneCTComputed tomographyMRIMagnetic resonance imagingPSMPropensity score matchingPSWPropensity score weightingIPTWInverse probability of treatment weightingSMRWStandardized mortality ratio weightingATTAverage treatment effect on the treated
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this manuscript.
Supporting Information
Supporting Table 1: Clinical characteristics and treatment factors of the two groups with propensity score matching (PSM) (1:1).
Supporting Table 2: Clinical characteristics and treatment factors of the two groups with propensity score weighting.
IPTW: inverse probability of treatment weighting.
SMRW: standardized mortality ratio (SMR) weighting.
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin W. C. , Wang C. K. , Wang W. H. et al., Multicenter Study of Benign Thyroid Nodules With Radiofrequency Ablation: Results of 762 Cases Over 4 Years in Taiwan, Journal of Personalized Medicine. (2022) 12, no. 1, 10.3390/jpm 12010063.PMC 878202535055378 · doi ↗ · pubmed ↗
- 2Di Crescenzo V. , Vitale M. , Valvano L. et al., Surgical Management of Cervico-Mediastinal Goiters: Our Experience and Review of the Literature, International Journal of Surgery. (2016) 28, no. Suppl 1, S 47–S 53, 10.1016/j.ijsu.2015.12.048, 2-s 2.0-84951971548.26721191 · doi ↗ · pubmed ↗
- 3Khairy G. A. , Al-Saif A. A. , Alnassar S. A. et al., Surgical Management of Retrosternal Goiter: Local Experience at a University Hospital, Annals of Thoracic Medicine. (2012) 7, no. 2, 57–60, 10.4103/1817-1737.94520, 2-s 2.0-84859752576.22558008 PMC 3339204 · doi ↗ · pubmed ↗
- 4Hegedus L. and Bonnema S. J. , Approach to Management of the Patient With Primary or Secondary Intrathoracic Goiter, Journal of Clinical Endocrinology and Metabolism. (2010) 95, no. 12, 5155–5162, 10.1210/jc.2010-1638, 2-s 2.0-78650055204.21131536 · doi ↗ · pubmed ↗
- 5Lim H. K. , Lee J. H. , Ha E. J. , Sung J. Y. , Kim J. K. , and Baek J. H. , Radiofrequency Ablation of Benign Non-Functioning Thyroid Nodules: 4-Year Follow-Up Results for 111 Patients, European Radiology. (2013) 23, no. 4, 1044–1049, 10.1007/s 00330-012-2671-3, 2-s 2.0-84878589826.23096937 · doi ↗ · pubmed ↗
- 6Yilmaz S. , Habibi H. A. , Yildiz A. , and Altunbas H. , Thyroid Embolization for Nonsurgical Treatment of Nodular Goiter: A Single-Center Experience in 56 Consecutive Patients, Journal of Vascular and Interventional Radiology. (2021) 32, no. 10, 1449–1456, 10.1016/j.jvir.2021.06.025.34256121 · doi ↗ · pubmed ↗
- 7Zhao W. , Gao B.-L. , Yang H.-Y. et al., Thyroid Arterial Embolization to Treat Graves’ Disease, Acta Radiologica. (March 2007) 48, no. 2, 186–192, 10.1080/02841850601128967, 2-s 2.0-33947152944.17354140 · doi ↗ · pubmed ↗
- 8Lima J. , Souza A. , Mendonça R. et al., Thyroid Arterial Embolization as a Therapeutic Option for Hyperthyroidism: A Case Series, Radiologia Brasileira. (March/April 2013) 46, no. 2, 83–88.